Paper Menu >>
Journal Menu >>
 Vol.1, No.3, 173-175 (2009) Health doi:10.4236/health.2009.13028 SciRes Copyright © 2009 Openly accessible at http://www.scirp.org/journal/HEALTH/ Study on regurgitation of a bearing-less mini axial aortic valvo-pump with closed impeller Kun-Xi Qian Institute of Biomedical Engineering, Jiangsu University, Jiangsu, Zhenjiang, China Received 5 May 5 2009; revised 13 July 2009; accepted 15 July 2009. ABSTRACT The back-flow of an aortic valvo-pump will re- duce the pumping flow rate but can wash out the gap between the rotor and the stator, and thus can improve the antithrombogenicity of the de- vice. To investigate the regurgitation of a 23mm OD aortic valvo-pump, its closed impeller was replaced by a cylinder and hereby the valvo- pump had lost its pumping function. The pres- sure head crossing the aortic valvo-pump was maintained by a locally made pulsatile centrifugal pump, beating rhythmically from 30 to 120mmHg. The back flow from outlet to inlet of valvo-pump via the above-mentioned gap was measured. Results demonstrated that this gap and the pressure head had remarkable effect on back- flow; a larger gap and/or a larger pressure head would lead to a larger back-flow. By 0,20mm gap and 100mmHg pressure head, the valvo-pump had ca. 0,8 l/min back-flow. Instantaneous meas- urement indicated that the back-flow had a pul- satile form with high rate during diastole while low rate during systole of the natural heart imi- tated by pulsatile centrifugal pump. The pump rotated at 12500rpm, 15000rpm and 17500rpm respectively, but it was found the rotating speed had no affection on back-flow. This investigation provides a basis for pump design seeking for both increase of the flow rate and improvement of the compatibility; the former is particularly important for a mini axial pump and the latter is extremely difficult for closed impeller. Keywords: Aortic Valvo-Pump; Regurgitation Measurement; Different Air-Gap and Pressure Head; Anti-Thrombogenicity 1. INTRODUCTION For long-term left ventricular assist, aortic valvo-pumps were developed [1-4,8], which deliver the blood directly from ventricle to aorta without connecting tubes and bypass circle, thus have less dangers of thrombus forma- tion outside the pump. In the inside of the pump, regur- gitation can wash out the blood contacting surfaces in the gap between the rotor and the stator and can prevent the formation of micro-thrombus thereafter. Regurgitation will reduce the pumping flow rate, however, it is signifi- cant therefore to control the back-flow rate to a certain range by measuring the back-flow and investigating the factors affecting the back-flow. 2. METHOD Figure 1 is a schematic drawing of an aortic valvo-pump with 23 mm outer diameter, in which the impeller is re- placed by a cylinder. That means the pump has no func- tion to propeller the fluid from right (inlet) to left (outlet). Therefore, the flow in the system is only the back-flow across the gap between the stator and the rotor, and the flow rate can be easily measured by flow meter. If there is a pressure head, namely, a pressure difference between the outlet and inlet of the device, there will be a flow from outlet to inlet via the air-gap as shown in Figure 1. The air-gap “S” in Figure 1 between the motor coil and rotor magnets was made into 0,1mm, 0,2mm and 0,3mm re- spectively. The pressure head between outlet and inlet of the aortic valvo-pump was produced to being pulsatile between 30mmHg~120mmHg by a locally made pulsa- tile centrifugal pump [5-7] (Figure 2). The valvo-pump without impeller rotated at 15,000rpm, 17,500rpm and 20,000rpm respectively, in order to compare the back- flow rate at the different rotating speeds, so as to show the effect of the rotating speed on back-flow of the aortic valvo-pump. The back-flow was measured by an Ameri- can Transonic T110 flow meter; the outlet pressure and inlet pressure were measured by HP 1205A manometer. Then the pressure difference between the outlet and the inlet of the pump was calculated and diagrammed to- gether with the back-flow value in Figures 3-5. Finally, the instantaneous back-flow curve was obtained and the relation between the back-flow and the natural heart Presented partly at the IEEE Conference on Biomedical Engineering and informatics. May 2008, Shanghai, China. 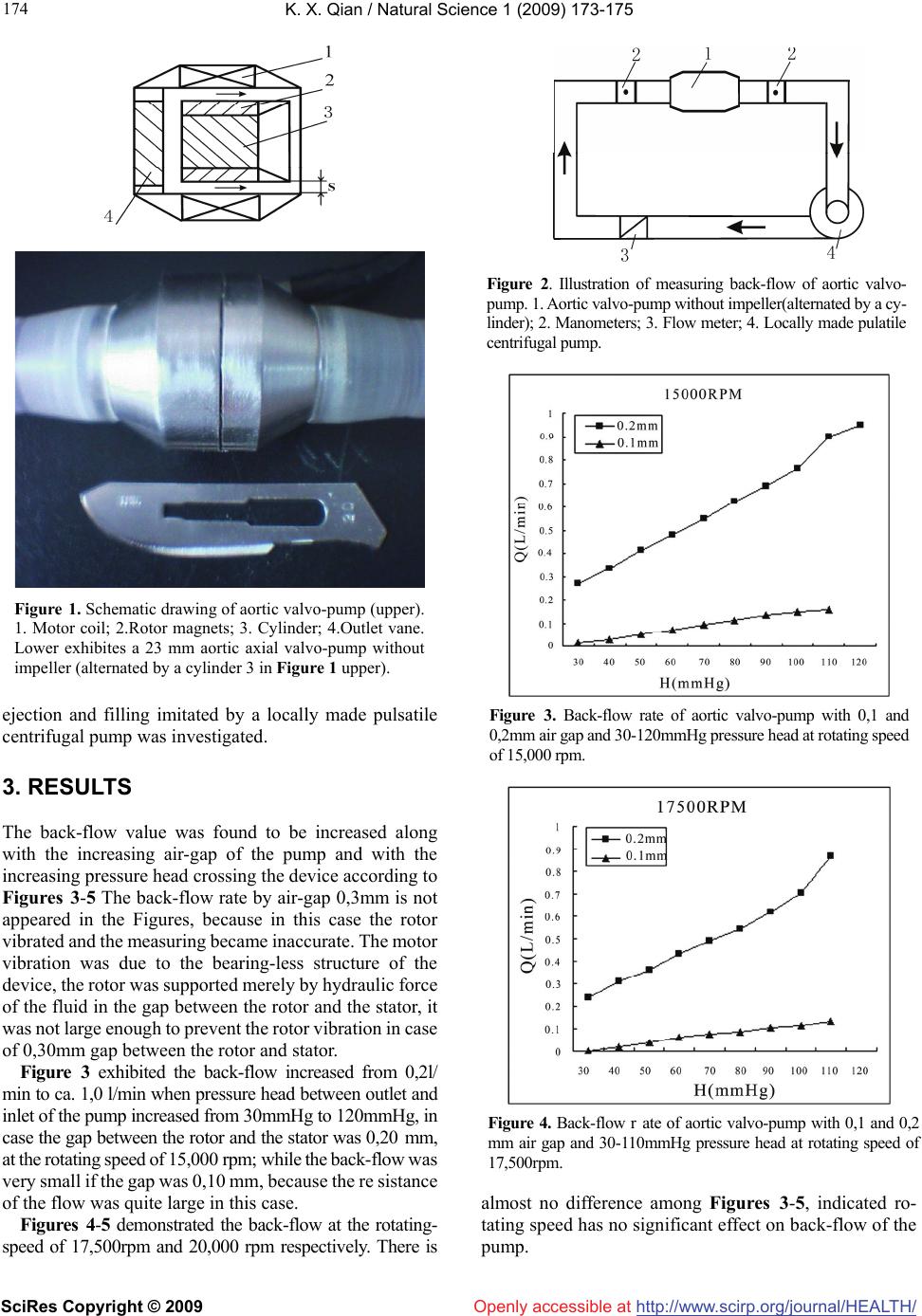 K. X. Qian / Natural Science 1 (2009) 173-175 SciRes Copyright © 2009 Openly accessible at http://www.scirp.org/journal/HEALTH/ 174 Figure 1. Schematic drawing of aortic valvo-pump (upper). 1. Motor coil; 2.Rotor magnets; 3. Cylinder; 4.Outlet vane. Lower exhibites a 23 mm aortic axial valvo-pump without impeller (alternated by a cylinder 3 in Figure 1 upper). ejection and filling imitated by a locally made pulsatile centrifugal pump was investigated. 3. RESULTS The back-flow value was found to be increased along with the increasing air-gap of the pump and with the increasing pressure head crossing the device according to Figures 3-5 The back-flow rate by air-gap 0,3mm is not appeared in the Figures, because in this case the rotor vibrated and the measuring became inaccurate. The motor vibration was due to the bearing-less structure of the device, the rotor was supported merely by hydraulic force of the fluid in the gap between the rotor and the stator, it was not large enough to prevent the rotor vibration in case of 0,30mm gap between the rotor and stator. Figure 3 exhibited the back-flow increased from 0,2l/ min to ca. 1,0 l/min when pressure head between outlet and inlet of the pump increased from 30mmHg to 120mmHg, in case the gap between the rotor and the stator was 0,20 mm, at the rotating speed of 15,000 rpm; while the back-flow was very small if the gap was 0,10 mm, because the re sistance of the flow was quite large in this case. Figures 4-5 demonstrated the back-flow at the rotating- speed of 17,500rpm and 20,000 rpm respectively. There is Figure 2. Illustration of measuring back-flow of aortic valvo- pump. 1. Aortic valvo-pump without impeller(alternated by a cy- linder); 2. Manometers; 3. Flow meter; 4. Locally made pulatile centrifugal pump. Figure 3. Back-flow rate of aortic valvo-pump with 0,1 and 0,2mm air gap and 30-120mmHg pressure head at rotating speed of 15,000 rpm. Figure 4. Back-flow r ate of aortic valvo-pump with 0,1 and 0,2 mm air gap and 30-110mmHg pressure head at rotating speed of 17,500rpm. almost no difference among Figures 3-5, indicated ro- tating speed has no significant effect on back-flow of the pump. 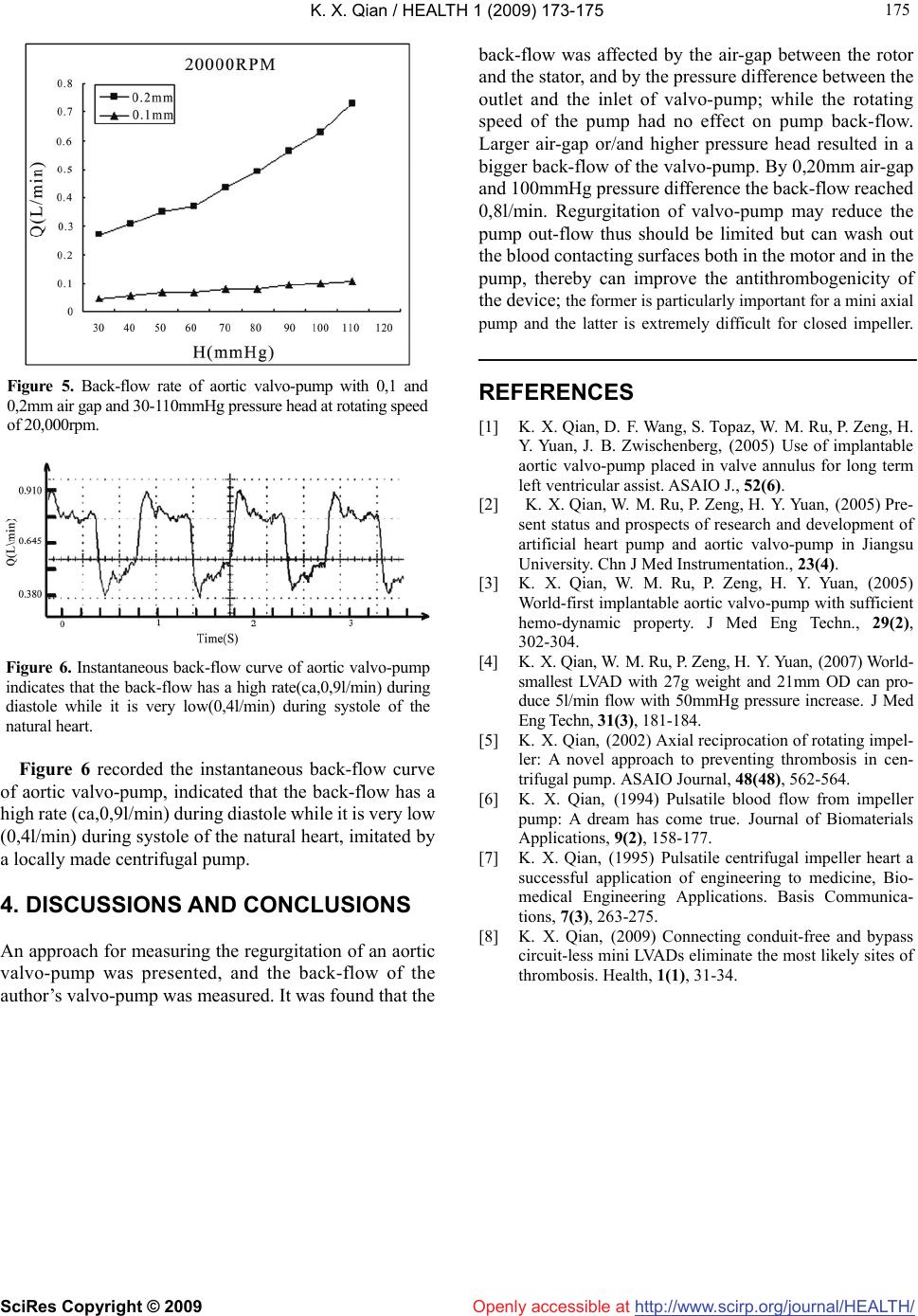 K. X. Qian / HEALTH 1 (2009) 173-175 SciRes Copyright © 2009 Openly accessible at http://www.scirp.org/journal/HEALTH/ 175 175 Figure 5. Back-flow rate of aortic valvo-pump with 0,1 and 0,2mm air gap and 30-110mmHg pressure head at rotating speed of 20,000rpm. Figure 6. Instantaneous back-flow curve of aortic valvo-pump indicates that the back-flow has a high rate(ca,0,9l/min) during diastole while it is very low(0,4l/min) during systole of the natural heart. Figure 6 recorded the instantaneous back-flow curve of aortic valvo-pump, indicated that the back-flow has a high rate (ca,0,9l/min) during diastole while it is very low (0,4l/min) during systole of the natural heart, imitated by a locally made centrifugal pump. 4. DISCUSSIONS AND CONCLUSIONS An approach for measuring the regurgitation of an aortic valvo-pump was presented, and the back-flow of the author’s valvo-pump was measured. It was found that the back-flow was affected by the air-gap between the rotor and the stator, and by the pressure difference between the outlet and the inlet of valvo-pump; while the rotating speed of the pump had no effect on pump back-flow. Larger air-gap or/and higher pressure head resulted in a bigger back-flow of the valvo-pump. By 0,20mm air-gap and 100mmHg pressure difference the back-flow reached 0,8l/min. Regurgitation of valvo-pump may reduce the pump out-flow thus should be limited but can wash out the blood contacting surfaces both in the motor and in the pump, thereby can improve the antithrombogenicity of the device; the former is particularly important for a mini axial pump and the latter is extremely difficult for closed impeller. REFERENCES [1] K. X. Qian, D. F. Wang, S. Topaz, W. M. Ru, P. Zeng, H. Y. Yuan, J. B. Zwischenberg, (2005) Use of implantable aortic valvo-pump placed in valve annulus for long term left ventricular assist. ASAIO J., 52(6). [2] K. X. Qian, W. M. Ru, P. Zeng, H. Y. Yuan, (2005) Pre- sent status and prospects of research and development of artificial heart pump and aortic valvo-pump in Jiangsu University. Chn J Med Instrumentation., 23(4). [3] K. X. Qian, W. M. Ru, P. Zeng, H. Y. Yuan, (2005) World-first implantable aortic valvo-pump with sufficient hemo-dynamic property. J Med Eng Techn., 29(2), 302-304. [4] K. X. Qian, W. M. Ru, P. Zeng, H. Y. Yuan, (2007) World- smallest LVAD with 27g weight and 21mm OD can pro- duce 5l/min flow with 50mmHg pressure increase. J Med Eng Techn, 31(3), 181-184. [5] K. X. Qian, (2002) Axial reciprocation of rotating impel- ler: A novel approach to preventing thrombosis in cen- trifugal pump. ASAIO Journal, 48(48), 562-564. [6] K. X. Qian, (1994) Pulsatile blood flow from impeller pump: A dream has come true. Journal of Biomaterials Applications, 9(2), 158-177. [7] K. X. Qian, (1995) Pulsatile centrifugal impeller heart a successful application of engineering to medicine, Bio- medical Engineering Applications. Basis Communica- tions, 7(3), 263-275. [8] K. X. Qian, (2009) Connecting conduit-free and bypass circuit-less mini LVADs eliminate the most likely sites of thrombosis. Health, 1(1), 31-34. |