 Vol.3, No.12, 762-771 (2011) doi:10.4236/health.2011.312127 C opyright © 2011 SciRes. Openly accessible at http:// www.scirp.org/journal/HEALTH/ Health Socioeconomic inequalities in the use of delivery care services in Bangladesh: a comparative study between 2004 and 2007* Jahan Shabnam1, Mervyn Gifford 2, Koustuv Dalal2# 1Independent Researcher, Denmark; 2Department of Public Health Science, School of Life Sciences, University of Skövde, Skövde, Sweden; #Corresponding Author: koustuv2010@hotmail.com Received 20 August 2011; revised 21 October 2011; accepted 29 October 2011. ABSTRACT The study explores inequalities in the utilization of delivery care services in different administra- tive divisions in Bangladesh, by key socioeco- nomic factors. It estimates the extent of the re- lationship between women’s socioeconomic in- equalities and their place of delivery during 2004 and 2007. Trends in relation to place of delivery in relation to residency and education over a period of thirteen years (1993-2007) have also been measured. The study analyzed the trends and patterns in utilization of institutional delivery care among mothers, using data from the Bangladesh Demographic Health Survey (BDHS) conducted during 1993-2007. The data was disaggregated by area of residence in dif- ferent divisions in Bangladesh. Bi-variate ana- lyses, concentration curves and multivariate lo- gistic regression w ere employed in the analysis of the data. The study indicated slow progress in the utilization of institutional delivery care among mothers in Bangladesh between 1993 and 2007. Large variations in outcome meas- ures were observed among the different divi- sions. Multivariate analyses suggested grow ing inequalities in utilization of delivery care ser- vices between different economic groups and parents with different educational levels. The use of institutional delivery care remains sub- stantially lower among poor and less educated rural mothers in Bangladesh, irrespectiv e of age and employment. Further studies are recom- mended to explore the specific causes relating to the non-utilization of institutional delivery care. Keyw ords: Home Delivery; Lorenz Curve; Socioeconomic Status; Trend; Banglad esh 1. INTRODUCTION Globally, 1500 women die every day because of prob- lems in pregnancy and childbirth. The burden is highest in Africa, followed by the South Asian region [1]. The disparity between maternal mortality in low and high income countries is striking, almost all (99%) maternal deaths occur in low income countries [2,3]. The WHO has identified the major causes of maternal mortality; these are severe hemorrhage (25%), infection (15%), eclampsia (12%), obstructed labor (8%) and/or unsafe abortion (13%) [1]. However, it is evident that most of these deaths could be prevented through timely care- seeking during pregnancy and the presence of a Skilled Birth Attendant (SBA) during delivery [4-6]. Morbidity and mortality are both serious public health concerns in Bangladesh. According to data from UNI- CEF, Bangladesh has a high Maternal Mortality Ratio (MMR), with 320 deaths per 100,000 births [7]. Along with the United Nations, the Government of Bangladesh is committed to achieving the Millennium Development Goal (MDG)-5, to reduce the MMR by 75% between 1990 and 2015. Despite the improvements in child health and family planning outcomes in Bangladesh, the MMR has reduced by only 38%, between 1991 and 2007, in spite of the fact that making pregnancy and childbearing safer for women has been identified as a central element of the MDGs [8]. Emergency obstetric care (EmOC) can help address the above mentioned delivery complications and the mortality and morbidity of the pregnant women could be reduced accordingly in Bangladesh. In the evolving stra- tegy of the Safe Motherhood movement since 1990, the Government of Bangladesh has implemented the EmOC service throughout the country [9,10]. Despite the initia- *Conflict of interest: declared none.  J. Shabnam et al. / Health 3 (2011) 762-771 Copyright © 2011 SciRes. Openly accessible at http:// www.scirp.org/journal/HEALTH/ 763763 tives taken by the Government, the key question is whether the women of all strata of the society actually receive the level of care they require. The survey by Na- tional Institute of Population Research and Training (NIPORT) 2002 shows that about two thirds of the rural deliveries are assisted by untrained Traditional Birth Attendants (TBAs), about 12% by trained TBAs, and another 12% by relatives/others [11,12]. In addition, only 63% of pregnant women seek antenatal care. 15% of deliveries took place in some kind of health facility, and 18% of women received delivery care from health care providers [13]. To achieve the MDG 5, the Government of Bangla- desh should speed up the process of improving the over- all situation of the women in the country by improving their socioeconomic status [14]. As is the case in other developing countries, maternal health care use in Bang- ladesh varies between women with different socioeco- nomic status, the demographic area, the educational level of the parents, religious factors and decision making power [13,15]. A study of Safe motherhood programs in Bangladesh showed that the low status of women in society, the poor quality of maternity care services, the lack of trained providers, the low uptake of services by women and the poor infrastructure all contribute to the high maternal death rates [16]. The place of delivery is the key issue of Safe Motherhood which remains a great challenge for the policy makers of Bangladesh. This may be due to the traditional view of rural societies. Culturally and tradi- tionally, most of the deliveries take place at a woman’s or her parents’ home. The majority of the homes are in rural areas and are therefore quite far from the hosptials or clinics where there are sufficient services for treating pregnant women who are at risk of delivery complica- tions [12]. Several studies showed that, in addition to the availability of health care, socioeconomic factors―such as women’s age, the education level of a woman and her husband, religion, location, wealth, employment status etc., also greatly influence maternal care utilization [12, 15,17,18]. There is wide variation in the utilization of health-re- lated cares services between lower and higher economic strata in Bangladesh. There is evidence that Socioeco- nomic inequality-related utilization of delivery care ex- ists both between countries and within countries [19,20]. Several studies have been carried out to examine the relationship between increasing socioeconomic and the utilization of delivery care in the context of low income and high income countries [15]. Few studies though have been conducted in Bangladesh which take into ac- count the trends and regional patterns of disparities in the utilization of delivery care services [20-22]. The study explores inequalities in the utilization of de- livery care services in different administrative divisions in Bangladesh, by key socioeconomic factors. It esti- mates the extent of the relationship between women’s socioeconomic inequalities and their place of delivery during 2004 and 2007. Trends in relation to place of de- livery in relation to residency and education over a pe- riod of thirteen years (1993-2007) have also been meas- ured. 2. METHODS The study used data from the Bangladesh Demo- graphic and Health Surveys (BDHS). This is a nationally representative household survey based on structured questionnaires [23]. The BDHS has been a vital source of both individual and household-level data in relation to health and health care since 1993. The study used BDHS datasets, namely, BDHS 1993, BDHS 1997, BDHS 2000, BDHS 2004 and BDHS 2007. Each data set contains data from approximately 10,000 households and each survey had questionnaires for both men and women. The study was based upon the questionnaires for women aged 15 - 49 years. The survey involved multistage clus- ter sampling and it was based on the population census Enumeration Areas (EAs) which include population and household information. EAs were used as Primary Sam- pling Units (PSUs) for the whole survey. Each PSU contained 100 households, identified with locational maps and geographical boundaries. In total 361 PSUs (227 in rural and 134 in urban areas) were randomly selected from the six divisions, namely, Barisal, Chit- tagong, Dhaka, Khulna, Rajshahi and Sylhet. Before conducting the main survey in the PSUs, a household recording was carried out. This was used as the sampling frame for the identification of households in the second stage. In the next stage, 30 households were selected from each PSU, using an equal probability systematic sampling technique and using information from the 2001 population census. Finally, 10,819 house- holds were selected from the sample clusters for inclu- sion in the survey. 2.1. Stud y Population BDHS 2004: For the BDHS, 10,811 households were included. From the selected households, 11,601 eligible women aged between 10 - 49 years were identified. Of these 11,601 women, 11,440 were interviewed (a re- sponse rate of 98.6%). To simplify the data analysis, data from women aged 10 - 14 years were merged with data from the women aged 15 - 19 years. BDHS 2007: For the BDHS 10,400 households were selected. From the selected households, 11,178 suitable  J. Shabnam et al. / Health 3 (2011) 762-771 Copyright © 2011 SciRes. Openly accessible at http:// www.scirp.org/journal/HEALTH/ 764 women aged 15 - 49 were selected. From this sample 10,996 were eventually interviewed (a response rate of 98.4%). 2.2. Sample Size For this current study based upon the 2004 data set, 5366 eligible women (with at least one child delivery) were included. This represents 47% of the total 11,440 women respondents. From the 2007 data set, 4925 eligi- ble women (with at least one child delivery) were in- cluded. This represents 45% of the total 10,996 women respondents in the study. 2.3. Questionnaire The questionnaire comprised demographics, repro- ductive behavior and intentions, knowledge and use of contraception, sexual life, nutrition, maternal and child health, knowledge of HIV/AIDS and other sexually transmitted diseases, etc. For this study questions relat- ing to demographics, wealth index and history of deliv- ery were also taken into account. 2.4. Description of the Variables of Interest The utilization of health facilities during delivery took into account the place of delivery, such as delivery at home or at other health facilities. Other facilities in- cluded Government hospitals, private hospitals/clinic and NGOs. The independent variables were age (groups divided into seven categories 15 - 19, 20 - 24, 25 - 29, 30 - 34, 35 - 39, 40 - 44 and 45 - 49); residency (urban or rural); the level of education of the women (no education, pri- mary education, secondary education and higher educa- tion); religion (Muslim or non-Muslim); divisional resi- dence within Bangladesh (Dhaka, Barisal, Sylhet, Ra- jshahi, Chittagong, Khulna); working status (working or not working); partner’s level of education (no education, primary education, secondary education and higher edu- cation). The economic statuses of the respondents were classi- fied as: poorest, poorer, middle, richer and richest. The economic statuses of the respondents were categorized based on data from the wealth index. This is extensively used to measure the economic status and to determine the equity of health programs in public or private ser- vices. Its major objectives are to assess both the ability to pay for health services and the allocation of services amongst the poor. Many demographic and health surveys in different parts of the world have validated and used the wealth index. It is a combined assessment of the cu- mulative living standard of a household. It is measured by using data on a household’s ownership of particular assets, e.g. radios, televisions and bicycles; materials used for construction of the house, types of water-access and the use of sanitation facilities. A statistical procedure called Principle Components Analysis is used in the wealth index calculations and it places a household on a point on a constant scale of relative wealth. The scale is consistent with a standard normal distribution with a mean of zero and a standard deviation of one. Thus, the regularly distributed scores can be partitioned to gener- ate the groups that classify wealth quintiles as: Poorest, poorer, average, richer and richest. The wealth index was introduced by Rutstein and Johnson and has been widely used in several studies [24-26]. The term Wealth Index comprises anything that may be a sign of economic status, particularly the major household assets and utility services, as well as country-specific items. 2.5. Ethical Issues In Bangladesh, the Demographic Health Survey (DHS) procedure (e.g. organization and sampling methods) and the instruments applied in the study received ethical permission from the Institutional Review Board of ORC Macro Inc, which gave the major scientific support for the whole survey. The consent to apply these data was acquired from Measure DHS, the officially authorized owner of the survey data under the main donor agency, USAID after proper project applications. This study is based on the secondary analysis of ex- isting survey data. All the information that might be used to identify the respondents was removed. The field in- terviewers for the survey acquired informed consent from the respondents and the respondents were assured of strict confidentiality. The respondents had the auton- omy to leave the study at any time. 2.6. Statistical Analysis Differences between the values of the dependent vari- ables (Place of delivery in 2004 and 2007) between the participants on different categories of the explanatory variables (i.e. demographics) were assessed using chi- square tests. Inequalities in health in different divisions were assessed by the Lorenz curve for 2004 and 2007 [27,28]. The X axis comprises the cumulative percentage (%) of wealth index and the Y axis the cumulative per- centage of utilization of delivery care. The trend of place of delivery in different years, percentage of home deliv- ery in 2004 and 2007 in six divisions and the trend of home delivery in different years in relation to the level of education were presented with line graphs. For as- sessing possible confounding effects in predicting home delivery, a multivariate logistic regression analysis was employed in the adjusted model. Some of the predictor  J. Shabnam et al. / Health 3 (2011) 762-771 Copyright © 2011 SciRes. Openly accessible at http:// www.scirp.org/journal/HEALTH/ 765765 variables included in the multivariate analysis, such as economic status, partners education and working status were not included in previous surveys, namely BDHS 1993, BDHS 1997 and BDHS 2000) but were included in the surveys of BDHS 2004 and BDHS 2007. That is the reason for including only two years data in multi- level and bi-variate analyses. However, delivery trend was estimated for all the five survey data (BDHSs: 1993, 1997, 2000, 2004 and 2007). The magnitude and direc- tion of association were expressed through odds ratios and significance levels were expressed as P values. Sta- tistical significance was considered to be P < 0.05. SPSS version 18.0 was used for all analyses. 3. RESULTS The demographics of the women indicate that regard- less of age, both in 2004 and 2007, more than 80% had home deliveries. In 2004 the range varied from 86% to 98% and in 2007 the range varied from 80% to 96%. In both years the highest percentage of women who had home deliveries was in the 45 - 49 years age group. The p value is not significant in relation to the age group and delivery at home, in both 2004 and 2007. In both 2004 and 2007 relatively more women in rural areas had home deliveries compared with those in urban areas. In both 2004 and 2007 the chi square test shows a significant relationship between residency and home deliveries. The level of education shows a distinct difference in relation to home deliveries. The women with least edu- cation had the highest percentage of home deliveries, both in 2004 and 2007 (97%). Higher education was associated with the least percentage of home deliveries in both 2004 (43%) and 2007 (33%). The p value is sig- nificant in both 2004 and 2007 in relation to the level of education and delivery at home. In both 2004 and 2007, non-Muslim women had a fewer home deliveries com- pared with Muslim women. The chi square test shows a significant relationship between religion and delivery at home, in both 2004 and 2007 (Table 1). The trends of delivery in different years (Figure 1) show that the number of home deliveries have reduced moderately over the years. In contrast, the number of deliveries in public hospitals, private hospitals and NGOs increased over this period. To summarize; the trend shows that the number of home deliveries decreased while deliveries in other health facilities increased over the time. The trend of delivery in different divisions (Figure 2) shows that in different years home delivery levels re- mained lowest in Khulna in both 2004 and 2007. The rate was highest in the Barisal division (91%) in 2004 and in the Sylhet division (87%) in the year 2007. The Table 1. Demographics of the delivery at home in 2004 and 2007. Demographics Home delivery 2004 N% of N Home delivery 2007 N% of N Age Group 15 - 19 years 20 - 24 years 25 - 29 years 30 - 34 years 35 - 39 years 40 - 44 years 45 - 49 years 892 1736 1338 837 389 126 48 P = 0.011 86 87 86 86 91 94 98 749 1627 1250 745 393 139 22 P = 0.015 83 80 79 80 81 91 96 Residency Urban Rural 1684 3682 P = 0.000 74 93 1748 3177 P = 0.000 67 89 Level of Education No Education Primary Secondary Higher 1866 1649 1512 339 P = 0.000 97 91 80 43 1267 1507 1742 406 P = 0.000 97 91 72 33 Partner’s Education Level No Education Primary Secondary Higher 1991 1433 1335 604 P = 0.000 95 93 82 56 1584 1380 1319 636 P = 0.000 95 90 75 42 Religion Muslim Non Muslim 4876 490 P = 0.000 88 79 4472 453 P = 0.000 82 74 P-values of chi-square tests. Figure 1. The trend of delivery in different years. results show that Khulna maintained the lowest percent- age of deliveries at home over time, whilst Barisal and Sylhet had higher percentages of home deliveries. The trend for home delivery in relation to education follows almost the same trend throughout the whole pe- riod (Figure 3). The women with no education mostly tended to have home deliveries. 97% of women between  J. Shabnam et al. / Health 3 (2011) 762-771 Copyright © 2011 SciRes. http://www.scirp.org/journal/HEALTH/ 766 Chittagong division in the year 2007, though the curve was initially below the line of equality, which indicates that home deliveries were concentrated among the poor. In 2007, the concentration curves for home delivery in Dhaka, Sylhet, Chittagong, Khulna all lie below that those for Barisal and Rajshahi. This indicates that there is less inequality at Dhaka, Sylhet, Chittagong, Khulna than in Barisal or Rajshahi. The Concentration curve (Lorenz) for the utilization of delivery care in different divisions in 2004 shows that, the concentration curves of all the six divisions lie above (dominate) the line of equality, indicating that the home deliveries are concentrated among the poor. The concen- tration curves for home delivery for Dhaka, Sylhet, Chittagong, Khulna for the period 2004 all lie below that of Rajshahi (i.e. the Rajshahi curve dominates the other mentioned curves), indicating there is less inequality at Dhaka, Sylhet, Chittagong, Khulna than in Rajshahi. Figure 2. The trend of delivery in different divisions. 1993 and 1994 had home deliveries, though this figure fell to 91% in 2007. Women with secondary education had comparatively fewer home deliveries than the other two mentioned groups. 88% had home deliveries during the period of the survey in 1993, while 72% had home deliveries in 2007. Finally the women with higher edu- cation had the smallest percentage of home deliveries from the outset of the surveys. During the initial survey the figure was 50%, reducing thereafter to 33% in 2007. All the groups of women had fewer home deliveries over time. The statistics show a sharp reduction in the number of home deliveries amongst more highly educated women. The reduction was only slightly reduced in rela- tion to women with no education (Figure 3). Table 2 indicated that respondents’ age and employ- ment status had no significant relationship with delivery at home. Respondents’ residency, education, economic status and religion emerged as the strongest predictors of delivery care. Compared with more highly educated women, their uneducated peers were eight times more likely and 12 times more likely to deliver at home in 2004 and 2007 respectively. Similarly, women educated to primary level had more home deliveries in 2007 compared with 2004. Figures 4(a)-(b) demonstrates the Lorenz curves. The Concentration Curve (Lorenz) for the utilization of delivery care in different divisions in 2007 shows that, apart from Chittagong, all the concentration curves rep- resenting all five divisions lie above (dominate) the line of equality, indicating that the home deliveries are con- centrated among the poor. The concentration curve shows that the inequality in home delivery increased fairly in 4. DISCUSSION The study showed that even after three years (2004- 2007) there was no such improved situation of deliveries at home. The demographic factors of residency, level of Figure 3. The trend of home delivery in relation to the maternal education level. Openly accessible at  J. Shabnam et al. / Health 3 (2011) 762-771 Copyright © 2011 SciRes. Openly accessible at http:// www.scirp.org/journal/HEALTH/ 767767 (a) (b) Figure 4. (a) Concentration (Lorenz) curve for delivery care utilization during 2004; (b) Concentration (Lorenz) curve for delivery care utilization during 2007. education, wealth index and religion were associated with the choice of delivery in a health facility rather than delivery at home in both the years examined. Inequality in health in relation to delivery was present in both years in all six administrative areas. Multivariate logistic re- gression showed that residency, level of education, part- ner educational level, wealth index, and religion had a strong relationship with delivery at home. The working status of the respondent was shown not to have any in- fluence in home delivery. The study showed that since 1993 the trend for home delivery is declining though it showed highest percentage in all years. It can be con- cluded from this result that home delivery had was the most popular type of deliver throughout Bangladesh. It is notable that the respondents with highest educational levels had the fewest home deliveries. The findings of the present study illustrate that in 2004 and 2007, eco- nomic inequality in the utilization of maternal health care was predominant in the Rajshahi and Barisal divi- sions. Barisal has demonstrated the greatest inequality for home delivery in recent years, indicating cultural conservative issues and infrastructural problems [20]. During recent years, all divisions (except Dhaka) had more inequalities than previous years. This indicates that inequalities are still increasing in Bangladesh. The re- gression analysis showed that the probability of home delivery was higher for mothers with no, or only primary education. Overall, an educated mother utilized more 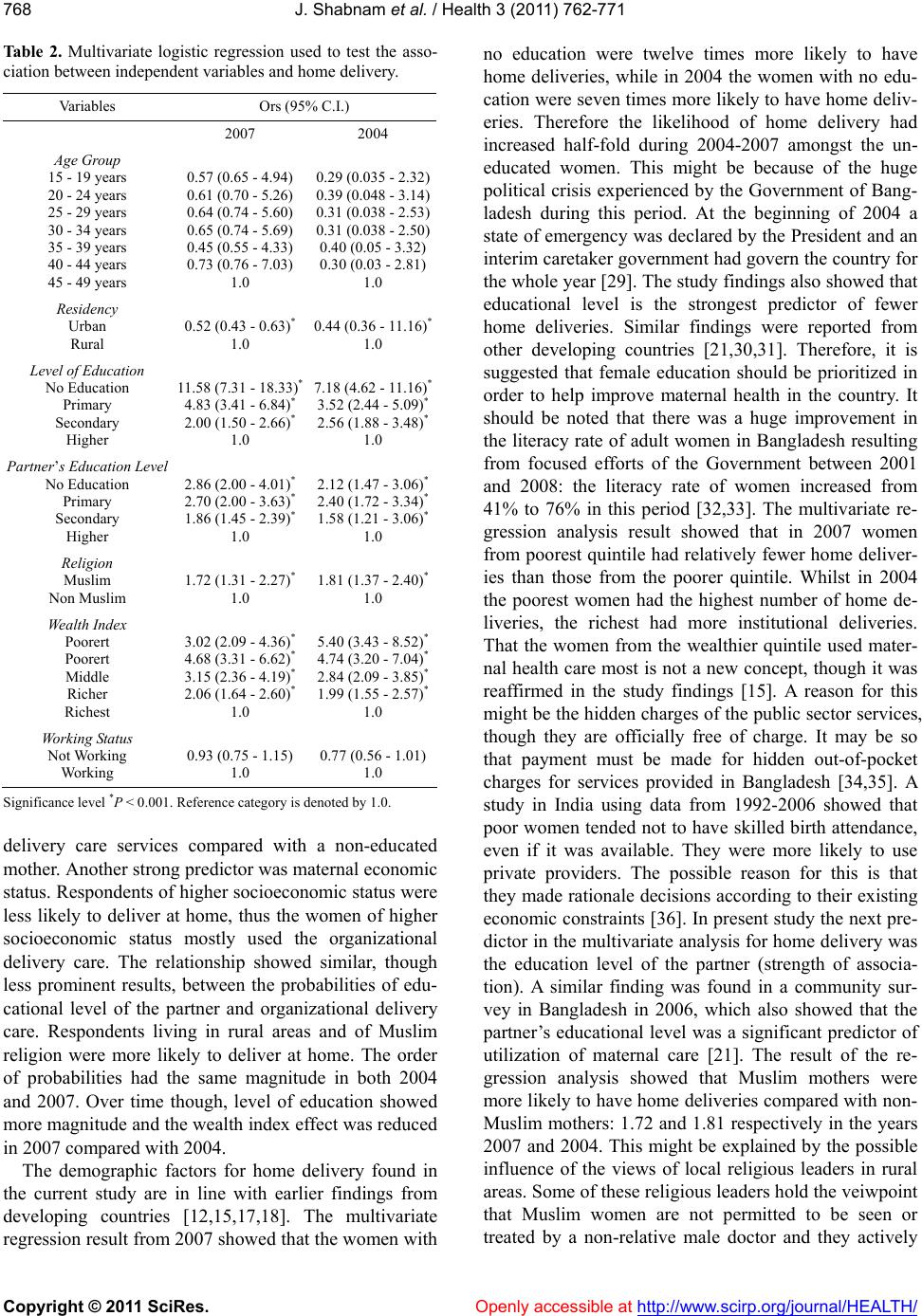 J. Shabnam et al. / Health 3 (2011) 762-771 Copyright © 2011 SciRes. Openly accessible at http:// www.scirp.org/journal/HEALTH/ 768 Ta b l e 2 . Multivariate logistic regression used to test the asso- ciation between independent variables and home delivery. Variables Ors (95% C.I.) 2007 2004 Age Group 15 - 19 years 20 - 24 years 25 - 29 years 30 - 34 years 35 - 39 years 40 - 44 years 45 - 49 years 0.57 (0.65 - 4.94) 0.61 (0.70 - 5.26) 0.64 (0.74 - 5.60) 0.65 (0.74 - 5.69) 0.45 (0.55 - 4.33) 0.73 (0.76 - 7.03) 1.0 0.29 (0.035 - 2.32) 0.39 (0.048 - 3.14) 0.31 (0.038 - 2.53) 0.31 (0.038 - 2.50) 0.40 (0.05 - 3.32) 0.30 (0.03 - 2.81) 1.0 Residency Urban Rural 0.52 (0.43 - 0.63)* 1.0 0.44 (0.36 - 11.16)* 1.0 Level of Education No Education Primary Secondary Higher 11.58 (7.31 - 18.33)* 4.83 (3.41 - 6.84)* 2.00 (1.50 - 2.66)* 1.0 7.18 (4.62 - 11.16)* 3.52 (2.44 - 5.09)* 2.56 (1.88 - 3.48)* 1.0 Partner’s Education Level No Education Primary Secondary Higher 2.86 (2.00 - 4.01)* 2.70 (2.00 - 3.63)* 1.86 (1.45 - 2.39)* 1.0 2.12 (1.47 - 3.06)* 2.40 (1.72 - 3.34)* 1.58 (1.21 - 3.06)* 1.0 Religion Muslim Non Muslim 1.72 (1.31 - 2.27)* 1.0 1.81 (1.37 - 2.40)* 1.0 Wealth Index Poorert Poorert Middle Richer Richest 3.02 (2.09 - 4.36)* 4.68 (3.31 - 6.62)* 3.15 (2.36 - 4.19)* 2.06 (1.64 - 2.60)* 1.0 5.40 (3.43 - 8.52)* 4.74 (3.20 - 7.04)* 2.84 (2.09 - 3.85)* 1.99 (1.55 - 2.57)* 1.0 Working Status Not Working Working 0.93 (0.75 - 1.15) 1.0 0.77 (0.56 - 1.01) 1.0 Significance level *P < 0.001. Reference category is denoted by 1.0. delivery care services compared with a non-educated mother. Another strong predictor was maternal economic status. Respondents of higher socioeconomic status were less likely to deliver at home, thus the women of higher socioeconomic status mostly used the organizational delivery care. The relationship showed similar, though less prominent results, between the probabilities of edu- cational level of the partner and organizational delivery care. Respondents living in rural areas and of Muslim religion were more likely to deliver at home. The order of probabilities had the same magnitude in both 2004 and 2007. Over time though, level of education showed more magnitude and the wealth index effect was reduced in 2007 compared with 2004. The demographic factors for home delivery found in the current study are in line with earlier findings from developing countries [12,15,17,18]. The multivariate regression result from 2007 showed that the women with no education were twelve times more likely to have home deliveries, while in 2004 the women with no edu- cation were seven times more likely to have home deliv- eries. Therefore the likelihood of home delivery had increased half-fold during 2004-2007 amongst the un- educated women. This might be because of the huge political crisis experienced by the Government of Bang- ladesh during this period. At the beginning of 2004 a state of emergency was declared by the President and an interim caretaker government had govern the country for the whole year [29]. The study findings also showed that educational level is the strongest predictor of fewer home deliveries. Similar findings were reported from other developing countries [21,30,31]. Therefore, it is suggested that female education should be prioritized in order to help improve maternal health in the country. It should be noted that there was a huge improvement in the literacy rate of adult women in Bangladesh resulting from focused efforts of the Government between 2001 and 2008: the literacy rate of women increased from 41% to 76% in this period [32,33]. The multivariate re- gression analysis result showed that in 2007 women from poorest quintile had relatively fewer home deliver- ies than those from the poorer quintile. Whilst in 2004 the poorest women had the highest number of home de- liveries, the richest had more institutional deliveries. That the women from the wealthier quintile used mater- nal health care most is not a new concept, though it was reaffirmed in the study findings [15]. A reason for this might be the hidden charges of the public sector services, though they are officially free of charge. It may be so that payment must be made for hidden out-of-pocket charges for services provided in Bangladesh [34,35]. A study in India using data from 1992-2006 showed that poor women tended not to have skilled birth attendance, even if it was available. They were more likely to use private providers. The possible reason for this is that they made rationale decisions according to their existing economic constraints [36]. In present study the next pre- dictor in the multivariate analysis for home delivery was the education level of the partner (strength of associa- tion). A similar finding was found in a community sur- vey in Bangladesh in 2006, which also showed that the partner’s educational level was a significant predictor of utilization of maternal care [21]. The result of the re- gression analysis showed that Muslim mothers were more likely to have home deliveries compared with non- Muslim mothers: 1.72 and 1.81 respectively in the years 2007 and 2004. This might be explained by the possible influence of the views of local religious leaders in rural areas. Some of these religious leaders hold the veiwpoint that Muslim women are not permitted to be seen or treated by a non-relative male doctor and they actively  J. Shabnam et al. / Health 3 (2011) 762-771 Copyright © 2011 SciRes. Openly accessible at http:// www.scirp.org/journal/HEALTH/ 769769 discourage the women from seeking maternal care ser- vices while they are pregnant [22]. The present study showed that women living in urban areas had lower probabilities for home deliveries. The chi square results showed that the percentage declined in 2007 compared with 2004. The multivariate analysis reconfirmed the findings of fewer home deliveries in the case of women in urban areas. The findings are in line results from the systemic review conducted by Say and Raine [15]. In- stitutional deliveries are possibly more common in urban areas than rural areas because of better transport systems, well-equipped hospitals and the provision of sufficient trained professionals in the urban hospitals. There was no significant relationship between the employment of women and the utilization of delivery care. A study was conducted in rural Bangladesh to identify the determi- nants of the use of maternal health services, and this also showed that the working status of women is not a posi- tive factor for the uptake of maternal home delivery. This might be because of the context and of the culture of the country, which does not permit the women to spend their money as they please [37]. Estimates of inequalities in the utilization of delivery care in different divisions of Bangladesh were achieved in the present study by plotting concentration curves. The figures showed that there are inequalities between the divisions. A study in Bangladesh was carried out to identify the reason behind inequalities in EmOC Ser- vices between the Khulna and Sylhet divisions―rela- tively high and low-performing areas of Bangladesh respectively [38]. The study showed that the major bar- riers for maternal health in Sylhet were the human-re- sources limitations, along with the poor quality of health facilities available in the hospitals. Moreover, the find- ings showed that the population in Sylhet was less liter- ate, more conservative, and faced more geographical and socio-cultural obstacles in accessing services [38]. More such studies should be conducted in the future to identify the barriers in different divisions and to plan interven- tions accordingly. The results in from the current study did not yield strong information on the influence of other predisposing and enabling factors, such as age of the women and their employment in the utilization of insti- tutional delivery care. The chi square and the multivari- ate logistic regression did not show any significant im- pact of these factors on the use of utilization of institu- tional delivery care. Regardless of all the findings, women from a traditional culture like that in Bangladesh might have a strong preference for home-based birth traditions, and they might prefer to utilize TBAs with whom they have better social relations. Such factors may be important in influencing their decision to choose home deliveries [21]. The current study has made a significant contribution to the knowledge of the various factors that can have an influence as to where women deliver their babies. A ma- jor strength was that it was nationally representative, thus allowing for conclusions to be relevant to the whole nation. One weakness of the study is the cross-sectional design which did not allow for causal attributions. A longitudinal study design could more easily identify causal links. The use of additional qualitative studies to investigate women’s choices for the place of delivery is necessary in order to study the influence of socioeco- nomic inequalities and social norms. Moreover, studies within the different divisions of Bangladesh are required to help identify the reasons for inequalities in utilization of maternal health care services. Another limitation of the current study is that not all the same households were followed in the survey over the period of time because of several alterations to the administrative areas of Bangla- desh. The findings of the current study may be legitimately generalized to some other South Asian, African and Latin American countries, which have similar socioeco- nomic conditions and inequitable delivery care services. A notable important policy implication emerged from the study findings. Most of the deliveries take place at home, and since it will take a long time to change this practice, maximum efforts should be made towards en- hanced training of birth attendants. These birth atten- dants could help in delivery at home and also help in making referrals to the nearest health facility, should the need arise. It is timely that Government policy and programs should aim to increase the uptake of professional deliv- ery care. The study findings suggest some areas for pol- icy makers to focus upon. The main finding of this study is the excessively high number of home delivery among mothers in Bangladesh, irrespective of age. There are also noticeable socioeconomic inequities in the use of delivery care services. To reach MDG-5 targets, de- creasing the socioeconomic inequalities in maternal de- livery care ought to be considered as a vital policy. Ad- ditionally, improving the education of women must be a priority since their educational levels have direct conse- quences in determining their choices of childbirth deliv- ery services. It is vital that women have the information and knowledge to help them make informed and intelli- gent choices about where they want to have their babies. Better education should increase the uptake of institu- tional delivery services and greatly enhance the concept and practice of safe motherhood. 5. ACKNOWLEDGEMENTS The authors acknowledge Measures DHS and their staff for data  J. Shabnam et al. / Health 3 (2011) 762-771 Copyright © 2011 SciRes. Openly accessible at http:// www.scirp.org/journal/HEALTH/ 770 collection and permission to use the data. REFERENCES [1] WHO (2008) Maternal mortality fact sheet. http://www.who.int/making_pregnancy_safer/events/200 8/mdg5/factsheet_maternal_mortality.pdf [2] Paruzzolo, S., Mehra, R., Kes, A. and Ashbaugh, C. (2010) Targeting poverty and gender inequality to im- prove maternal health solutions for girls and women. 2nd Global Conference, Washington DC, New York, 7-9 June 2010. [3] Ahmed, S., Creanga, A.A., Gillespie, D.G. and Tsui, A.O. (2010) Economic status, education and empowerment: Implications for maternal health service utilization in developing countries. PLoS One, 23, e11190. [4] Rahman, M.H., Mosley, W.H., Ahmed, S. and Akhter, H.H. (2008) Does service accessibility reduce socioeco- nomic differentials in maternity care seeking? Evidence from rural Bangladesh. Journal of Biosocial Science, 40, 19-33. doi:10.1017/S0021932007002258 [5] Houweling, J., Ronsmans, C., Campbell, O.M.R. and Kunst, A.E. (2007) Huge poor rich inequalities in mater- nity and child care in developing countries. Bulletin of the World Health Organization, 85, 745-754. [6] WHO (2003) Bangladesh: Skilled birth attendant. http://www.whoban.org/skill_birth_training.html [7] UNICEF (2010) Bangladesh: Statistics; women. http://www.unicef.org/infobycountry/bangladesh_bangla desh_statistics.html [8] UNDP (2010) Bangladesh. MDGs and Bangladesh. http://www.undp.org.bd/mdgs.php [9] Colin, S.M., Anwar, I. and Ronsmans, C. (2007) A dec- ade of inequality in maternity care: Antenatal care, pro- fessional attendance at delivery, and caesarean section in Bangladesh (1991-2004). International Journal for Eq- uity in Health, 30, 6-9. [10] Islam, M.T., Hossain, M.M., Islam, M.A. and Haque, Y.A. (2005) Improvement of coverage and utilization of EmOC services in southwestern Bangladesh. Interna- tional Journal of Gynecology & Obstetrics, 91, 298-305. doi:10.1016/j.ijgo.2005.06.029 [11] National Institute of Population Research and Training (NIPROT). ORC Macro. (2002) Bangladesh maternal health services and maternal mortality survey 2001. NI- PORT, Dhaka. [12] Islam, M.A., Chowdhury, R.I. and Akhter, H.H. (2006) Complications during pregnancy, delivery, and postnatal stages and place of delivery in rural Bangladesh. Health Care for Women International, 27, 807-821. doi:10.1080/07399330600880368 [13] Bangladesh Demographic and Health Survey 2007. http://www.measuredhs.com/pubs/pdf/FR207/FR207%5 BApril-10-2009%5D.pdf [14] UNICEF. Bangladesh; health and nutrition; women’s health. http://www.unicef.org/bangladesh/health_nutrition_407.h tm [15] Say, L. and Raine, R. (2007) A systematic review of ine- qualities in the use of maternal health care in developing countries: Examining the scale of the problem and the importance of context. Bulletin of the World Health Or- ganization, 85, 812-819. [16] UNICEF. Maternal health in Bangladesh. http://www.unicef.org/bangladesh/MATERNAL_HEALT H.pdf [17] Gage, A.J. (2007) Barriers to the utilization of maternal health care in rural Mali. Social Science & Medicine, 65, 1666-1682. doi:10.1016/j.socscimed.2007.06.001 [18] Navaneetham, K. and Dharmalingam, A. (2020) Utiliza- tion of maternal health care services in Southern India. Social Science & Medicine, 55, 1849-1869. doi:10.1016/S0277-9536(01)00313-6 [19] Kunst, A.E. and Houweling, T. (2001) A global picture of poor-rich differences in the utilization of delivery care. Studies in Health Services Organization and Policy, 17, 297-316. [20] Ahmed, S. and Hill, K. (2011) Maternal mortality esti- mation at the sub national level: A model based method with an application to Bangladesh. Bulletin of the World Health Organization, 89, 12-21. doi:10.2471/BLT.10.076851 [21] Anwar, I., Sami, M., Akhtar, N., Chowdhury, M.E., Salma, U., Rahman, M. and Koblinskya, M. (2008) In- equity in maternal health-care services: Evidence from home-based skilled-birth-attendant programmes in Bang- ladesh. Bulletin of the World Health Organization, 86, 252-259. doi:10.2471/BLT.07.042754 [22] Hossain, M.I. (2010) Inequality in the utilization of ma- ternal care and the impact of a macroeconomic policy: Evidence from Bangladesh. HEDG Working Paper 10/08, The University of York, York, 1-31. [23] Bangladesh Demographic and Health Survey (2004). http://www.measuredhs.com/countries/country_main.cfm ?ctry_id=1&c=Bangladesh [24] Rutstein, S.O. and Johnson, K. (2004) The DHS wealth index. ORC Macro, Calverton, MD. [25] Dalal, K. (2011) Does economic empowerment protects women from intimate partner violence? Journal of Injury and Violence Research, 3, 35-44. [26] Dalal, K. and Lindqvist, K. (2010) A National study of the prevalence and correlates of domestic violence among women in India. Asia-Pacific Journal of Public Health, Nov 30. [Epub ahead of print] [27] Wagstaff, A. and van Doorslaer, E. (2003) Watanabe N. on decomposing the causes of health sector inequalities, with an application to malnutrition inequalities in Viet- nam. Journal of Econometrics, 112, 219-227. doi:10.1016/S0304-4076(02)00161-6 [28] O’Donnell, O., van Doorslaer, E., Wagstaff, A. and Lin- delow, M. (2008) Analysing health equity using house- hold survey data: A guide to techniques and their imple- mentation, Washington DC. http://web.worldbank.org/WBSITE/EXTERNAL/TOPIC S/EXTHEALTHNUTRITIONANDPOPULATION/EXT PAH/0,,contentMDK:20216933~menuPK:400482~pageP K:148956~piPK:216618~theSitePK:400476,00.html chapter link_ http://siteresources.worldbank.org/INTPAH/Resources/P ublictions/459843-1195594469249/HealthEquityCh7.pdf [29] Iqbal, J.M. (2007) In defence of Marxism, Bangladesh and the crisis over the caretaker government. http://www.marxist.com/bangladesh-crisis-caretaker-gov  J. Shabnam et al. / Health 3 (2011) 762-771 Copyright © 2011 SciRes. http://www.scirp.org/journal/HEALTH/Openly accessible at 771771 ernment170107.htm [30] Ikeako, L.C., Onah, H.E. and Iloabachie, G.C. (2006) Influence of formal maternal education on the use of for- mal maternity services in Inagu, Nigeria. Journal of Ob- stetrics & Gynaecology, 26, 30-34. doi:10.1080/01443610500364004 [31] Mekonnen, Y. and Mekonnen, A. (2003) Factors influ- encing the use of maternal health care services in Ethio- pia. Journal of Health, Population and Nutrition, 21, 374-382. [32] UNICEF (2010) Bangladesh: Statistics. Education. http://www.unicef.org/infobycountry/bangladesh_bangla desh_statistics.html [33] Bangladesh Bureau of Educational Information and Sta- tistics (2006). http://www.banbeis.gov.bd/bd_pro.htm [34] Nahar, S. and Costello, A. (1998) The hidden cost of “free” maternity care in Dhaka, Bangladesh. Health Pol- icy Plan, 13, 417-422. doi:10.1093/heapol/13.4.417 [35] Killingsworth, J.R., Hossain, N., Hedrick-Wong, Y., Thomas, S.D., Rahman, A. and Begum, T. (1999) Unof- ficial fees in Bangladesh: Price, equity and institutional issues. Health Policy Plan, 14, 152-163. doi:10.1093/heapol/14.2.152 [36] Pathak, P.K., Singh, A. and Subramanian, S.V. 2010) Economic inequalities in maternal health care: Prenatal care and skilled birth attendance in India, 1992-2006. PLoS ONE, 27, e13593. doi:10.1371/journal.pone.0013593 [37] Chakraborty, N., Islam, M.A., Chowdhury, R.I., Bari, W. and Akhter, H.H. (2003) Determinants of the use of ma- ternal health services in rural Bangladesh. Health Promo- tion International, 18, 327-337. doi:10.1093/heapro/dag414 [38] Anwar, I., Kalim, N. and Koblinsky, M. (2009) Quality of obstetric care in public-sector facilities and constraints to implementing emergency obstetric care services: Evi- dence from high- and low-performing districts of Bang- ladesh. Journal of Health, Population and Nutrition, 27, 139-155. doi:10.3329/jhpn.v27i2.3327
|