P. N. Hasse et al. / Open Journal of Stomatology 1 (2011) 172-178 177
cases (20%), there was the need for osteossynthesis in
three pillars and in only 1 patient (6.6%) one fixation
point was used.
Davidson et al. [14] analyzed, in an in vitro study,
several forms of fixation, combining steel wires, plates
and screws, obtaining a total of 25 different combina-
tions. By means of traction that simulated the action of
the masseter muscles they calculated the rotation and the
dislocation after the application of the forces on the dif-
ferent planes. The means of fixation that received the
best results were: fixation with steel wires in three points
and fixation with plates and screws in three points.
However, the stability reached by fixation with plates
and screws in two points was similar to the previous
fixations, highlighting the zygomatic pillar as the strate-
gic point for the opposition of the forces of th e masseter
muscle.
In relation to the combinations and the choice of os-
seous pillars, the combination between the frontozygo-
matic region and the zygomatic maxillary making up a
total of nine (60%) of the fifteen patients treated.
The zygomatic maxillary pillar should be the region of
choice for unstable fractures of the zygomatic bone, for
it acts as a direct antagonist to the action of traction
provoked by the masseter muscle [15].
Strong and Sykes [16] propose a combination of sys-
tems of mini-plates and micro-plates in the different pil-
lars of support of the ZMC. They recommend the use of
microplates of 1.0 or 1.2 mm in the infra-orbital border,
1.5 or 1.7 mm in the frontozygomatic region and 2.0 mm
in the zygomatic maxillary pillar region.
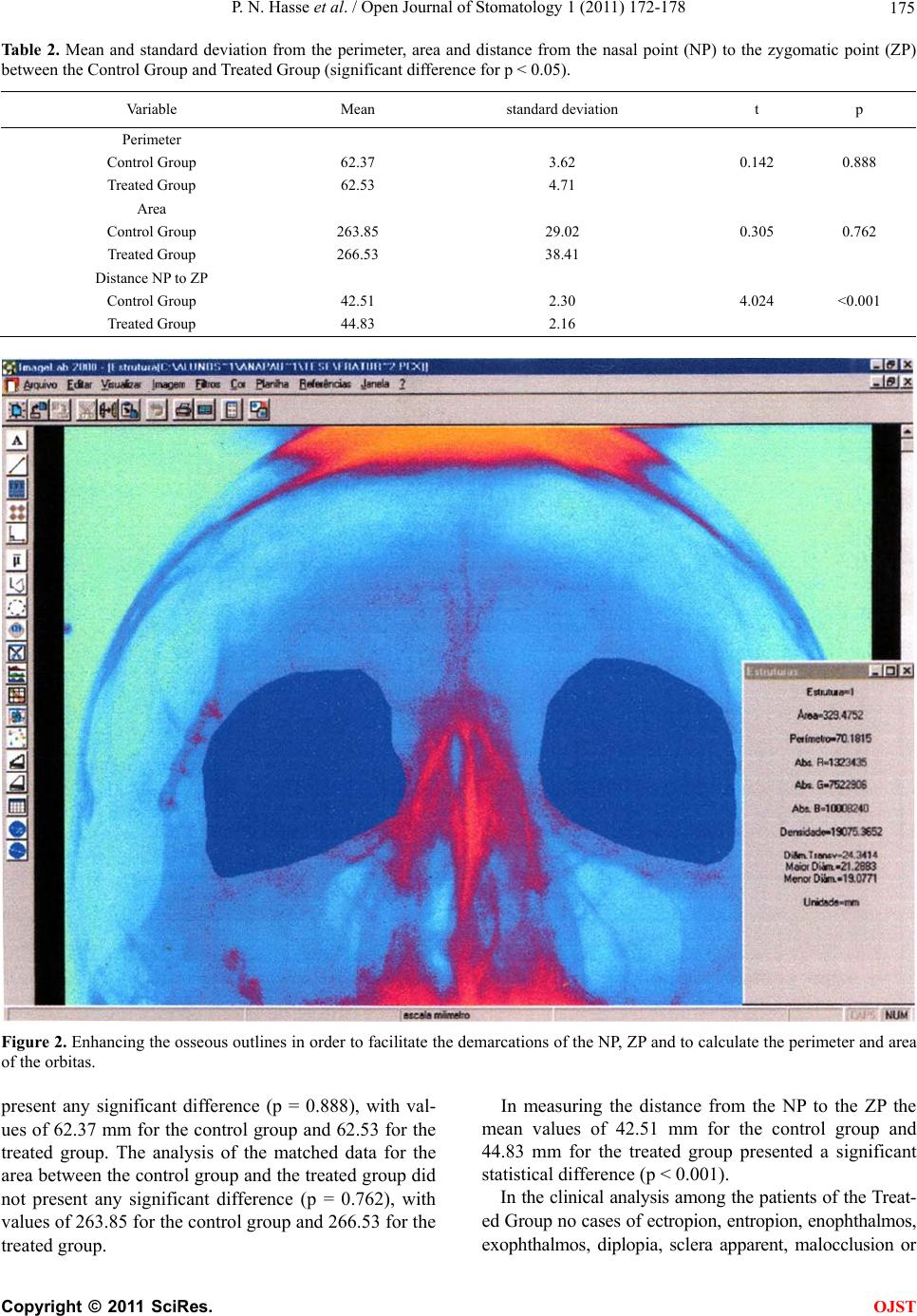
The data obtained from this study are in agreement
with the results obtained in other studies [17]. The diffe-
rences obtained, for the perimeter as well and for the
area of the operated side and the opposite side of the
Treated Group were not statistically significant.
The good stability obtained from the fixation in two
points gains force when compared with the sides obtain-
ed from the Control Group, in other words, the patients
who did not have fractures of the ZMC. In those we
verified that the differences in the values obtained be-
tween the right side and the left side, in referring to the
perimeter and, as well as the area, were also not statistic-
cally significant.
The distance from the NP to the ZP was also another
variable that was analyzed in this study with the aim to
determine a possible zygomatic asymmetry between the
opposite side and the treated side (Figure 3). The results
showed a significant difference between the sides in the
treated group, although the clinical analysis of this data
has not been made evident.
In the patients from the Treated Group a case of asy-
mmetry classified as “discreet” (6.6%) was found, pre-
senting dystopia, but with no complaints from the pa-
tient. Data that corroborates an incidence from 2% to 9%
of facial asymmetry in patients treated by a system of
internal rigid fixation [18,19]. However, in these, the
system used was of 2.0 mm, that structurally guarantees
the smallest rate of deflection, when compared to the
system of 1.5 mm.
The esthetic-functional items evaluated in this study
showed a significant improvement, principally related to
the “bother from the use of the plate”, related by the use
of the system 2.0 mm. One case was reported with dis-
comfort in the region of the zygomatic pillar, however,
associated with a symptomatology of disestesia in the re-
gion of the mucosa near the region with teeth and not
perceptible to palpation.
6. CONCLUSIONS
In this study the treatment of the unilateral fractures of
the zygomatic maxillary complex with the use of plates
and screws of the 1.5 mm system presented good esthe-
tic results and low rates of complications.
7. CONFLICT OF INTEREST
STATEMENT
The authors haven’t any financial and personal relation-
ships with other people or organizations that could inap-
propriately influence this work.
REFERENCES
[1] Rohrich, R.J. and Watumull, D. (1995) Comparison of
rigid plate versus wire fixation in the management of
zygoma fractures: A long-term follow-up clinical study.
Plastic and Reconstructive Surgery, 96, 570-575.
doi:10.1097/00006534-199509000-00008
[2] Fonseca, R.J., Walker, R.V., Betts, N.J. and Barber, H.D.
(1997) Oral and maxillofacial trauma. 2nd Edition, W. B.
Sauders, Philadelphia, 652.
[3] Zachariades, N., Mezitis, M. and Anagnostopoulos, D.
(1998) Changing trends in the treatment of zygomatico-
maxillary complex fractures: A 12-year evaluation of
methods used. Journal of Oral and Maxillofacial Surgery,
56, 1152-1157. doi:10.1016/S0278-2391(98)90759-5
[4] Luhr, H.G. (1998) A micro-system for cranio-maxillo-
facial skeletal fixation. Preliminary report. Journal of
Cranio-Maxillofacial Surgery, 16, 312-314.
doi:10.1016/S1010-5182(88)80069-6
[5] Reher, P. and Duarte, G.C. (1994) Miniplates in the fron-
tozygomatic region. An anatomic study. Journal of Oral
and Maxillofacial Surgery, 23, 273-275.
doi:10.1016/S0901-5027(05)80107-9
[6] Stevens, M.R. and Menis, M.A. (1993) Microscrew fixa-
tion of zygomatic arch fractures. Journal of Oral and
Maxillofacial Surgery, 51, 1158-1159.
doi:10.1016/S0278-2391(10)80460-4
[7] Covington, D.S., Wainwright, D.J., Teichgraeber, J.F. and
Parks, D.H. (1994) Changing pattern in the epidemiology
C
opyright © 2011 SciRes. OJST