H. Ueda et al. / Open Journal of Stomatology 1 (2011) 165-167
166
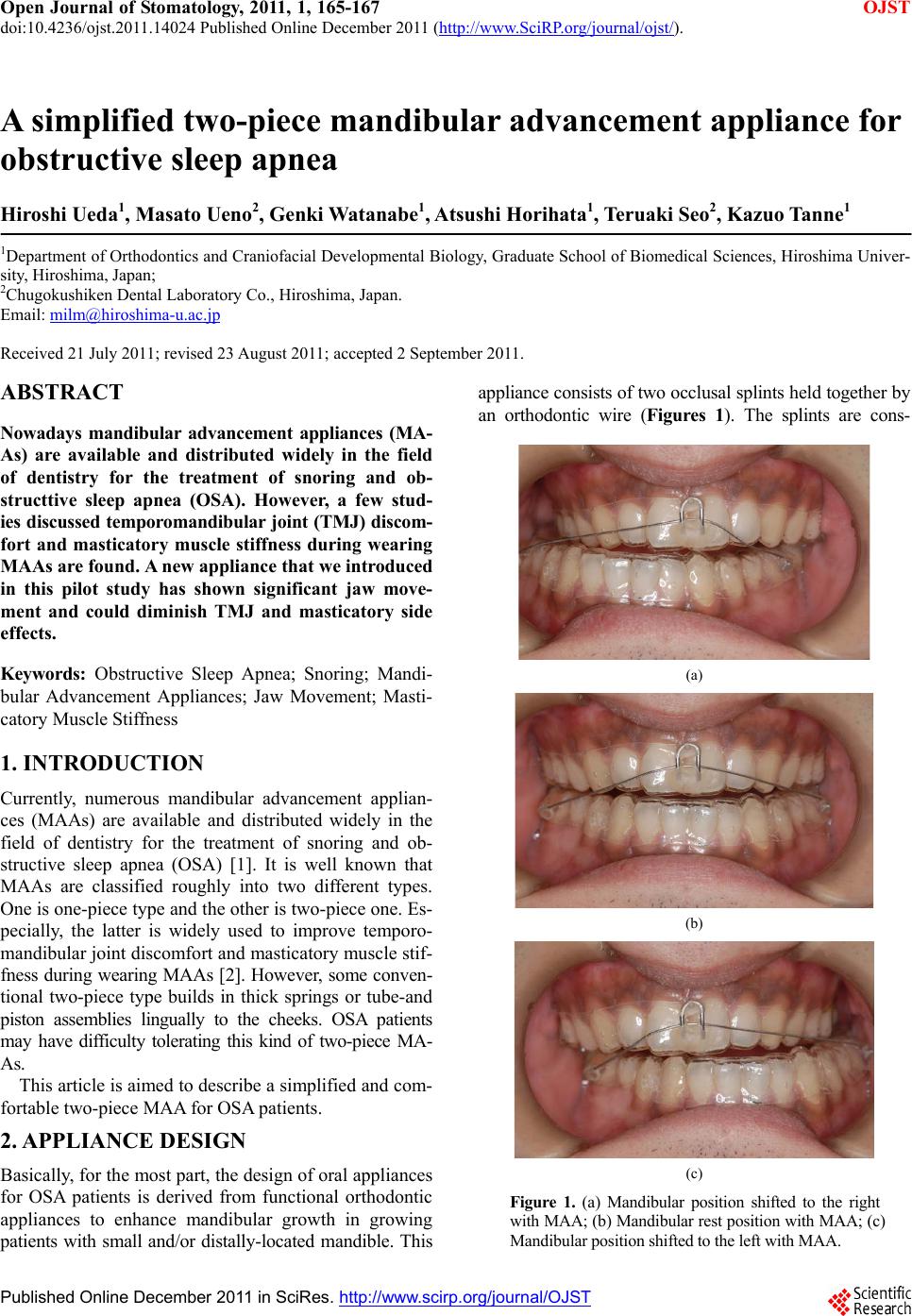
tructed of a 0.75 mm thick acrylic resin that provides full
occlusal coverage of teeth. A 0.0175 multi-stranded and
twist wire is attached on the buccal sides of the lower
splint (Figure 2). Patients can connect the lower splint
easily with the hook attached on the front portion of the
upper splint. The initial mandibular advancement was
defined as two-thirds of maximum mandibular forward
position with a 3 - 4 mm vertical opening at the anterior
teeth. This appliance can permit patients to freely move
the jaw horizontally (approximatel y 10 mm in the lateral
direction) and at the same time prevent the mandible to
move downward within 2 mm in the supine position by
means of an optoelectric jaw-tracking system with six
degrees of freedom (Gnathohexagraph system II, Ono-
sokki Co., Yokohama, Japan) (Table 1).
The mandibular position can also be titrated forward
from its initial position by adjusting the wire length on
the appliance.
Figure 2. Upper and lower plates of MAA.
Tab le 1. The distance of mandib ular movement with MAA dur-
ing maximum voluntary effort.
Jaw movement mm
Right-left direction Shift to the right
Shift to the left 11.9 +/– 1.99
11.4 +/– 1.82
Antero-posterior
direction Maximum jaw opening
Lateral jaw movement 1.63 +/– 0.95
0.77 +/– 0.25
(N = 5)
3. CASE REPORT
A 38-year-old male with a chief complaint of sleep frag-
mentation from OSA was referred to our clinic from a
cardiac physician. The patient’s weight, height and BMI
were 73 kg, 171 cm and 25 kg/m2, respectively.
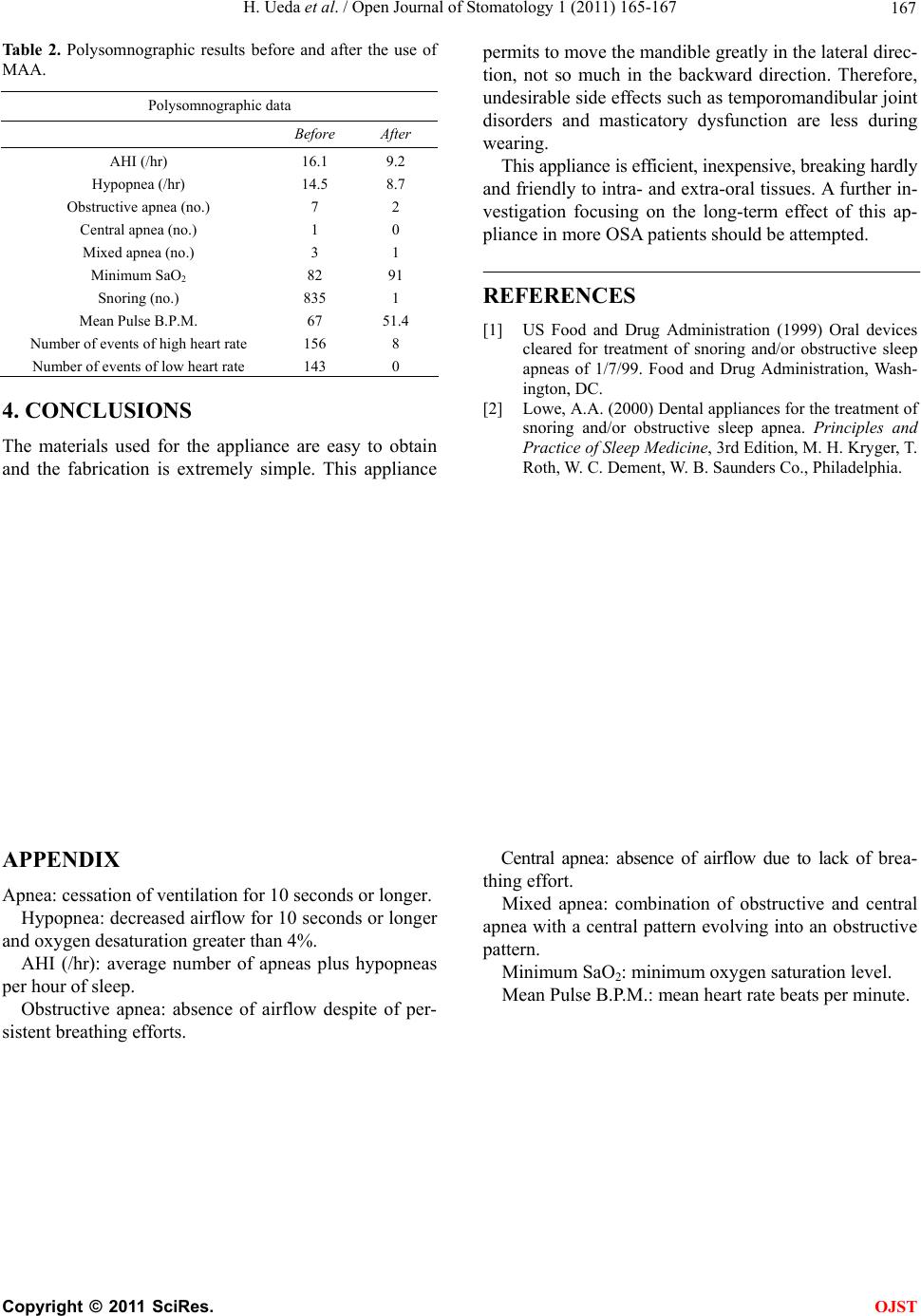
The molar relationship on both sides was Angle’s
Class I, and mild crowding was found in the upper and
lower anterior teeth (Figure 3). Periodontal problems
and tem po romandibular joi nt disorders were not found.
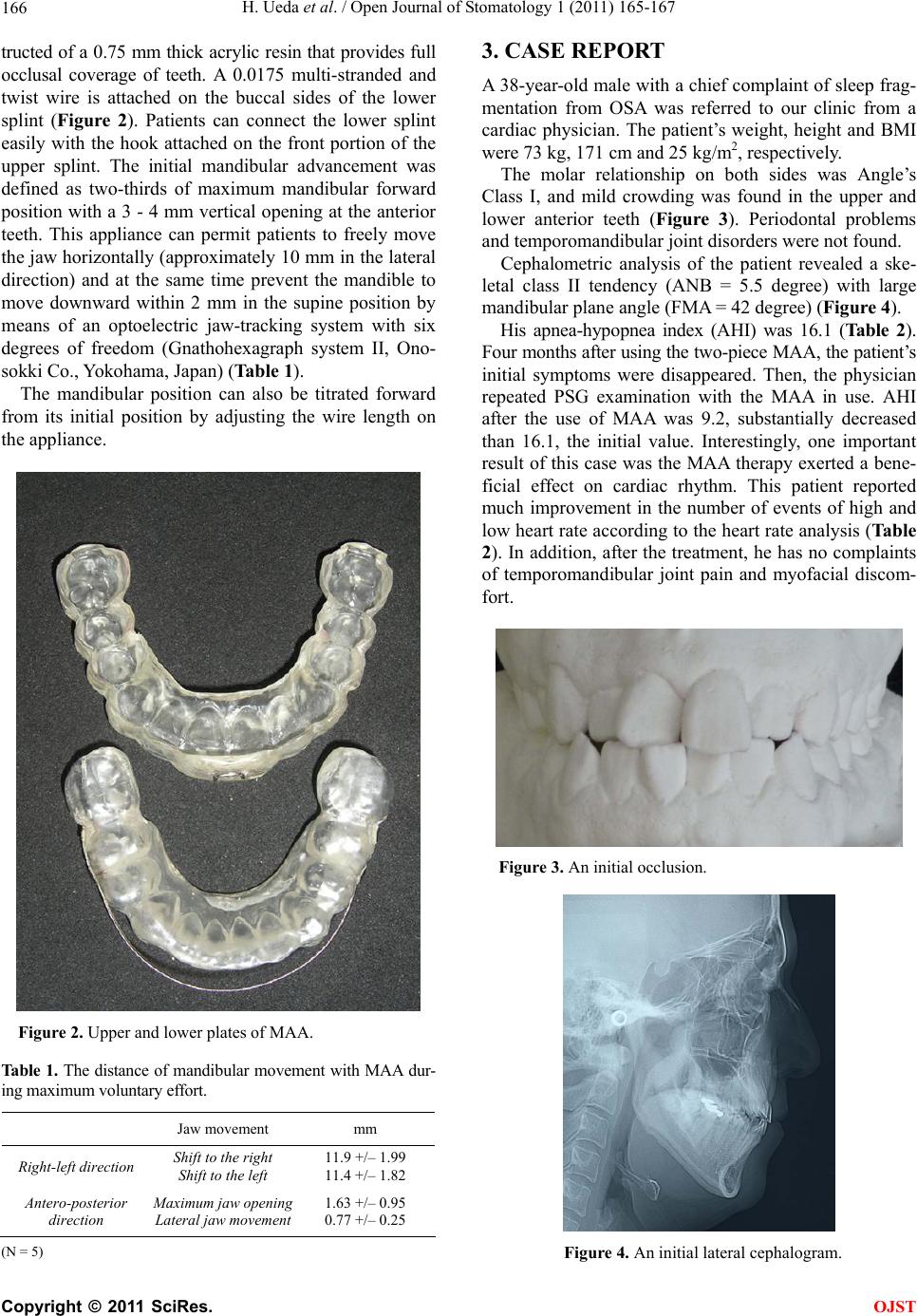
Cephalometric analysis of the patient revealed a ske-
letal class II tendency (ANB = 5.5 degree) with large
mandibular pl ane angle (FMA = 42 degree) (Figure 4).
His apnea-hypopnea index (AHI) was 16.1 (Table 2).
Four months after using the two-piece MAA, the patient’s
initial symptoms were disappeared. Then, the physician
repeated PSG examination with the MAA in use. AHI
after the use of MAA was 9.2, substantially decreased
than 16.1, the initial value. Interestingly, one important
result of this case was the MAA therapy exerted a bene-
ficial effect on cardiac rhythm. This patient reported
much improvement in the number of events of high and
low heart rate according to the heart rate analysis (Table
2). In addition, after the treatment, he has no complaints
of temporomandibular joint pain and myofacial discom-
fort.
Figure 3. An initial occlusion.
Figure 4. An initial lateral cephalogram.
C
opyright © 2011 SciRes. OJST