 Vol.1, No.3, 139-145 (2009) doi:10.4236/health.2009.13023 SciRes Copyright © 2009 Openly accessible at http://www.scirp.org/journal/HEALTH/ Health Long-term survival and prognostic implications of Chinese type 2 diabetic patients with coronary artery disease after coronary artery bypass grafting Ming C Hsiung1, Tao-Hsin Tung2, Chung-Yi Chang3, Yi-Cheng Chuang3, Kuo-Chen Lee3, Sung-How Sue3, Yi-Pen Chou4, Richard Hsiung1, Chien-Ming Huang1, Chang-Chyi Lin1, Wei-Hsian Yin1, Mason S Young1, Jeng Wei3* 1Division of Cardiology, Department of Medicine, Cheng-Hsin General Hospital, Taipei, Taiwan 2Department of Medicine Research and Education, Cheng-Hsin General Hospital, Taipei, Taiwan 3Division of Cardiovascular Surgery, Cheng-Hsin General Hospital, Taipei, Taiwan; ch2876@chgh.org.tw 4Department of Anesthesiology, Cheng-Hsin General Hospital, Taipei, Taiwan *Corresponding author Received 13 August 2009; revised 11 September 2009; accepted 14 September 2009. ABSTRACT This study was conducted to determine the sur- vival rates of type 2 diabetic patients after coro- nary artery bypass grafting (CABG) surgery, and the prognostic factors related to all-cause mor- tality during a 7-year follow-up. The medical re- cords of 816 type 2 diabetic patients who un- derwent primary, isolated CABG surgery during 1997-2003 were studied. The Kaplan-Meier me- thod and Cox regression were used to estimate survival and the independence of prognostic factors associated with all-cause mortality. One hundred and five out of 816 patients expired during the 7-year period. The overall survival rate was 83.5% (95%CI: 78.7-88.3%). Associated prog- nostic factors varied by gender. For males, but not for females, smoking (RR=3.44, 95%CI: 1.01- 11.70), myocardial infarction (RR=4.77, 95% CI: 1.23-18.86), respiratory failure (RR=4.21, 95% CI: 1.48-7.99), cardiogenic shock (RR=12.58, 95% CI: 3.25-20.77), and congestive heart failure (RR= 3.77, 95%CI: 1.10-13.45) were significantly related to all-cause mortality. Older age at sur- gery (RR= 1.15, 95%CI: 1.04-1.27), emergent op- eration (RR= 21.29, 95%CI: 10.03-39.43), pul- monary ede-ma (RR=7.72, 95%CI: 1.89-15.59), and days of ICU stay (RR=1.05, 95%CI: 1.02-1.09) were significant- ly related to all-cause mortality in females only. In conclusion, several gen- der-related differences were noted pertaining to all-cause mortality and its relationship to smok- ing, myocardial infarction, respiratory failure, cardiogenic shock, congestive heart failure, older age at surgery, emergent operation, pul- monary edema, and days of ICU stay. Keywords: Coronary Artery Bypass Grafting; Gender Difference; Prognostic Factors; Survival; Type 2 Diabetes 1. INTRODUCTION Diabetes mellitus is viewed as a major risk factor for car- diovascular disease, and coronary heart disease is the leading cause of death in adult diabetics [1]. In general, around 20% of patients undergoing coronary artery bypass surgery (CABG) suffer from diabetes mellitus [1]. In ad- dition, diabetics have a higher mortality than patients without diabetes after CABG surgery [2,3]. Choosing this type of surgical therapy for patients depends on the esti- mate of the risk of the procedure and the possible benefits compared with alternative forms of therapy. Long-term outcome among diabetics with coronary artery disease (CAD) after CABG is associated with severity of diabetes at the time of surgery [4]. This observation suggests that early detection of this disorder followed by early treatment could improve both survival and quality of life. In Taiwan, the remarkable economic achievements of the last 40 years have resulted in a great improvement in living standards and in an increase in life expectancy. Type 2 diabetes in adults is one of the global public health problems in the Taiwanese population. Screening for type 2 diabetes by the natural history of diabetes, fasting plasma glucose (FPG), and oral glucose tolerance test (OGTT) showed the overall prevalence of type 2 diabetes in Taiwan to be 5-9% and 11-13% for residents above 20 or 40 years of age, respectively [5-11]. From the view- point of evidence-based medicine, it is not only important to be cognizant of the long-term survival of diabetic pa- tients after CABG, but also to explore the complete spectrum of demographic and biological markers that  M. C. Hsiung et al. / HEALTH 1 (2009) 139-145 SciRes Copyright © 2009 Openly accessible at http://www.scirp.org/journal/HEALTH/ 140 may be related to survival rate. To the best of our know- ledge, the long-term survival of Chinese type 2 diabetic patients with CAD undergoing CABG surgery has not been carefully examined. Some uncertainty still exists regarding the influence of gender on long-term survival and on associated risk factors for long-term survival for these patients after CABG surgery. Thus, in order to de- termine the long-term survival of and associated risk factors for diabetic patients after CABG surgery, a long- term survival study was performed. Because long-term prognosis after CABG surgery in relation to gender has not been closely evaluated among type 2 diabetic patients in Taiwan, the present study was designed to explore the possibility of gender-related dif- ferences in risk factors, because such differences might have important implications for understanding the value of individual prognostic factors for estimation of long- term survival of diabetic patients after surgery. The pur- pose of this study was to determine the long-term (7-year follow-up) survival rate of each gender after primary, isolated CABG surgery, and to identify the associated prognostic factors related to all-cause mortality among Chinese type 2 diabetic patients. 2. MATERIALS AND METHODS 2.1. Patient Population Between January 1997 and December 2003, a total of 898 type 2 diabetic patients with CAD underwent CABG surgery at the Division of Cardiovascular Surgery and Heart Center, Cheng-Hsin General Hospital, a fully cer- tified regional and teaching hospital with 757 beds in Taipei, Taiwan. Of the 898 type 2 diabetic patients, 66 (7.3%) were excluded due to simultaneous valve surgery and another 16 (1.8%) patients were excluded due to repeated CABG surgery. The remaining 816 patients who underwent primary, isolated CABG surgery because of CAD without concomitant valve procedures and without previous history of CABG participated in the evaluation. Seventy-one per cent (581/816) of these participants were males. 2.2. Data Collection Patients’ demographic characteristics and surgical vari- ables were retrieved from medical records and computer files. The hospital records of each diabetic patient were reviewed by well trained, senior chart reviewers using a standard data collection form. Demographic information, presence of pre-existing co-morbidities and associated medications at admission and discharge were obtained from the nursing and medical histories. Indicators of postoperative recovery and complications were identified from the details of patient’s progress notes. Subjects were divided into three categories according to smoking or alcohol drinking: current users, ex-users, and non users. We combined current users and ex-users as the user group. The identification of type 2 diabetes was based on the WHO definition in 1999 [12]: subjects with FPG126 mg/dl or 2 h post-load 200mg/dl were defined as indi- viduals with type 2 diabetes. Hypertension was defined as systolic blood pressure 140 mmHg or diastolic blood pressure 90 mmHg [13]. Hyperlipidaemia was defined as one or more of the following: total cholesterol 200 mg/dl; triglyceride 200 mg/dl; HDL < 35 mg/dl [14]. Subjects featuring a personal disease history of type 2 diabetes, hypertension, or hyperlipidaemia and who had received medication to treat such conditions were viewed as “known cases” of such disease. In addition, for diabetic patients after CABG who died in the hospital, case re- cords such as autopsy findings were used for information about the causes of death. For those patients who died outside the hospital, information including autopsy find- ings, scheduled investigations, and death certificates were collected. In addition, access to hospital records was approved by the hospital human subjects review board at Cheng-Hsin General Hospital. 2.3. Operative Technique The operative procedures for CABG surgery have been described in previous studies [15-17]. The CABG opera- tions were performed by means of a median sternotomy with the aid of extracorporeal cardiopulmonary bypass hemodilution (hematocrit, 25% to 30%) and moderate hypothermia (25 to 28C). Cardiopulmonary bypass used an ascending aortic cannula followed by a two-stage venous cannula. Myocardial preservation was achieved with a hypercalcemic, hypothermic crystalloid solution and external cooling with ice slush or a cold saline solu- tion. Crystalloid cardioplegia was infused through the aortic root at least every 20 minutes and was infused into each completed vein graft in addition to the aortic root infusion. Blood cardioplegia was usually used for patients with left ventricular hypertrophy, cardiogenic shock, or acutely occluded coronary arteries. Venting was per- formed primarily via the aorta, and if necessary, via the pulmonary artery. The myocardial temperature was monitored and kept below 15C. After completion of all distal anastomoses, the patient was warmed systemically to 37C, while warm cardioplegic solution followed by warm blood was given by the antegrade method. 2.4. Statistical Analysis Statistical analysis was performed using SAS software. Prognostic predictors and all-cause mortality were de- termined by univariate and multivariate techniques. In the univariate analysis, chi-square testing or two-sample  M. C. Hsiung et al. / HEALTH 1 (2009) 139-145 SciRes Copyright © 2009 Openly accessible at http://www.scirp.org/journal/HEALTH/ 141 Table 1. Comparison of baseline characteristics among type 2 diabetic patients with CAD after CABG surgery (n=816). Male (n=581) Female (n=235) Total (n=816) n (%) n (%) n (%) p-value for t-test or 2-test Categorical variables Known case of diabetes 385 (66.3) 165 (70.2) 550 (67.4) 0.28 Emergent operation 2 (0.3) 3 (1.3) 5 (0.6) 0.12 Smoking 160 (27.5) 27 (11.5) 187 (22.9) <0.0001 Alcohol drinking 82 (14.1) 16 (6.8) 98 (12.0) 0.005 MI (Inferior or Posterior) 227 (39.1) 77 (32.7) 304 (37.3) 0.09 Hypertension 417 (71.8) 185 (78.7) 602 (73.8) 0.04 Hyperlipidemia 227 (39.1) 90 (38.3) 317 (38.9) 0.84 COPD 36 (6.2) 14 (6.0) 50 (6.1) 0.90 PAOD 24 (4.1) 16 (6.8) 40 (4.9) 0.11 Pulmonary edema 53 (9.1) 32 (13.6) 85 (10.4) 0.06 Old CVA 74 (12.7) 32 (13.6) 106 (13.0) 0.73 Renal failure 82 (14.1) 49 (20.9) 131 (16.1) 0.02 Sepsis 8 (1.4) 6 (2.6) 14 (1.7) 0.24 UGI bleeding 9 (1.6) 4 (1.7) 13 (1.6) 0.87 Respiratory failure 26 (4.5) 10 (4.3) 36 (4.5) 0.93 Cardiogenic shock 39 (6.7) 11 (4.7) 50 (6.1) 0.30 Unstable angina 194 (33.4) 92 (39.1) 286 (35.0) 0.08 Pre PTCA 102 (17.6) 31 (13.2) 133 (16.3) 0.16 CHF 62 (10.7) 25 (10.6) 87 (10.7) 0.94 Type of bypass (arterial/venous) 464/117 (79.9 /20.1) 162/73 (68.9 /31.1) 626/190 (76.7 /23.3) 0.001 Continuous variables Duration of diabetes 12.644.85 14.785.32 13.574.97 0.01 Operation age (yrs) 64.0210.05 66.508.18 64.749.61 0.0003 FPG (mg/dl) 169.1107.6 201.2106.6 178.498.2 0.002 HbA1c (%) 8.22.0 8.41.9 8.22.0 0.54 SBP(mmHg) 135.020.7 141.122.2 136.921.4 0.02 DBP(mmHg) 76.711.9 77.313.8 75.912.6 0.11 BMI (Kg/m2) 26.717.8 24.94.2 26.115.0 0.15 Cholesterol (mg/dl) 189.344.3 204.3131.8 193.950.0 0.002 Triglyceride (mg/dl) 190.2147.0 204.960.4 194.3142.8 0.32 BUN (mg/dl) 23.417.6 24.415.0 23.716.8 0.56 Creatinine (mg/dl) 1.701.92 1.610.68 1.670.85 0.63 Uric acid (mg/dl) 7.55.6 7.56.5 7.55.9 0.91 AST (U/L) 50.057.0 42.541.5 47.864.8 0.37 ALT (U/L) 40.6107.0 38.625.5 37.291.6 0.19 HDL(mg/dl) 38.511.7 49.967.5 41.636.7 0.09 LDL (mg/dl) 125.438.0 131.848.1 127.141.0 0.18 RBC (103/ul) 4.33.0 4.03.7 4.33.2 0.28 WBC (103/ul) 9.44.5 15.975.4 11.340.6 0.10 Hs-CRP(mg/dl) 0.1890.177 0.1790.164 0.1850.152 0.51 Ischaemic time (min) 61.6441.01 65.1538.65 62.6540.35 0.26 Cardiopulmonary bypass time (min) 104.9968.65 111.9167.68 106.9868.40 0.19 CAD number 2.830.44 2.740.54 2.800.47 0.02 CABG number 3.130.97 3.011.02 3.100.99 0.12 Pre-operation LVEF (%) 50.9319.68 54.0919.91 51.8419.78 0.03 Post-operation LVEF (%) 55.2517.24 57.7218.58 56.0117.68 0.17 ICU stay (days) 6.447.17 8.6413.88 7.089.64 0.02 CAD: coronary artery disease, CABG: coronary artery bypass grafting, MI: myocardial infarction, COPD: chronic obstructive pulmonary disease, PAOD: peripheral arterial occlusive disease, CVA: cerebrovascular accident, PTCA: percutaneous transluminal coronary angioplasty, CHF: congestive heart failure. 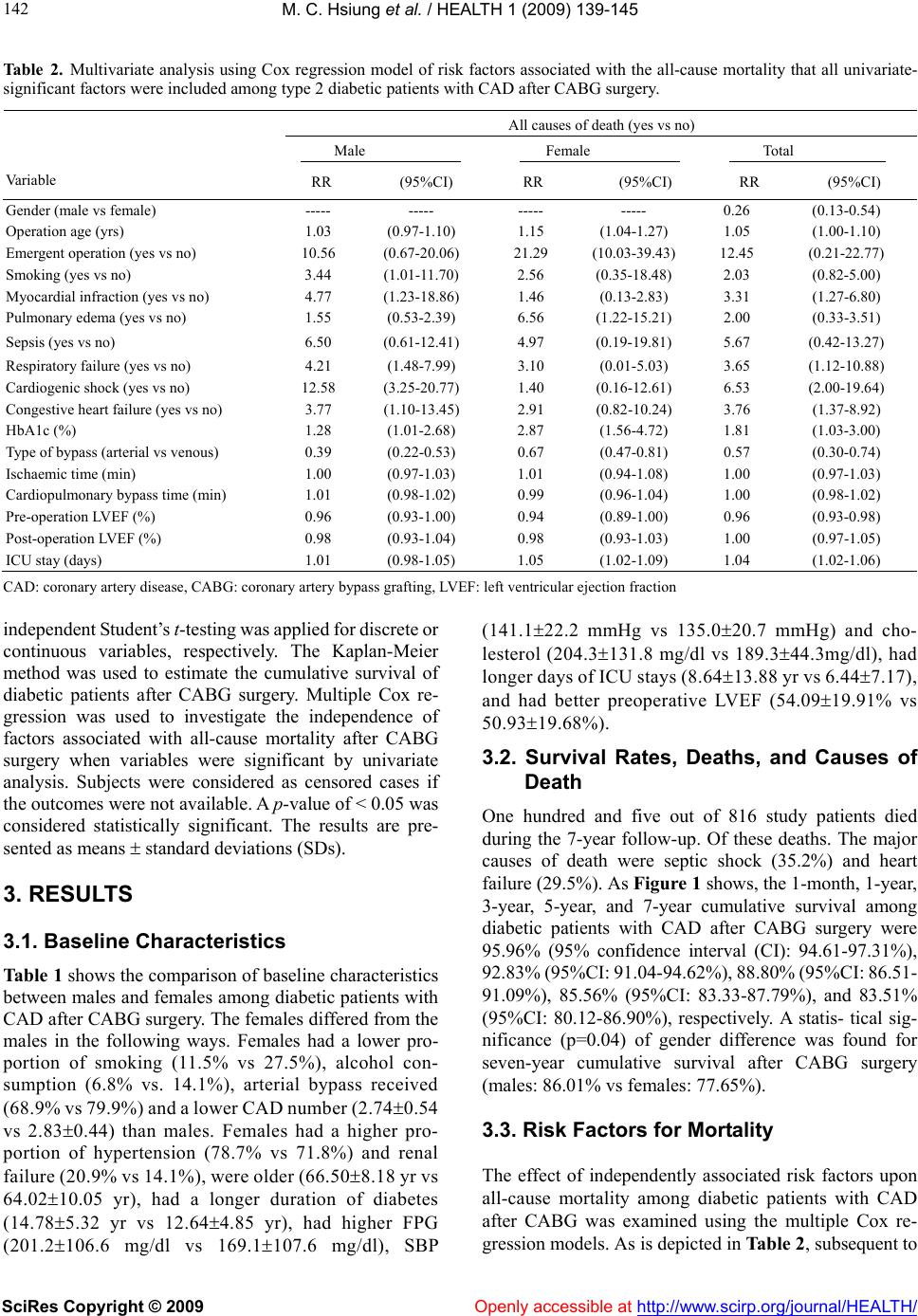 M. C. Hsiung et al. / HEALTH 1 (2009) 139-145 SciRes Copyright © 2009 http://www.scirp.org/journal/HEALTH/Openly accessible at 142 Table 2. Multivariate analysis using Cox regression model of risk factors associated with the all-cause mortality that all univariate- significant factors were included among type 2 diabetic patients with CAD after CABG surgery. All causes of death (yes vs no) Male Female Total Va ri abl e RR (95%CI) RR (95%CI) RR (95%CI) Gender (male vs female) ----- ----- ----- ----- 0.26 (0.13-0.54) Operation age (yrs) 1.03 (0.97-1.10) 1.15 (1.04-1.27) 1.05 (1.00-1.10) Emergent operation (yes vs no) 10.56 (0.67-20.06) 21.29 (10.03-39.43) 12.45 (0.21-22.77) Smoking (yes vs no) 3.44 (1.01-11.70) 2.56 (0.35-18.48) 2.03 (0.82-5.00) Myocardial infraction (yes vs no) 4.77 (1.23-18.86) 1.46 (0.13-2.83) 3.31 (1.27-6.80) Pulmonary edema (yes vs no) 1.55 (0.53-2.39) 6.56 (1.22-15.21) 2.00 (0.33-3.51) Sepsis (yes vs no) 6.50 (0.61-12.41) 4.97 (0.19-19.81) 5.67 (0.42-13.27) Respiratory failure (yes vs no) 4.21 (1.48-7.99) 3.10 (0.01-5.03) 3.65 (1.12-10.88) Cardiogenic shock (yes vs no) 12.58 (3.25-20.77) 1.40 (0.16-12.61) 6.53 (2.00-19.64) Congestive heart failure (yes vs no) 3.77 (1.10-13.45) 2.91 (0.82-10.24) 3.76 (1.37-8.92) HbA1c (%) 1.28 (1.01-2.68) 2.87 (1.56-4.72) 1.81 (1.03-3.00) Type of bypass (arterial vs venous) 0.39 (0.22-0.53) 0.67 (0.47-0.81) 0.57 (0.30-0.74) Ischaemic time (min) 1.00 (0.97-1.03) 1.01 (0.94-1.08) 1.00 (0.97-1.03) Cardiopulmonary bypass time (min) 1.01 (0.98-1.02) 0.99 (0.96-1.04) 1.00 (0.98-1.02) Pre-operation LVEF (%) 0.96 (0.93-1.00) 0.94 (0.89-1.00) 0.96 (0.93-0.98) Post-operation LVEF (%) 0.98 (0.93-1.04) 0.98 (0.93-1.03) 1.00 (0.97-1.05) ICU stay (days) 1.01 (0.98-1.05) 1.05 (1.02-1.09) 1.04 (1.02-1.06) CAD: coronary artery disease, CABG: coronary artery bypass grafting, LVEF: left ventricular ejection fraction independent Student’s t-testing was applied for discrete or continuous variables, respectively. The Kaplan-Meier method was used to estimate the cumulative survival of diabetic patients after CABG surgery. Multiple Cox re- gression was used to investigate the independence of factors associated with all-cause mortality after CABG surgery when variables were significant by univariate analysis. Subjects were considered as censored cases if the outcomes were not available. A p-value of < 0.05 was considered statistically significant. The results are pre- sented as means standard deviations (SDs). 3. RESULTS 3.1. Baseline Characteristics Table 1 shows the comparison of baseline characteristics between males and females among diabetic patients with CAD after CABG surgery. The females differed from the males in the following ways. Females had a lower pro- portion of smoking (11.5% vs 27.5%), alcohol con- sumption (6.8% vs. 14.1%), arterial bypass received (68.9% vs 79.9%) and a lower CAD number (2.740.54 vs 2.830.44) than males. Females had a higher pro- portion of hypertension (78.7% vs 71.8%) and renal failure (20.9% vs 14.1%), were older (66.508.18 yr vs 64.0210.05 yr), had a longer duration of diabetes (14.785.32 yr vs 12.644.85 yr), had higher FPG (201.2106.6 mg/dl vs 169.1107.6 mg/dl), SBP (141.122.2 mmHg vs 135.020.7 mmHg) and cho- lesterol (204.3131.8 mg/dl vs 189.344.3mg/dl), had longer days of ICU stays (8.6413.88 yr vs 6.447.17), and had better preoperative LVEF (54.0919.91% vs 50.9319.68%). 3.2. Survival Rates, Deaths, and Causes of Death One hundred and five out of 816 study patients died during the 7-year follow-up. Of these deaths. The major causes of death were septic shock (35.2%) and heart failure (29.5%). As Figure 1 shows, the 1-month, 1-year, 3-year, 5-year, and 7-year cumulative survival among diabetic patients with CAD after CABG surgery were 95.96% (95% confidence interval (CI): 94.61-97.31%), 92.83% (95%CI: 91.04-94.62%), 88.80% (95%CI: 86.51- 91.09%), 85.56% (95%CI: 83.33-87.79%), and 83.51% (95%CI: 80.12-86.90%), respectively. A statis- tical sig- nificance (p=0.04) of gender difference was found for seven-year cumulative survival after CABG surgery (males: 86.01% vs females: 77.65%). 3.3. Risk Factors for Mortality The effect of independently associated risk factors upon all-cause mortality among diabetic patients with CAD after CABG was examined using the multiple Cox re- gression models. As is depicted in Table 2, subsequent to  M. C. Hsiung et al. / HEALTH 1 (2009) 139-145 SciRes Copyright © 2009 Openly accessible at http://www.scirp.org/journal/HEALTH/ 143 143 0 10 20 30 40 50 60 70 80 90 100 01234567 year survival (%) Total (105/816) Male(68/581) Female(37/235) Figure 1. Seven-year cumulative survival among type 2 dia- betic patients with CAD after CABG surgery in males versus females. adjustment for confounding factors, gender (male vs. female, RR=0.26, 95%CI: 0.13-0.54), age at surgery (RR=1.05, 95%CI: 1.00-1.10), respiratory failure (yes vs. no, RR=3.65, 95%CI: 1.12-10.88), cardiogenic shock (yes vs. no, RR=6.53, 95%CI: 2.00-19.64), congestive heart failure (yes vs. no, RR=3.76, 95%CI: 1.37-8.92), HbA1c (RR=1.81, 95%CI: 1.03-3.00), type of bypass (arterial vs venous, RR=0.57, 95%CI: 0.30-0.74), preop- erative LVEF (RR=0.96, 95%CI: 0.93-0.98), and days of ICU stay (RR=1.04, 95%CI: 1.02-1.06) appeared to be statistically significantly related to all-cause mortality. The dramatically different results of multiple Cox re- gression analyses of the data stratified by gender also show in Table 2. 4. DISCUSSION 4.1. Implications of Gender Difference as Regards Associated Risk Factors for All-Cause Mortality Diabetes is known as a determinant of prognosis in CAD and may pose an increased risk for major complications during CABG surgery [3,18]. Diabetic patients represent about 20% of patients undergoing CABG surgery [19]. Although previous studies have shown that diabetic pa- tients with CAD have worse long-term survival after CABG than non-diabetics [1,2], the plausible biological mechanisms that could link diabetes to the early and late outcome of CABG remain uncertain. The extent of vas- cular compromise in diabetes is of particular relevance in CAD patients, as it might account for the more severe coronary artery pathology and might also impair the biological integrity of the bypass grafts [3,20,21]. Pre- served functional and structural properties of CABG conduits are essential for a successful myocardial revas- cularization [3,21]. The continuing surgical and technical improvements in the operative management of CAD patients who undergo CABG surgery, as well as consistently better anesthetic and postoperative care, might have made it difficult to identify any specific gender-related risk factors associ- ated with all-cause mortality. However, our results showed that diabetic females with CAD who were re- ferred for CABG surgery clearly differed from males in that they were older and had a higher proportion of hy- pertension and renal failure. This finding not only implies that females were at a later disease stage or had more serious symptoms than males before being referred for CABG surgery, but also that associated chronic diseases were major risk indicators for females with CAD [17,22]. In addition, females more frequently had renal dysfunc- tion. To some extent, this might be explained by older age and more frequent histories of personal disease such as diabetes mellitus and hypertension [22]. In the present study, female diabetic patients with CAD had slightly elevated all-cause mortality during the 7-year study when compared to male patients. Our findings are in agreement with previous experiences focused on all CAD population that showed gender differences in late mortality [17,22]. They are also in agreement with a large study taking major risk factors into account that showed that there were no substantial differences in the long-term survival of males and females after CABG surgery [22]. Although there seem to be only small differences overall in long-term survival after CABG surgery between males and females, there may be greater gender differences in specific patient subgroups. But after adjustment for con- founding factors, female sex was still independently as- sociated with all-cause mortality in the current study. This difference between male and female may become of greater importance than in earlier times because the population of patients undergoing CABG surgery has aged, there are more patients with abnormal pre- and postoperative LVEF and the patient populations have more diffuse diseases [16,22]. It should be noted that a difference in survival rates in females and males occurs after CABG surgery about 4 to 5 years in this study. Previous studies have also shown that after adjustment for all independent predictors of long-term mortality, female sex was an independent pre- dictor of improved 5-year survival [23]. While the in- formation yielded by univariate analyses was valuable, the relationships between predictors and all-cause mor- tality among diabetic patients with CAD after CABG surgery were far too complex to be answered completely by univariate analysis. It has been well documented in many academic studies that females presenting for CABG have a vastly different preoperative risk profile than that of their male counterparts [23]. The risk profiles of males and female are quite different and indicate that although it is usually appropriate to directly compare the two groups, male and female, with respect to a specific predictor, the predictor might be inappropriate. The use of multivariate models is particularly important because they fully ac- p-value for log-rank test=0.04  M. C. Hsiung et al. / HEALTH 1 (2009) 139-145 SciRes Copyright © 2009 Openly accessible at http://www.scirp.org/journal/HEALTH/ 144 count for all related important risk factors. In this study, some risk factors for all-cause mortality were detrimental to males and others were more detrimental to females after CABG surgery. Greater adverse preoperative char- acteristics such as diabetic females being older and hav- ing more associated diseases can be suggested as one explanation of the higher mortality rates among female. Since female gender was an independent predictor of all-cause mortality in the multivariate analysis, discrep- ancies in preoperative demographic or clinical charac- teristics could only explain part of the increased mortality rates among diabetic females after CABG surgery. However, dissimilarities in profiles between female and male diabetic patients might contribute to the debate about the gender difference in outcome after CABG sur- gery [23,24]. In addition, increased mortality among female patients was probably due to the fact that females had more comorbid conditions than did men at the time of referral, perhaps because they were not being evaluated aggressively enough [25]. From the viewpoint of pre- ventive medicine, although discrepancies suggest that associated predictive variables for long-term survival after CABG surgery differ between hospitals and could change with time, regular identification of risk factors makes it possible to focus attention on current problems to minimize surgical risk and reduce mortality, especially among females. Clinical decision making and follow-up should also not be influenced by stereotypes but by spe- cific findings. 4.2. Methodological Considerations Although based on the follow-up study design, that is, being prospective in design as well as including all dia- betic patients with CAD who underwent CABG surgery in a well defined patient population for 7 years, we not only determined the hospital mortality, but also further explored the cumulative survival and prognostic factors related to all-cause mortality among diabetic patients with CAD after CABG surgery. The present study still has some limitations that need to be considered while as- sessing the results. First, some of the clinical variables obtained from medical records could have resulted in misclassification bias. Nevertheless, it seems reasonable to assume that if misclassification bias was present, it was not related to gender and all-cause mortality, thus could be viewed as nondifferential misclassification. Second, potential Berkson’s bias (selection bias) was inevitable due to the hospital-based study design. This population was not only not exactly representative of the whole general population, but it was also difficult to estimate the survival of a matched total population sample in Taiwan, preferably in the region of Taipei. Third, due to having no information on the quantity and duration of some risk factors such as smoking and alcohol drinking, we could not clarify the dose-response effect between specific personal habits and all-cause mortality. Fourth, the female sample size might not be large enough to identify the exact confidence interval of related prognostic factors. Further studies should be conducted with larger sample sizes for female to re-examine gender-specific prognostic factors for long-term survival among diabetic patients with CAD after CABG surgery. 5. CONCLUSIONS The all-cause mortality of diabetic patients with CAD after CABG surgery and several gender-related differ- ences pertaining to all-cause mortality were investigated, including the relationships between all-cause mortality and smoking, myocardial infarction, cardiogenic shock, respiratory failure, congestive heart failure, older age at surgery, emergent operation, pulmonary edema, and days of ICU stay. In order to increase long-term survival among diabetic patients with CAD, adequate diagnosis and treatment risk factors after CABG surgery are essen- tial. 6. ACKNOWLEDGEMENTS This study was presented partly in the 2nd International Congress on “PREDIABETES and the METABOLIC SYNDROME”, Barcelona, Spain, 2007. REFERENCES [1] T. Hakala, O. Pitkanen, P. Halonen, et al., (2005) Early and late outcome after coronary bypass surgery in diabetic patients. Scand Cardiovasc J, 39(3), 177-181. [2] A. M. Calafiore, M. Di Mauro, G. Di Giammarco, et al., (2003) Effect of diabetes on early and late survival after isolated first coronary bypass surgery in multivessel dis- ease. J Thorac Cardiovasc Surg, 125(1), 144-154. [3] V. H. Thourani, W. S. Weintraub, B. Stein, et al., (1999) Influence of diabetes mellitus on early and late outcome after coronary artery bypass grafting. Ann Thorac Surg, 67(4), 1045-1052. [4] T. Ono, J. Kobayashi, Y. Sasako, et al., (2002) The impact of diabetic retinopathy on long-term outcome following coronary artery bypass graft surgery, J Am Coll Cardiol, 40(3), 428-436. [5] J. D. Lin, W. B. Shieh, M. J. Huang, et al., (1993) Diabetes mellitus and hypertension based on the family history and 2-h postprandial blood sugar in the Ann-Lo district (Northern Taiwan). Diabetes Res Clin Pract, 20(1), 75-85. [6] C. L. Li, S. T. Tsai, P. Chou, et al., (1999) Comparison of the results between two diagnostic criteria by ADA and WHO among subjects with FPG 5.6-7.8 mmol/l in Kin-Hu and Kin-Chen, Kinmen, 1991-94. Diabetes Res Clin Pract, 45(1), 51-59. [7] P. Chou, M. J. Liao, H. S. Kuo. et al., (1994) A population survey on the prevalence of diabetes in Kin-Hu, Kinmen. Diabetes Care, 17(9), 1055-1058. [8] P. Chou, C. L. Li, H. S. Kuo, et al., (1997) Comparison of the prevalence of two diabetes surveys between 1987-88  M. C. Hsiung et al. / HEALTH 1 (2009) 139-145 SciRes Copyright © 2009 http://www.scirp.org/journal/HEALTH/Openly accessible at 145 145 and 1991-92 in Pu-Li, Taiwan. Diabetes Res Clin Pract, 38(1), 61-67. [9] H. D. Chen, C. K. Shaw, W. P. Tseng, et al., (1997) Prevalence of diabetes mellitus and impaired glucose tol- erance in Aborigines and Chinese in eastern Taiwan. Diabetes Res Clin Pract, 38(3), 199-205. [10] F. H. Lu, Y. C. Yang, J. S. Wu, et al., (1998) A popula- tion-based study of the prevalence and associated factors of diabetes mellitus in southern Taiwan. Diabetes Med, 15(7), 564-572. [11] K. T. Chen, C. J. Chen, E. W. Gregg, et al., (1999) High prevalence of impaired fasting glucose and type 2 diabetes mellitus in Penghu Islets, Taiwan: evidence of a rapidly emerging epidemic? Diabetes Res Clin Pract, 44(1), 59-69. [12] World Health Organization, (1999) Definition, diagnosis and classification of diabetes mellitus and its complica- tions: Report of a WHO Consultation, Part 1, Diagnosis and classification of diabetes mellitus, Geneva, World Health Organization. [13] Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure, (1997) The sixth report of the joint national committee on pre- vention, detection, evaluation, and treatment of high blood pressure. Arch Intern Med, 157(21), 2413-2446. [14] C. M. Liu, T. H. Tung, J. H. Liu, et al., (2005) A commu- nity-based epidemiological study of elevated serum alanine aminotransferase levels in Kinmen, Taiwan. World J Gastroenterol, 11(11), 1616-1622. [15] C. H. Huang, S. T. Lai, and Z. C. Weng, (2001) Risk factors for mortality in primary isolated coronary artery bypass grafting surgery. J Formos Med Assoc, 100(5), 299-303. [16] C. H. Huang, C. P. Hsu, S. T. Lai, et al., (2004) Operative results of coronary artery bypass grafting in women. Int J Cardial, 94(1), 61-66. [17] M. C. Hsiung, J. Wei, C. Y. Chang, et al., (2006) Long- term survival and prognostic implications after coronary artery bypass grafting in Chinese patients with coronary artery disease. Acta Cardiol, 61(5), 519-524. [18] W. Whang and J. T. Bigger, (2000) Diabetes and outcomes of coronary artery bypass graft surgery in patients with se- vere left ventricular dysfunction: results from the CABG Patch trial database, The CABG Pateh Trial Investigators and Coordinators. J Am Coll Cardiol, 36(4), 1166-1172. [19] C. Rajakaruna, C. A. Rogers, C. Suranimala, et al., (2006) The effect of diabetes mellitus on patients undergoing coronary surgery: A risk-adjusted analysis. J Thorac Car- diovasc Surg, 132(4), 802-810. [20] R. Lorusso, S. Pentiricci, R. Raddino, et al., (2003) In- fluence of type 2 diabetes on functional and structural properties of coronary artery bypass conduits. Diabetes, 52(11), 2814-2820. [21] J. G. Motwani and E. J. Topol, (1998) Aortocoronary saphenous cein graft disease: Pathogenesis, predisposition and prevention. Circulation, 97(9), 916-931. [22] G. Brandrup-Wognsen, H. Berggren, M. Hartford, et al., (1996) Female sex is associated with increased mortality and morbidity early, but not late, after coronary artery bypass grafting. Eur Heart J, 17(9), 1426-1431. [23] I. K. Toumpoulis, C. E. Anagnostopoulos, S. K. Balaram, et al., (2006) Assessment of independent predictors for long-term mortality between women and men after coro- nary artery bypass grafting: Are women different from men? J Thorac Cardiovasc Surg, 131(2), 343-351. [24] C. D. Naylor and C. M. Levinton, (1993) Sex-related difference in coronary revascularization practices: the perspective from a Canadian queen management project. Can Med Assoc J, 149(7), 965-973. [25] M. R. Williams, A. F. Choudhri, D. L. Morales, et al., (2000) Gender differences in patients undergoing coro- nary artery bypass surgery, from a mandatory statewide database. J Gend-Specif Med, 3(1), 41-48.
|