Open Journal of Preventive Medicine
Vol. 2 No. 4 (2012) , Article ID: 25028 , 9 pages DOI:10.4236/ojpm.2012.24068
Certainty of patient survival with reference to game information dynamic model
![]()
1School of Information Science, Japan Advanced Institute of Science and Technology, Nomi, Japan; *Corresponding Author: takeo-n@jaist.ac.jp
Received 18 July 2012; revised 10 September 2012; accepted 6 October 2012
Keywords: Certainty of Patient Survival; Game Information Dynamic Model; Naturopathic Therapy; Herbal Treatment; Natural Antioxidants; Hepato-Cellular Carcinoma
ABSTRACT
This paper is concerned with Hepato-Cellular Carcinoma (HCC) patients treated naturopathic agents. Patients treated with ≥4 agents survived significantly longer than patients treated with ≤3 agents. The great effect is seen in patients treated with at least 4 agents that include Cordyceps sinensis. This greater certainty of patient survival without toxic side effects is significant benefit comparing with the conventional therapy. Treatment of HCC with a regimen of ≥4 agents prepared from natural products is associated with greater certainty of patient survival in a substantial portion of patients. The information dynamic model for certainty of patient survival is derived based on fluid mechanics, where a series of approximate solutions of the flow between two parallel flat walls, one of which is at rest, the other is suddenly accelerated from the rest to a constant velocity are used. The kinetic energy of certainty of patient survival decreases with increasing time, while the potential energy increases with increasing time. Total mechanical energy of patients treated with 4 or more agents is smaller than that treated with 3 or fewer agents. The kinetic energy (potential energy) of patients treated with 4 or more agents decreases (increases) more slower than the kinetic energy (potential energy) of patients treated with 3 or fewer agents.
1. INTRODUCTION
Hepato-Cellular Carcinoma (HCC) is the 3rd most frequent cause of cancer death globally and in Japan, where the age-adjusted death rate from HCC is approximately 23 per 100,000 per year. Surgical resection, liver transplantation, and radiofrequency ablation are considered to be potentially curative treatments for HCC. However, only a minority of patients is eligible for surgery or transplantation at the time of diagnosis, and the rate of eventual relapse with all of these therapies is high. The other treatments, including percutaneous ethanol injecttion therapy, transarterial chemoembolization, chemotherapy, and most recently, therapy with kinase inhibitors, are not curative but can prolong survival. Non the less, for patients with advanced liver disease and inoperable tumors, the prognosis for long-term survival with HCC is quite poor.
The use of naturally occuring botanical and microbial products, one of the principals of naturopathic medicine, is another category of treatment to be considered in patients with end stage malignancy for which is there is no curative treatment. This paper is concerned with Retrospective analysis of case series of Hepato-Cellular Carcinoma (HCC) patients treated naturopathic agents [1]. It is found that there is a significant correlation between number of agents administered and survival (p < 0.0001). Patients treated with ≥4 agents survived significantly longer than patients treated with ≤3 agents (40.2 months vs. 6.4 months, p < 0.00001). This difference could not be attributed to statistically significant differences in severity of liver disease or tumor stage, delay in treatment, previous treatment, concurrent nondrug treatment, or censoring effects. The great effect is seen in patients treated with at least 4 agents that include Cordyceps sinensis. This greater certainty of patient survival without toxic side effects is significant benefit comparing with the conventional therapy. It is concluded that treatment of HCC with a regimen of ≥4 agents prepared from natural products is associated with greater certainty of patient survival in a substantial portion of patients. Principles of naruropathic medicine, is another category of treatment to be considered in patients with end stage malignancy for which there is no curative treatment. However, for clinicians who seek to practice evidence-based medicine, this form of therapy poses significant difficulties and limitations. These include lack of standardization of different preparations, lack of data regarding mechanism of action, and a paucity of controlled trials. Although randomized controlled studies that meet conventional standards have been reported for a variety of herbal products in the treatment of several diseases other than malignnancy, herbal treatments for cancer have rarely been subjected to this degree of scrutiny.
For over 20 years, we have designed and applied treatments based on natural substances to a variety of conditions, including malignancies. We have found that patients with HCC in particular seem to benefit from this therapy. In a number of cases the tumor is found to decrease in size, the tumor maker levels decrease substantially, and the patient survives comfortably for more than 5 years.
Main purpose of the present paper is to summarize our results in applying the naturopathic therapy to HCC. It has been shown that there is a strong correlation between survival and the number of preparations administered, thereby providing evidence for efficacy.
2. EXPERIMENT
2.1. Patients
We begin administering naturopathic treatment to patients with HCC in 1998. Records are available for review for 153 patients. The records for some patients seen 1998 and 2002 have been lost, but all available records are included, including records of all patients seen since 2002. Fifty-two patients are examined once and either do not qualify for treatment or do not return. Eight of these are known to have died a median of 22 days after presentation, while the fate of the others is unknown.
2.2. Consent
All treatment protocols are approved by the ethical review board of our hospital, which includes physicians, nurses, and phamacists. Upon their initial visit to the hospital or clinics, patients and their families are given an hour and half orientation to our approach to treatment. This includes mention of the likelihood that the case will be included in a presentation or publication. Those who agree to treatment are accepted as patients. For inpatients, written consent both for treatment and for inclusion in presentations or manuscripts is obtained on admission. For outpatients, written consent for inclusion in presentations or manuscripts is obtained upon initial preparation of the preparation or manuscript. Upon completion of the manuscript, oral confirmation of consent is obtained from surviving patients who can be contacted. Inclusion of patients in the manuscript is also reviewed and approved by the ethical review board.
2.3. Diagnosis of HCC
This analysis describes 101 patients who are given naturopathic treatment. The diagnosis of HCC is based primarily on characteristic dynamic CT imaging, with serum levels of α-fetoprotein and/or prothrombin induced by vitamin K absence or antagonist II providing supportive evidence [2]. In cases that have previously undergone surgical resection, the diagnosis is confirmed by histopathology. Patients who have undergone resection are excluded unless the tumor has recurred after resection and is no longer operable. Included are patients who have undergone percutaneous ethanol injection therapy, trans-catheter arterial chemoembolization, radiofrequency ablation, and/or chemotherapy. Patients are not prevented from continuing these therapies after beginning naturopathic therapy.
Staging: Tumor staging at the time of treatment initiation is performed according to the Balcelona Clinic iver Cancer (BCLC) [3]. Liver disease is assessed at the time of initiation of naturopathic treatment by a modification of the Child-Pugu classification (Llovet et al. 2008), in which the platelet count is substituted for the prothrombin time (platelet count ≥ 100,000 = 1 point, <100,000 and ≥50,000 = 2 points, <50,000 = 3 points). Because of this modification, and because performance staging is not done, the actual BCLC classification used is a modification.
Treatment: Patients are treated with combinations of the natural agents, to be listed. Blood cell counts, measures of hepatic and renal function, urinalysis, tumor markers, tumor size on imaging, and chest X-ray are monitored.
The survival data reported here is assessed from the time of initiation of naturopathic treatment. Patients lose to follow up are considered to have died one day after the last kept follow up visit, and thus the calculated certainty of patient survival figures are minimum estimates. Survival data are analyzed by Kaplan-Meier statistics, using Prism software.
2.4. Agents
The following naturopathic treatments are used, given as oral preparations.
1) Cirdyceps sinensis: This came from wildly grown, natural Cordyceps sinensis that is subjected to far infrared ray heating, brewing with Aspergillus oryzae and lipophilization with sesame oil, as described previously [4]. This process has been shown to activate antioxidant, tumoricidal, and other biological activities contained in natural products [4]. Cirdyceps sinensis is a parasitic fungus that infects insects, which has long been used in traditional Chinese medicine. The active ingredient in Cirdyceps sinensis, cordycepin, has been known since 1950 to be a purine nucleoside analog, 3’-deoxyadenosine and acts as an anti-metabolite of adenosine [5]. This compound is shown over 40 years ago to have anti-cancer activity in both human and rodent systems in vitro and in rodents in vivo [6]. The mode of action is thought to be related to the termination of nucleic acid synthesis [7]. Moreover, it has been shown that cordycepin experts a variety of pharmacologic effects in different tumor cell lines, and rodent systems including inhibition of polyadenylation, simulation of adenosine A3 receptors, and induction of apoptosis [6].
2) TT, OT, B-T: These are closely related Chinese natural products that are harvested and produced in Taiwan that have been widely used in traditional Chinese medicine for centuries. TT consists of extracts of Bezoar bovis, Kadinum, Rhei rhizome, Phellodendri cortex, Arecae semen, and Mori folium, OT consists of extracts of Bezoar bovis, Kadinum, Rhei rhizome, Hoelen, Arecae semen, Mori folium, and Crassocephalum crepidioides.
3) HTT: This is a modification of TT containing Harpago, a variety of pedaliaceae from the Kalahari Desert in Africa.
4) WBF: This is another traditional Chinese product containing extracts of Zizyphi fructus, Talcum crystallinum(Kadinum), Moutan cortex, Puerariae, Ginseng radix, Zingiberis rhizome, Rhei rhizome, Glycyrrhizae radix, Saposhnikvoviae radix, and Trichosanthis radix.
5) Natural anti-oxidants (NAO): This preparation is developed and is produced by the authors [8]. It is produced from wheat germ, rice bran, soybean, hato mugi, which is a type of oriental wheat, wheat, sesame, green leaf extracts from Japanese green tea and Yuzu oranges. The extracts are subjected to far infrared ray heating, brewing with Aspergillus oryzae (koji), and with lipophilization with sesame oil treated as described above for Cirdyceps sinensis.
6) UCR: This is derived from Guacatonga (Casearia sylvestris), a tropical plant grown in the clay soils of Amazon. It is taken as tea and is said to show anti-tumor activity [10]. It is also used to treat benign digestive disorders.
7) TIM: This is an extract of the bark of Tecomaipe Mart, a tree that grows throughout South and Central America. It contains naphthoquinones, furanonaphoquinones, and other compounds reported to have anti-cancer, anti-microbial, and anti-inflammatory properties [9].
8) BG103: This is beta-glucan extracted from the edible Agaricus blazei mushroom, reported to be effective in several types of malignancy. It shows in vivo immunomodulatory and anti-inflammatory anti-tumor effets [11]. Other extracts from this mushroom have been shown to have specific anti-tumor activity against heaptoma cells [12].
9) BWS: This is derived from the seeds of loquat, known to be rich in amygdalin, which has been claimed to have anti-cancer activity.
10) BG105: This is “Chaga”, an aqueous extract of an edible mushroom, Inonotus obliquus, that grows in northern Asian latitudes, e.g., in Siberia, Hokkaido, and Mongolia. It has been reported to inhibit the protease of HIV-1. Recent literature has extensively documented antioxidant, anti-tumor, and hypoglycemic activity [13].
11) Sandbath Treatment: The sandbath is produced from stones that emit far infrared radiation (4 - 14 μm). This treatment has been reported to inhibit the growth of tumor cells in mice [14]. The patients undergoing this treatment also have received intravenous multivitamin infusions.
12) Regimen: WBF is specifically applied for HCC, and other agents are generally given for the overall purpose of inhibiting tumor growth. Agents are added or substituted when there is evidence of tumor progression. In particular, Cirdyceps sinensis is generally used for signs of tumor progression.
13) Lifestyle Counseling: Patients are routinely counseled to get adequate sleep, and to avoid overwork, mental stress, and dietary fat.
3. DATA COLLECTION
Present data are picked up from the medical records. In addition to demographic data, routine laboratory data mentioned above, and all administered therapies. These are as follows; tumor imaging by CT, presence or absence of cirrhosis, underlying liver disease (e.g. hepatitis C virus, hepatitis B virus, alcoholism), presence and location of metatases, AFP, PIVKA II, previous outside treatments including surgery, outside treatments occurring during naturopathic therapy and dates of such treatments.
3.1. Experimental Results
3.1.1. Patient and Disease Characteristics
The data here are obtained from 101 patients who are started on treatment with the natural products described methods in the above, who have returned for follow up, and for whom records are available. Most of them have underlying cirrhosis (80%), and most of them have chronic infection with either hepatitis C virus (63%) or Hepatitis B virus (18%) or both (1%). Nine have metastatic disease.
Over a quarter (27%) has had no previous treatment. Of the remainder, 20% have had surgical resection of the primary tumor, with subsequent relapse. Other prior treatments consist of TACE (50%), RFA (28%), PEIT (15%), and chemotherapy (14%). 34% have undergone one of these treatment modalities, whereas 40% have undergone 2 or more. 38% of patients undergo one or more conventional forms of treatment concurrent with naturopathic treatment.
The median modified Childs-Pugh Score is 6, ranging from 3 to 13.
3.1.2. Treatment Regimens
Patients are treated with combinations of the natural products, as described in Methods. A total of 12 different agents are used. The six most commonly used are HTT, WBF, NAO, BG103, Cordyceps senensis, and BWS, which are given to 96, 95, 72, 39, 27, and 17 patients, respectively. The most common combination is that of HTT, WBF, and NAO, which is given to 66 patients, with or without NAO, with or without other agents. Patients have normally started on 2 or 3 agents (mean ± standard deviation of 2.6 ± 0.8), and other agents are added or substituted later if there is evidence of tumor progression. Patients attended clinic monthly or bimonthly until they will die, are lost to follow up, or are too debilitated to attend. Median time from beginning of treatment to death or last clinic visit is 13.4 months, ranging from 0.8 to 100.8 months, mean ± SEM25.7 ± 2.7 months.
3.1.3. Strong Correlation between Survival and Number of Agents Administered
Comparing the curves on certainty of patient survival for the 50 patients treated with ≥4 agents (4.7 ± 1.0, mean ± standard deviation)and the 51 patients treated with ≤3 agents (2.7 ± 0.5, mean ± standard deviation), there is a dramatic difference in median survival (40.2 vs. 6.4 months, respectively, p < 0.00001), as shown in Figure 1. There is no apparent difference between these two groups with respect to most of the characteristics. The
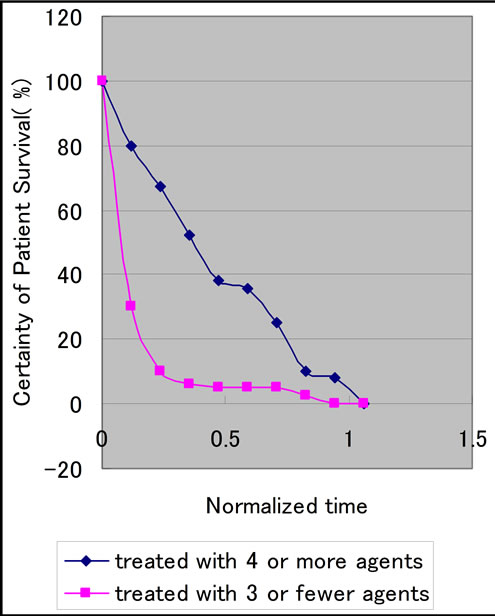
Figure 1. Certainty of patient survival (%) against normalized time t.
two exceptions are the median serum AFP level (50 vs. 24) and the median lag time to the onset of natural product therapy (7.6 vs. 2.0 months). The difference in the means of this time interval is not statistically significant.
3.1.4. Evidence That the Increased Survival in Patients Treated with ≥4 Agents Is Biologically
Although the correlation between the number of agents given and survival potentially suggests an effect of treatment, several potential artifacts need to be considered. It is possible that the correlation might simply reflect a censoring effect, i.e., the disproportionate addition of more than 3 agents to the regimen of patients who have already survived longer. It is also possible that the patients treated with ≤3 agents have more advanced disease at the outset. Another possibility is a difference in the use or response to conventional therapy.
Further examination of the data indicates that these possibilities are not major underlying factors. First of all, the difference in median survival, 34 months, is far grater than the 8 months median time lag between the start of treatment and the addition of the 4th agent. Second, in the group treated with ≥4 agents, there is no correlation between overall survival after onset of treatment and the interval between onset of treatment and addition of the 4th agent (r2 = 0.015, p = 0.397, i.e. not significantly different from 0).
In the 50 patients that received ≥4 agents, certainty of patient survival after the addition of the 4th agent is sig-

Figure 2. Certainty of patient survival (%) against normalized time. Blue curve is certainty of patient survival after start of 4th agent in 50 pts receiving ≥4 agents median survival = 13.7 months, while red curve is certainty of patient survival after start of 1st agent in 51 pts receiving ≤3 agents median survival = 6.4 months. p = 0.005.
nificantly greater than the overall survival of the group receiving ≤3 agents (13.5 vs. 6.4 months, p = 0.005) as shown in Figure 2. Moreover, certainty of patient survival after the addition of the 4th agent is biphasic, with approximately half the patients dying within 10 months. The median survival after addition of the 4th agent of the 24 patients that survive at least 10 months after addition of the 4th agent is 36.5 months, and their overall median survival is 67.5 months. This suggests that a subgroup of patients show a robust response to the addition of the 4th agent. The 26 patients that die within 10 months of addition of the 4th agent and 24 patients that survive more than 10 months do not differ significantly from each other in any of the parameters.
3.1.5. Possible Additional Benefit of Cordyceps sinensis
Among the natural product agents used, Cordyceps sinensis is given almost exclusively in the context of at least 4 agents. Overall, 27 patients received this agent, and 25 of them also received at least 3 other agents. There is a dramatically greater median survival in the patients given Cordyceps sinensis compared with all of the other treatment combination (42.7 vs. 15.7 months from the onset of therapy, p < 0.0001). Among the patients treated with ≥4 agents, people who receive Cordyceps sinensis have shown greater certainty of patient survival after addition of the 4th agent in Figure 2. Even when compared with the other patients receiving other regimens containing at least 4 agents, patients receiving Cordyceps sinensis and at least 3 other agents show significantly longer survival (55.7 vs. 32.5 months, p = 0.047).
4. INFORMATION DYNAMIC MODEL FOR CERTAINTY OF PATIENT SURVIVAL
The modeling procedure of information dynamics based on fluid mechanics has been established by Iida et al. [15]. An information dynamic model for a series of approximate solutions of the flow between two parallel flat walls, one of which is at rest, the other is suddenly accelerated from the rest to a constant velocity U0. Figure 3, will be constructed by following the procedure step by step.
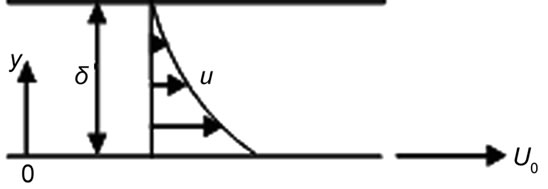
Figure 3. A definition sketch of flow between two parallel flat walls, one of which is at rest, the other is suddenly accelerated from the rest to a constant velocity U0.
4.1. Model
A similar flow near a flat plate which is suddenly accelerated from rest and moves in its own plane with a constant velocity is solved by Stokes [16]. For a brief sketch of the solution, see Schlichting [17].
For the present modeling, let us consider the flow between two parallel flat walls, one of which is at rest, the other is suddenly accelerated from the rest to a constant velocity U0 (Figure 1). Note that the walls are two-dimensional, horizontal and infinitely long.
Since the system under consideration has no preferred length in the horizontal direction, it is reasonable to suppose that the velocity profile are independent of the horizontal x-direction, which means that the velocity profile  for varying distance x can be made identical by selecting suitable scale factors for u and y. The scale factors for u and y appear quite naturally as the lower wall velocity U0 and gap length between the two walls δ. Hence, the velocity profile after the time t > 0 can be written as the function of f in the following way.
for varying distance x can be made identical by selecting suitable scale factors for u and y. The scale factors for u and y appear quite naturally as the lower wall velocity U0 and gap length between the two walls δ. Hence, the velocity profile after the time t > 0 can be written as the function of f in the following way.
 . (1)
. (1)
4.2. Solutions
The velocity profile is here accounted for by assuming that function f depends on  only, and contains no additional free parameter. Since the fluid particles are fixed on the surface of two walls due to the viscous effect, the function must take the value of 1 on the lower wall (y = 0) and the value of 0 on the upper wall (y = δ), The boundary conditions are:
only, and contains no additional free parameter. Since the fluid particles are fixed on the surface of two walls due to the viscous effect, the function must take the value of 1 on the lower wall (y = 0) and the value of 0 on the upper wall (y = δ), The boundary conditions are:

When writing down an approximate solution of the present flow, it is necessary to satisfy the above boundary conditions for u/U0. It is evident that the following velocity profiles satisfy all of the boundary conditions.
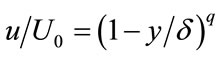 , (2)
, (2)
in the range , where q is positive real number parameter. Eq.2 is considered as the approximate solutions on the flow between two parallel flat walls, one of which is at rest, the other is suddenly accelerated from the rest to a constant velocity U0, where each solution takes a unique value of q. The value of q must be determined by the boundary conditions and the Reynolds number
, where q is positive real number parameter. Eq.2 is considered as the approximate solutions on the flow between two parallel flat walls, one of which is at rest, the other is suddenly accelerated from the rest to a constant velocity U0, where each solution takes a unique value of q. The value of q must be determined by the boundary conditions and the Reynolds number , where ν is the kinematic viscosity of the fluid.
, where ν is the kinematic viscosity of the fluid.
It is known that the transition from laminar to turbulent flow in the boundary layer is governed by the Reynolds number , where U∽ is the free stream velocity, d the boundary layer thickness. The critical Reynolds number Re crit, at which the transition is initiated, is of 2800 approximately [17,18].
, where U∽ is the free stream velocity, d the boundary layer thickness. The critical Reynolds number Re crit, at which the transition is initiated, is of 2800 approximately [17,18].
In case of the present flow, as shown in Figure 3, at 1 atmospheric pressure and temperature at 20˚C, water has the kinematic viscosity ν = 1.004 × 10−2 cm2/s. When water is chosen as the fluid, and the constant velocity U0 = 10 cm/s and the gap distance between the two walls δ = 10 cm are set, we obtain the Reynolds number Re 104. The result of this calculation clearly illustrates how the flow is liable to be turbulent under ordinary conditions.
104. The result of this calculation clearly illustrates how the flow is liable to be turbulent under ordinary conditions.
The solutions (2) are smooth analytical functions and thus they are only valid for laminar flow. For turbulent flow, no solution is known yet, but there is some hope to obtain it, by following Tsugé’s statistical theory of turbulence [19,20].
The fundamental governing equations for fluid mechanics are the Navier-Stokes equation [21,22]. This inherently nonlinear set of partial differential equations has no general solution, only severall exact solutions have been found [23]. All of these exact solutions are for laminar flows, and no turbulent flow solution is available yet. However, it is considered that each of the laminar solutions in (2) represents an approximate turbulent solution. In this regard, we consider that the solutions (2) are only applicable for laminar flow.
4.3. Applicability
Let us examine whether this solution is game information or not. The non-dimensional velocity  varies from 1 to 0 with increasing non-dimensional distance
varies from 1 to 0 with increasing non-dimensional distance  in many ways with changing the parameter q. It can be considered that
in many ways with changing the parameter q. It can be considered that  represents certainty of patient survival. This is why certainty of patient survival takes the value of 1 at start, and it decreases with increasing the time and becomes the value of 0 at her or his death.
represents certainty of patient survival. This is why certainty of patient survival takes the value of 1 at start, and it decreases with increasing the time and becomes the value of 0 at her or his death.
4.4. Parallelity of Physical and Informatical World
Imagine that the assumed flow is visualized with neutral buoyant particles. Motion of the visualized particles is detected by the eye almost instantaneously through light and is mapped on our retina [24], so that during these processes, motion of the “fluid particles” is transformed into that of the “information particles” by light carrying the images of fluid particles. This is why motion of the fluid particles is intact in the physical space, but only the reflected lights, or electromagnetic waves consisting of photons can reach the retina. Photons are then converted to electrochemical particles and are passed along the visual cortex for further processing in parts of the cerebral cortex [24]. Photons and/or electrochemical particles are considered to be information particles. It is, therefore, natural to expect that the flow in the physical world is faithfully transformed to that in the information world, or brain including eye, which is referred to “informatical world” here after. During this transformation, the flow solution in the physical world changes into the information in the informatical world.
4.5. Equivalencies
Proposed are correspondences between the flow in physical world and information in informatical world, which are listed in Table 1.
Considering the correspondences in Table 1, (2) can be rewritten as
 (3)
(3)
Introducing the following normalized variables in (4),
 and
and We finally obtain the analytical function of certainty of patient survival as
We finally obtain the analytical function of certainty of patient survival as
 , (4)
, (4)
where ξ is certainty of patient survival, η the normalized time and q the positive real number parameter.
Figure 4 illustrates how certainty of patient survival ξ due to (4) changes with increasing normalized time η.
5. DISCUSSION
5.1. Integration of Niwa’s Experiment in the Model
In this section, Niwa’s [1] 1st and 2nd experiments have been compared with the present information dynamic model expressed by (4).
Figure 5 shows a comparison of Niwa’s 1st experiment with the present model. It may be evident that the case treated with 4 or more agents fits with the model curve , while another case treated with 3 or fewer agents with
, while another case treated with 3 or fewer agents with . This shows how the former treatment contributes to make patient life time much longer.
. This shows how the former treatment contributes to make patient life time much longer.
Figure 6 shows a comparison of Niwa’s 2nd experiment with the present model. It may be evident that the

Table 1. Correspondences between flow and game information.

Figure 4. Certainty of patient survival ξ against normalized time η.
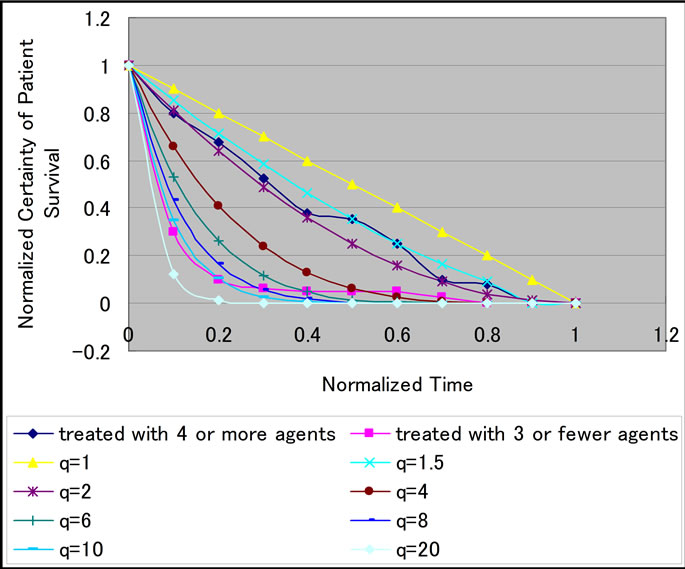
Figure 5. Normalized certainty of patient survival ξ against normalized time η. Comparison the 1st experiment with the present model.

Figure 6. Normalized certainty of patient survival ξ against normalized time η. Comparison the 2nd experiment with the present model.
case after start of 4th agent in 50% receiving greater than 4 agents fits with the model curve , while another case after start of 1st agent in 50% receiving smaller than 3 agents with
, while another case after start of 1st agent in 50% receiving smaller than 3 agents with . This shows how the former case contributes to make patient life time much longer.
. This shows how the former case contributes to make patient life time much longer.
5.2. Information Energy
In this section, the way how information energy depends on the time has been discussed.
Let consider the information mechanical energy and it is assumed to be conserved, thus we obtain the following relationship,
 , (5)
, (5)
where KE is the kinetic energy, PE the potential energy, and C the total mechanical energy. Eq.4 gives the explicit forms of KE and PE, respectively,
 (6)
(6)
where m is the normalize information mass. We here consider only when m = 1 without loss of generality. Physically, this case may correspond to that the information fluid in the informatical world is homogeneous.
When q = 2, the case treated with 4 or more agents,
 (7)
(7)
Substituting (7) in (5), we get
 (8)
(8)
With conditions at η = 1, KE = 2, PE = 0, at η = 1, KE = 0, PE = 2, (8) becomes
 (9)
(9)
Figure 7 illustrates KE expressed by (7) and PE expressed by (9), respectively.
Similarly to the above, when q = 10, we have
 (10)
(10)
and
 (11)
(11)
Figure 8 illustrates KE expressed by (10) and PE expressed by (11), respectively.
It is interesting to note the following to 3 points in Figures 7 and 8:
1) KE of certainty of patient survival decreases with increasing time, while the PE increases with increasing time;
2) Total mechanical energy of patients treated with 4 or more agents is smaller than that treated with 3 or fewer agents;
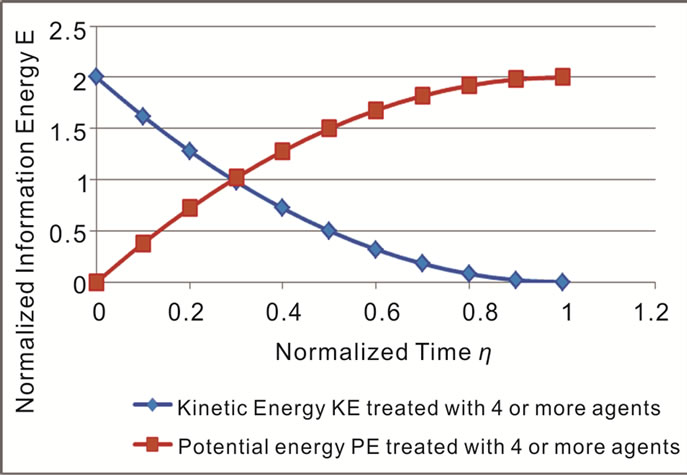
Figure 7. Normalized information energy E against normalized time η.
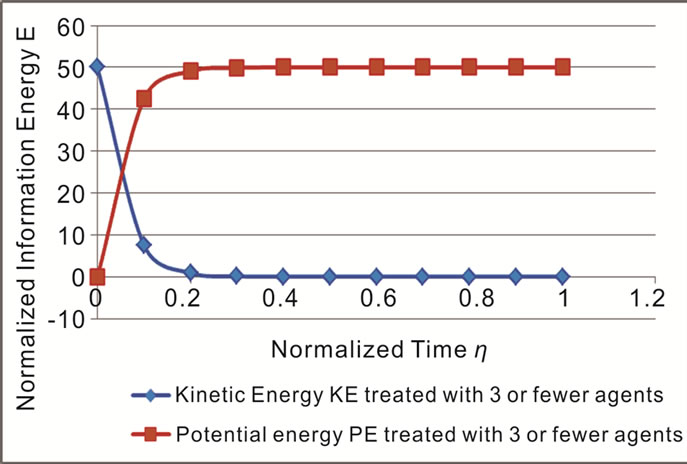
Figure 8. Normalized information energy E against normalized time η. Patients are treated with 3 or fewer agents.
3) KE (PE) of patients treated with 4 or more agents decreases (increases) more slower than KE (PE) of patients treated with 3 or fewer agents.
6. CONCLUSIONS
The new knowledge and insights obtained through the present study concerned with retrospective analysis of case series of Hepato-Cellular Carcinoma (HCC) patients treated naturopathic agents, have been summarized as follows;
1) There is a significant correlation between number of agents administered and survival (p < 0.0001); Patients treated with ≥4 agents survived significantly longer than patients treated with ≤3 agents (40.2 months vs. 6.4 months, p < 0.00001). This difference could not be attributed to statistically significant differences in severity of liver disease or tumor stage, delay in treatment, previous treatment, concurrent nondrug treatment, or censoring effects;
2) The great effect is seen in patients treated with at least 4 agents that include Cordyceps sinensis. This greater certainty of patient survival without toxic side effects is significant benefit comparing with the conventional therapy. That is, treatment of HCC with a regimen of ≥4 agents prepared from natural products is associated with greater certainty of patient survival in a substantial portion of patients;
3) The information dynamic model for certainty of patient survival is derived based on fluid mechanics, where a series of approximate solutions of the flow between two parallel flat walls, one of which is at rest, the other is suddenly accelerated from the rest to a constant velocity are used;
4) The kinetic energy of certainty of patient survival decreases with increasing time, while the potential energy increases with increasing time;
5) Total mechanical energy of patients treated with 4 or more agents is smaller than that treated with 3 or fewer agents.
The kinetic energy (potential energy) of patients treated with 4 or more agents decreases (increases) more slower than the kinetic energy (potential energy) of patients treated with 3 or fewer agents.
![]()
![]()
REFERENCES
- Niwa, Y., Matsuura, H., Murakami, M., Sato, J., Hirai, K. and Sumi, H. (2012) Evidence that naturopathic therapy including Cordyceps sinensis prolongs survival of patients with hepatocellular carcinoma. Integrative Cancer Therapies (in press). doi:10.1177/1534735412441704
- Bruix, J. and Sherman, M. (2005) Management of hepatocellular carcinoma. Hepatology, 42, 1208-1236. doi:10.1002/hep.20933
- Llovet, J.M., Ricci, S., Mazzaferro, V., et al. (2008) Sorafenib in advanced hepatocellular carcinoma. The New England Journal of Medicine, 359, 378-390. doi:10.1056/NEJMoa0708857
- Niwa, Y., Miyachi, Y., Ishimoto, K. and Kanoh T. (1991) Why are natural plant medicinal products effective in some patients and not in others with the same disease? Planta Medica, 57, 299-304. doi:10.1055/s-2006-960102
- Cunningham, K.G, Manson, W. Spring, F.S. and Hutchinson, S.A. (1950) Cordycepin, a metabolic product isolated from cultures of Cordyceps militaries (Linn.) Link. Nature, 166, 949. doi:10.1038/166949a0
- Jagger, D.V., Kredich, N.M. and Guarrino, A.J. (1961) Inhibition of Ehrlich mouse ascites tumor growth by cordycepin. Cancer Research, 21, 216-220.
- Nakamura, K., Yoshikawa, N., Yamaguchi, Y., Kagota, S., Shinozuka, K. and Kunitomo, M. (2006) Antitumor effect of cordycepin(3’-deoxyadenosine) on mouse melanoma and lung carcinoma cells involves adenosine A3 receptor stimulation. Anticancer Research, 26, 43-47.
- Niwa, Y. and Sumi, H. (1999) Anti-cancer effect in vitro and clinical efficacy of a cancer therapeutic containing natural herbs, exposed to far infrared-ray heating and fermentation process using Aspergillus oryzae (in Japanese). Journal of Japan Society for Cancer Therapy, 34, 199.
- Hirai, K.I., Koyama, J., Pan, J. et al. (1999) Furanonaphthoquinone analog possessing preferential antitumor activity compared to normal cells. Cancer Detection and Prevention, 23, 539-550. doi:10.1046/j.1525-1500.1999.99052.x
- Itokawa, H., Totsuka, N. Morita, H. et al. (1990) New antitumor principles, casearins A-F, for Casearia sylvestris Sw.(Flacourtiaceae). Chemical and Pharmaceutical Bulletin (Tokyo), 38, 3384-3388. doi:10.1248/cpb.38.3384
- Gu, Y., Fujimiya, Y., Itokawa, Y. et al. (2008) Tumorricidal effects of beta-glucans: Mechanisms include both antioxidant activity plus enhanced systemic and topical immunity. Nutrition and Cancer, 60, 685-691. doi:10.1080/01635580802030884
- Su, Z.Y., Tung, Y.C., Hwang, L.S. and Sheen, L.Y. (2011) Blazeispirol A from Agarcicus blazei fermentation product induces cell death in human hepatoma Hep 3B cells through caspase-dependent and caspase-independent pathways. Journal of Agricultural and Food Chemistry, 59, 5109-5116. doi:10.1021/jf104700j
- Zhong, X.H., Wang, L.B. and Sun, D.Z. (2011) Effects of inotodiol extracts from inonotus obliquus on proliferation cycle and apoptotic gene of human lung adenocarcinoma cell line A549. Chinese Journal of Integrative Medicine, 17, 218-223. doi:10.1007/s11655-011-0670-x
- Niwa, Y., Kawahira, K. and Matsumoto, K. (1996) Effect of far infrared ray emitting products and stones on human leukocyte functions, lipid peroxidation, the growth of tumor on mice, drug-induced hepatitis rat, and clinical course and serum lipid peroxide levels of rheumatoid arthritis patients (in Japanese). Japanese Journal of Inflammation, 16, 425-436.
- Iida, H., Nakagawa, T. and Spoerer, K. (2012) Game information dynamic models based on fluid mechanics. Entertainment and Computing, 3, 89-99. doi:10.1016/j.entcom.2012.04.002
- Stokes, G. (1901) On the effect of the internal friction of fluids on the motion of pendulums. Mathematical and Physical Papers, 3, 1-141.
- Schlichting, H. (1968) Boundary-layer theory. 6th Edition, McGraw-Hill, New York.
- Hansen, M. (1928) Die Geschwindigkeitsverteilung in der Grenzschicht ab der längahgeströmten Platte. Journal of Applied Mathematics and Mechanics, 8, 185-199.
- Tsugé, S. (1974) Approach to origin of turbulence on the basis of two-point kinetic theory. Physics of Fluids, 17, 22-33. doi:10.1063/1.1694592
- Nakagawa, T. (2008) Dr. Shunichi Tsugé’s statistical theory of turbulence-microscopic view to motion of fluids, White. Mountains Academia Press, Hakusan.
- Nakagawa, T. and Chanson, H. (2002) Fluid mechanics for marine ecologists. Basic Edition, IPC Press, Tokyo.
- Nakagawa, T. and Chanson H. (2006) Fluid mechanics for marine ecologists. Applied Edition, IPC Press, Tokyo.
- Wang, C.Y. (1991) Exact solutionsof the steady-state Navier-Stokes equations. Annual Review of Fluid Mechanics, 23, 159-177. doi:10.1146/annurev.fl.23.010191.001111
- Solso, R. (1994) Cognition and the visual arts. MIT Press, Cambridge.