Health
Vol.5 No.4(2013), Article ID:29885,8 pages DOI:10.4236/health.2013.54095
Socio-demographic and health-related determinants of metabolic syndrome (MetS) among male Kuwaiti adolescents aged 10 - 19 years*
![]()
1Department of Community Medicine and Behavioural Sciences, Faculty of Medicine, Kuwait University, Kuwait; #Corresponding Author: alisa@hsc.edu.kw
2Department of Pathology, Faculty of Medicine, Kuwait University, Kuwait
Copyright © 2013 Abdulwahab N. Al-Isa, Abayomi O. Akanji. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received 20 November 2012; revised 30 December 2012; accepted 30 March 2013
Keywords: Metabolic Syndrome; Kuwaiti; Arabs; Adolescents; Obesity
ABSTRACT
Background and Aims: The aim of this study was to explore the association between socio-demographic and health-related factors and metabolic syndrome (MetS) among male adolescents in Kuwait. Methods and Results: We used a cross sectional study with a sample of 303 male Kuwaiti adolescents of age 10 - 19 years, selected from intermediate and high schools. All had anthropometric measurements and biochemical tests. In addition, a questionnaire for the evaluation of the association of a variety of socio-demographic and health-related factors with MetS was given to participants for assessing these factors. The presence of the MetS was assessed in each subject using two validated criteria proposed by the National Cholesterol Education Program-Third Adult Treatment Panel Modified for age (NCEP-ATP III) and the International Diabetes Federation (IDF). We established that the prevalence of MetS by the ATP III and IDF criteria was respectively 9.8% and 11.7%. The educational level of both parents and factors such as weight, diet and physical activity associated significantly with the presence of MetS in Kuwaiti adolescents. Conclusions: The IDF gave higher values for the prevalence of MetS than the ATP III. Using either criterion, this information obtained in this study is important in planning strategies for prevention and control of this disorder.
1. INTRODUCTION
The prevalence of metabolic syndrome (MetS) is expected to be high as overweight (BMI > 25 kg/m2) and obesity (BMI > 30 kg/m2) are high in Kuwait [1,2]. In recent years, the prevalence of obesity in developing countries has tripled and along with MetS also increased [3,4]. Other studies have also shown a high prevalence of MetS in developing countries among the young, which may lead to morbid conditions, chief among which are cardiovascular diseases, especially later on in life [5,6].
However, defining MetS among children and adolescents is not a straight-forward matter. The criteria used to quantify the MetS were shown in an earlier publication by the authors [7]. Studies which explore the association of socio-demographic and health-related factors are few among adults [8-11] and those which explore the same among adolescents are, at present, scarce [12,13]. The second study, Aboul Ella, is the only Arab study found in the literature that address the prevalence of MetS and insulin resistance among Egyptian adolescents 10 - 18 years of age and include socio-demographic and healthrelated factors associated with MetS. The authors reported earlier on the prevalence of MetS among female Kuwaiti adolescents [7]. In this study, the authors have attempted to quantify the prevalence of MetS among male Kuwaiti adolescents of similar age group, using the IDF and ATP III criteria, and in addition assess in details the potential influence of a variety of common sociodemographic and health-related factors on the likely high prevalence of MetS in this population. It should be noted, however, that this is the first study of its kind done on Kuwaiti male adolescents and which included the largest yet number of socio-demographic and healthrelated factors in an attempt to explore their association with MetS.
2. SUBJECTS & METHODS
This has been described in detail earlier but it is presented here with some modification [7].
2.1. Sampling
A multi-stage sampling procedure was followed. There are six governorates in Kuwait, each with a set of school levels from kindergarten to secondary. A list of the schools was obtained from the Ministry of Education. Two of the six governorates were randomly selected for the study, the Capital and Hawally governorates. From each of the two governorates, one intermediate and one secondary school were randomly selected. Every student was invited to participate, in anticipation of a low participation rate. Ethical approval for the study was obtained from the Ethics Committee of the Faculty of Medicine, Kuwait University. The subjects were recruited after written informed consent from both the student and his parent/guardian.
The exclusion criteria were diabetes mellitus, hypertension, other chronic systemic illness requiring longterm medication, and limb fractures (with cast that may make anthropometry difficult).
2.2. Questionnaires Measurement and Blood Sample
2.2.1. Questionnaire
Socio-demographic and health-related information were obtained through a questionnaire, administered with the assistance of one of the project personnel. The specific parameters evaluated were:
• age: 10 - 19 years;
• family structure: number of brothers, sisters, and total number of siblings: none (0), low (1 - 3), medium (4 - 7) and high (> or 8);
• birth order: first, middle, last;
• parental education categorized as: low (illiterate or elementary), medium (intermediate or secondary), high (college or higher);
• parental occupation: working, not working;
• type of housing: private rental, government subsidized, owner-occupier;
• number of rooms in residence: low (1 - 2), medium (3 - 4), high (≥ or 5);
• number of residents in house: low (1 - 2), medium (3 - 5), high (≥ or 6);
• number of domestic servants: none, low (1 - 2), medium (3 - 5), high (≥ or 6);
• family income/month: low (<$1500), medium ($1500 - $3000), high (>$3000);
• relationship between parents: first cousins, related, not related;
• preferred travel: west, east, both, neither;
• number of major meals eaten: 1, 2, 3;
• eating between meals: yes, no, sometimes;
• physical exercise: yes, no;
• participation in sports (hours/week): none, low (≤ or 2), medium (3 - 4), high (≥ or 5);
• participation in sports (months/yr): <1 month, 1 - 3, ≥ or 4;
• last dental or physical check-up: do not remember, >2 yr ago, 1 yr ago, 1 month ago;
• number of times on supervised diet: none, low (1 - 2), medium (3 - 4), high (≥ or 5);
• dieting practice: self, via specialist, relatives/friends, mass media, none;
• self-assessed nutritional knowledge: weak, good, excellent;
• need for special diet: yes, no, do not know.
2.2.2. Anthropometric Measurements
Waist circumference (WC) was measured midway between the inferior costal margin of the ribs and the iliac crest. Weight and height were measured with the subject in light clothing while standing against a wall. These measurements were taken by the same person to avoid inter-observer variability. The body mass index (BMI) was, thereafter, calculated as weight (kg) divided by height2 (m2). We used age-specific BMI cut-off points for overweight and obesity, as previously described [7].
2.2.3. Biochemical Analyses
Fasting blood sample was collected from each participant in the morning after a 10hr overnight fast. The specimens were kept cool in an ice box until separation of blood from plasma or serum; the latter were frozen at −80˚C prior to biochemical analysis. Serum was subsequently analyzed for biochemical liver and kidney function parameters and blood lipids (total cholesterol (TC), triglycerides (TG), and HDL by routine Auto-Analyzer techniques (Beckman-Coulter DxC, Fullerton, CA, USA) at the Clinical Biochemistry Laboratory of the Faculty of Medicine with robust QC procedures. The levels of LDL were calculated using the Friedewald equation in all cases with TG < 4.50 mmol/L.
2.3. The Criteria for Diagnosing Metabolic Syndrome (MetS)
The presence of MetS was diagnosed using two commonly used criteria—IDF and NCEP ATP III-, modified for age. There are no criteria currently recommended for Arab population. We have used these criteria in defining MetS in a previous publication [7].
3. STATISTICAL ANALYSIS
Version 17 of the Statistical Package for Social Sciences software (SPSS, Inc., Chicago, USA) was used for data entry and analysis. Descriptive statistics were used which included mean, standard deviation and proportions. Moreover, sensitivity and specificity measures of the two MetS criteria were used and were presented in an earlier publication [7]. In addition, logistic regression analysis was performed on the socio-demographic and health-related factors that were obtained through a questionnaire to find possible association between MetS and these factors. The level of significance was set to be p < 0.05. This was done after adjustment for age, BMI, and both.
4. RESULTS
The mean (SD) age of the subjects was 14.2 ± 2.2 yrs. Table 1 indicates the mean (SD) for WC, and the different biochemical and clinical parameters considered as components of the MetS by either of the criterion. The MetS prevalence rate was 9.8% by the IDF criterion, and slightly higher (11.7%) by the ATP III criterion. It is of interest that the higher prevalence value seen with the latter diagnostic group was obviously attributable to the higher percentages of subjects with increased WC, glucose and BP. Incidentally, hypertriglyceridemia was more commonly recognized with the IDF criterion, not surprisingly because of the lower cut-off point. The sensitivity and specificity of both the modified IDF and ATP III diagnostic criteria of MetS were presented in an earlier publication [7].
Table 2 indicates the expected differences in mean values for the various diagnostic parameters for those individuals with and without MetS, determined according to the IDF and ATP III criteria. It is clear that, while systolic BP differed in the subjects with or without MetS, diastolic BP did not appear to be influenced by the presence of MetS.
Table 3 indicates the age-adjusted odds ratios for the putative socio-demographic and health-related factors’ associations with MetS in the subjects. The results suggested that parental education (particularly paternal), being on some form of supervised dietary control (currently or previously), including the mode of access to that control as well as chronic, persistent and constant physical activity including participation in sports were the important associations of MetS diagnosed essentially by either criteria, although seen more robustly with the IDF criterion. It was of interest that maternal level of education and a family history of obesity (as indicated
Table 1. Relative prevalence of metabolic syndrome (MetS) and its diagnostic parameters in Kuwaiti male adolescents aged 10 - 19 years.
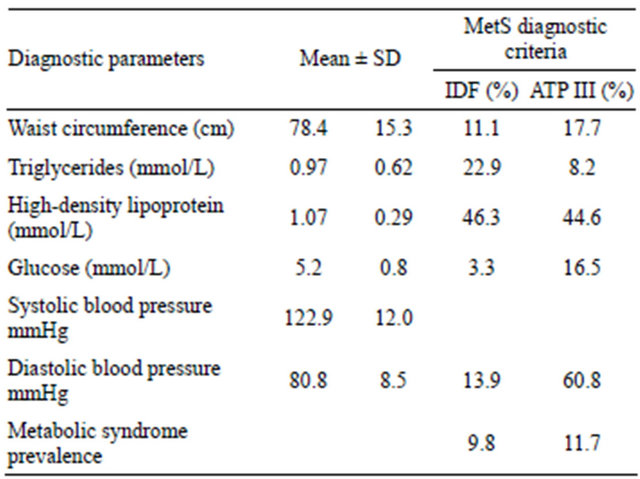
Table 2. Differences in mean values for diagnostic parameters in Kuwaiti male adolescents aged 10 - 19 years with and without metabolic syndrome, according to the IDF and ATP III criteria (p-values represent between group differences for each diagnostic group).
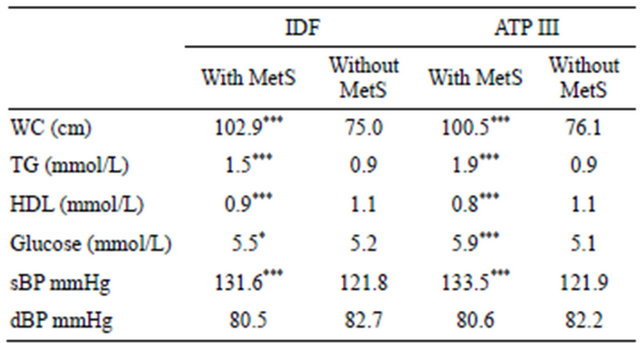
Abbreviations: WC, waist circumference; TG, triglycerides; HDL, highdensity lipoprotein; sBP, systolic blood pressure; dBP, diastolic blood pressure; MetS, metabolic syndrome. The column for IDF (%) and ATP III (%) indicate the relative prevalence of the different diagnostic parameters in the subjects, ***p < 0.001.
by numbers of obese first degree relatives) did not appear to influence liability to MetS. Obesity was an expected determinant, by definition and the logistic regression analyses was, therefore, repeated with adjustment of the calculated ORs for BMI.
Table 4 indicates the BMI-adjusted odds ratios for putative socio-demographic and health-related associations with MetS in the subjects. The results suggested that age, governorate (Hawally), father’s education, family monthly income, number of sisters and GPA were the important socio-demographic associations with MetS seen with IDF criterion. Health-related factors that showed similar association with MetS included obese relatives, practicing sports, weekly and monthly physical activity, being on a diet, health status, number of times dieting, diet consultation and last dental check-up. The
Table 3. Logistic regression analysis with determination of age-adjusted odds ratios (and 95% CI) for the putative anthropometric, socio-demographic and health-related determinants of metabolic syndrome in the subjects, according to the IDF and ATP III diagnostic criteria.
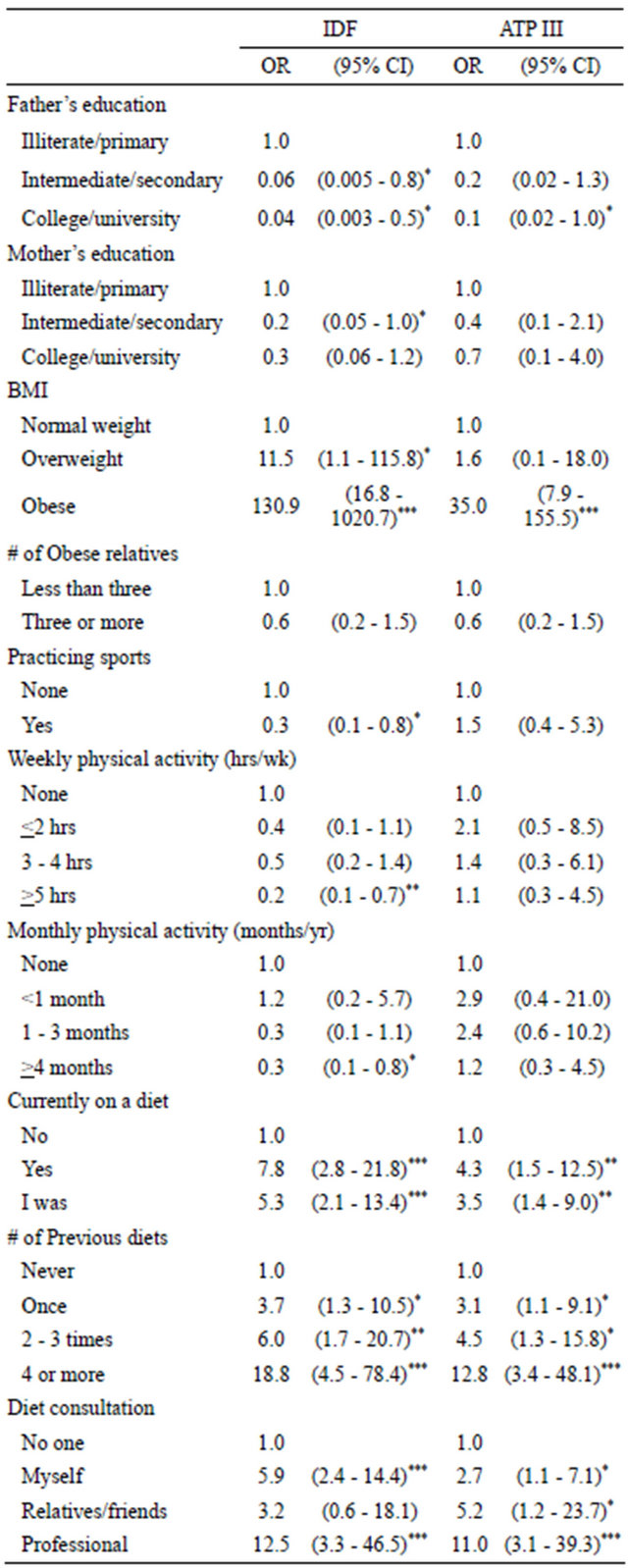
*p < 0.05, **p < 0.01, ***p < 0.001.
associations of socio-demographic and health-related factors with MetS, using ATP III criterion were less robust. It included, among the socio-demographic factors age, governorate, father’s education and number of persons living at home. The association of health-related factors with MetS included being on diet, number of times dieting, and diet consultations.
Table 5 indicates the ageand BMI-adjusted odds ratios for the putative socio-demographic and health-related associations with MetS in the subjects. The results suggested that governorate, persons living at home and GPA showed significant association with MetS using the IDF criterion. However, health-related factors that showed significant association with MetS included all those related to physical activity, number of times dieting and health status, using the IDF criterion. However, the ATP III showed less robust socio-demographic and healthrelated association with MetS. It included one sociodemographic, (number of people living at home) and one health-related factor (number of times dieting). Therefore, it is obvious from these results that the IDF was more robust in presenting significant associations with MetS after adjustment of the calculated ORs for age, BMI and age and BMI.
5. DISCUSSION
The higher value of ATP III (11.7%) for MetS is perhaps related to the stark differences obtained for Glucose and BP (Table 1). There were slight differences between means MetS (Table 2). In fact the values were almost identical. It was noted in this study that adolescents whose father had intermediate or college education were at risk of having MetS, using the IDF criterion. But with the ATP III criterion, only those whose father had a college education were at risk of having MetS. Those whose mother had an intermediate education were at risk of having MetS using the IDF criterion. No explanation can be found for these findings. For health-related factors, those who are overweight and obese were more at risk of MetS using the IDF criterion as opposed to those who were obese using the ATP III criterion. Those currently on a diet were at risk of having MetS using both criteria. The same was true for those who had a number of previous diets. Those on diet consultation were at risk of MetS except for those doing it on their own. Those practicing sport were at risk of MetS using the IDF criterion. The same was true for those who practiced sports >5 a week and >4 months a year.
The topic addressing socio-demographic and healthrelated factors associated with MetS is scarce among adults and even more so among adolescents. No study, whether among adults or adolescents have included as many socio-demographic and health-related factors as this study. A Korean study on adults using the ATP III
Table 4. Logistic regression analysis with determination of BMI-adjusted odds ratios (and 95% CI) for the putative anthropometric, socio-demographic and health-related determinants of metabolic syndrome in Kuwaiti male adolescents, according to the IDF and ATP III diagnostic criteria.
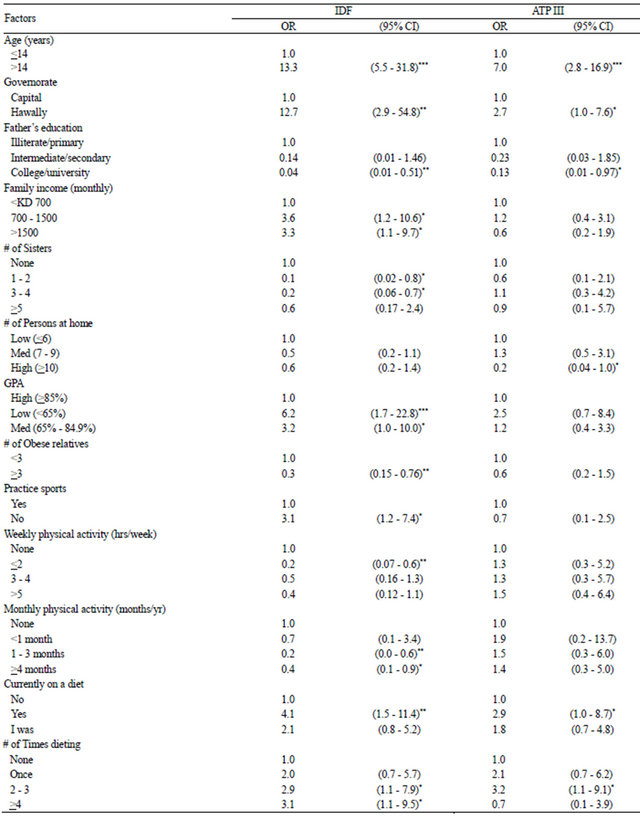
Continued
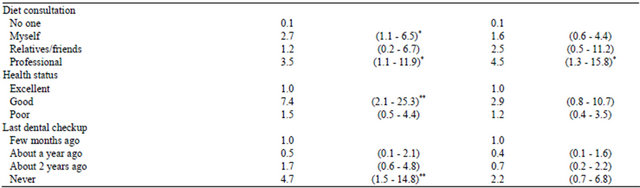
*p < 0.05, **p < 0.01, ***p < 0.001.
Table 5. Logistic regression analysis with determination of age and BMI-adjusted odds ratios (and 95% CI) for the putative anthropometric, socio-demographic and health-related determinants of metabolic syndrome in Kuwaiti male adolescents, according to the IDF and ATP III diagnostic criteria.
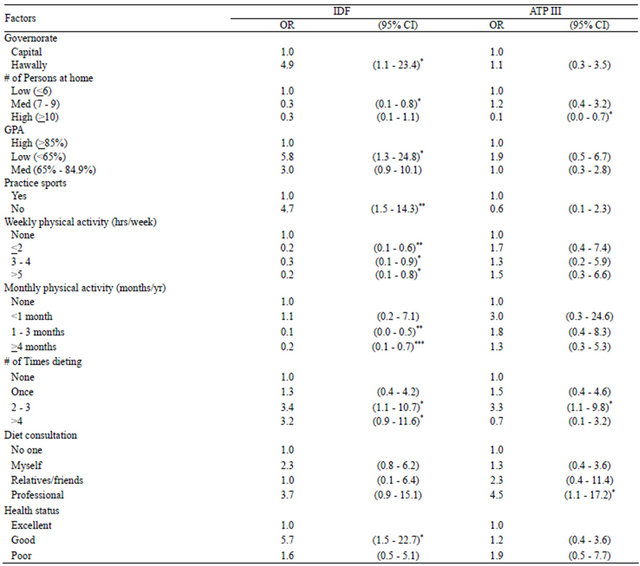
*p < 0.05, **p < 0.01, ***p < 0.001.
criterion found MetS to be 14.2% for men and 17.7% for women. Age, not working, and elevated BMI were associated with MetS in both genders. A moderate physical activity session (2 - 3 sessions per week) in men reduced the odds of MetS [9]. Another study which focused on the social class and MetS found the two associated on the basis of behavioural factors [10]. A study on a Mediterranean population addressed the association of sociodemographic risk factors associated with MetS, using the same criteria used in this study. The findings of the study were that in addition, to age, gender, level of adiposity the socio-demographic risk factors that were independently associated with MetS were physical activity and social class [8]. The association of socio-economic status (SES) with MetS in one study included gender, females of lower class, as reflected by education and occupation were more at risk of MetS. This was not true for men [11]. A study on the influencing factors on MetS among Iranian adolescent girls showed that SES and medical history of parents can influence the prevalence of MetS [12]. The best yet study which came the closest to the present study was done in Egypt on Egyptian adolescents 10 - 18 years of age. Its main focus in the title was on insulin resistance. Nevertheless, while using the ATP III criterion, the study found that the prevalence of MetS was 7.4%. The health-related factors that were significantly associated with MetS were family history of obesity and physical inactivity [13].
The reviewed studies suggested several conclusions, foremost among which is the risk of obesity on MetS. This is, of course, related to the level of physical activity. Social class and social inequalities play a part on the prevalence of MetS. SES showed an association with MetS which may be reflected by education, occupation and income. Adverse effect on certain factors, if not all addressed here, may have an influence on increasing the risk of cardiovascular disease, especially with a lifestyle that included increase in obesity and sedentary lifestyle. Understanding and being aware of factors that influence the prevalence of MetS are useful for determining public health strategies that control the MetS Epidemic, especially in developing and Arab countries. The few sociodemographic and health-related factors that were found to be associated with MetS suggest that in addressing the problem of MetS, researchers should look beyond the anthropometric and biochemical parameters for its diagnosis.
A possible bias in the results may be related to the low rate, because of the invasive nature of the study, of parental and/or students consent to take part in the study despite the fact that consent forms were given to all students. It is possible that those who gave consent have more health awareness and knowledge about the value of the procedure, if not for now but may be for the future. It will allow them to take the necessary precautions to avoid being at risk of some morbid conditions associated with MetS. On the other hand, the high refusal rate may vary with different strata of the population and whether or not the rich or the more educated had higher participation rate or a combination of the whole strata, including the poor or less educated, makes it difficult to be certain that such bias would have affected our results. Furthermore, it is not certain that male Kuwaiti students could always have followed the requirements of coming to school fasting for the previous ten hours and, therefore, carrying out blood tests may not come with ease.
6. ACKNOWLEDGEMENTS
The authors are grateful to Kuwait University Research Administration and Kuwait Foundation for the Advancement of Sciences for funding this study (MC 01/04). We are also grateful to the Ministry of Education, to all participating adolescents and their parents; and for the directors of selected schools for facilitating data collection. A special acknowledgment goes to Miss Shorooq Al Saji, especially with data analysis.
REFERENCES
- Al-Isa, A.N. (2003) Are Kuwaitis getting fatter? Nutrition and Health, 17, 185-197. doi:10.1177/026010600301700301
- Al-Isa, A.N. (2004) Body mass index, overweight and obesity among Kuwaiti intermediate school adolescents aged 10 - 14 years. European Journal of Clinical Nutrition, 58, 1273-1277. doi:10.1038/sj.ejcn.1601961
- Kelishadi, R. (2007) Childhood overweight, obesity and the metabolic syndrome in developing countries. Epidemiologic Reviews, 29, 62-76. doi:10.1093/epirev/mxm003
- Hossain, P., Kawar, B. and El Nahas, M. (2007) Obesity and diabetes in the developing world—A growing challenge. The New England Journal of Medicine, 356, 213- 215. doi:10.1056/NEJMp068177
- Franks, P.W., Hanson, R.I. and Knowler, W.C. (2007) Childhood predictors of young onset type 2 diabetes mellitus. Diabetes, 56, 2964-2972. doi:10.2337/db06-1639
- Morrison, J.A., Friedman, L.A. and Gray-McGuire, C. (2007) Metabolic syndrome in childhood predicts adult cardiovascular disease 25 years later: The Princeton lipid research clinics follow-ups study. Pediatrics, 120, 340- 345. doi:10.1542/peds.2006-1699
- Al-Isa, A.N., Akanji, A.O. and Thalib, L. (2010) Prevalence of the metabolic syndrome among female Kuwaiti adolescents, using two different criteria. British Journal of Nutrition, 103, 77-81. doi:10.1017/S0007114509991425
- Buckland, G., Salas-Salvado, J., Roure, E., Bullo, M. and Serra-Majem, L. (2008) Sociodemographic risk factors associated with metabolic syndrome in a Mediterranean population. Public Health Nutrition, 11, 1372-1378. doi:10.1017/S1368980008003492
- Park, H.S., Oh, S.W., Cho, S.-II, Choi, W.H. and Kim, Y.S. (2004) The metabolic syndrome and associated lifestyle factors among South Korean adults. International Journal of Epidemiology, 33, 328-336. doi:10.1093/ije/dyh032
- Ramsay, S.E., Whincup, P.H., Morris, R., Lennon, L. and Wannamethee, S.G. (2008) Is socioeconomic position related to the prevalence of metabolic syndrome? Influence of social class across the life course in a population-based study of older men. Diabetes Care, 1, 1-16.
- Santos, A.C., Ebrahim, S. and Barros, H. (2008) Gender, socio-economic status and metabolic syndrome in middle-aged and old adults. BMC Public Health, 8, 62-71. doi:10.1186/1471-2458-8-62
- Mirhossini, N.Z., Yusoff, N.A.M., Shahar, S., Parizadeh, S.M.R., Mobarhen, M.G. and Shahkery, M.T. (2009) Prevalence of the metabolic syndrome and its influencing factors among adolescent girls in Mashhad, Iran. Asia Pacific Journal of Clinical Nutrition, 18, 131-136.
- Aboul Ella, N.A., Shehab, D.I., Ismail, M.A. and Maksoud, A.A. (2010) Prevalence of metabolic and insulin resistance among Egyptian adolescents 10 - 18 years of age. Journal of Clinical Lipidology, 4, 185-195. doi:10.1016/j.jacl.2010.03.007
NOTES
*Funding: Kuwait University Research Administration (KURA) and Kuwait Foundation for the Advancement of Sciences (KFAS), Grant #MC01/04.
Conflict of interest: None declared.