Role of HLA-A, HLA-B, HLA-DRB1 and HLADQB1 Alleles in HIV-1 Patients with Pulmonary
138 Tuberculosis Co-Infection from Western India
studies on South Indian population, it is reported that
HLA-DQB1*06:01:01:01 plays a protective role against
HIV disease progression in Europeans [9]. In our study a
significantly increased frequency of HLA-DQB*06:01:
02 in HIV+ve/PTB+ve co-infected patients when com-
pared to controls and HIV+ve PTB-ve patients may suggest
its strong association with both HIV infection and PTB
co-infection. On the contrary HLA-DRB1* 06:01:01:01
frequency was significantly decreased in HIV+ve/PTB+
ve co-infected patients compared to controls, thereby
may protect from HIV infection and PTB development.
HLA-DQB1*05:02:01 allele is reportedly related to high
risk of developing TB in population from Asia and Latin
America [10]. In the present study, frequency of HLA-
DQB1*05:02:01 is increased in HIV+ve/PTB+ve co-
infected patients compared to healthy subjects to show
that HLA-DQB1* 05:02:01 may be associated with
HIV+ve/PTB+ve co-infection. There was no consider-
able change in frequency of HLA-A*26:01:01 in HIV+
ve/PTB+ve co-infected patients when compared with
controls and decreased frequency was observed when
compared with HIV+ve PTB-ve patients. This suggests
that, HLA-A*26:01:01 may not be associated with HIV
infection and may play a protective role in PTB devel-
opment. HLA-A*31 and HLA-B*41 antigens and the
HLA-DRB1*10 and HLA-DQB1*05 were over repre-
sented in Brazilian patients with AIDS and tuberculosis,
suggesting association to tuberculosis with AIDS [11].
As reported earlier HLA-DRB1*13 is associated with sus-
ceptibility to HIV-1 infection whereas HLA- DQB1*02: 03
and DRB1*01 are resistant to HIV-1 infection which
may vary in differen t ethnic group s [12]. HLA-DRB1* 15
is susceptible in PTB development and DRB1*11 may be
protective allele in Chinese population [6]. In the present
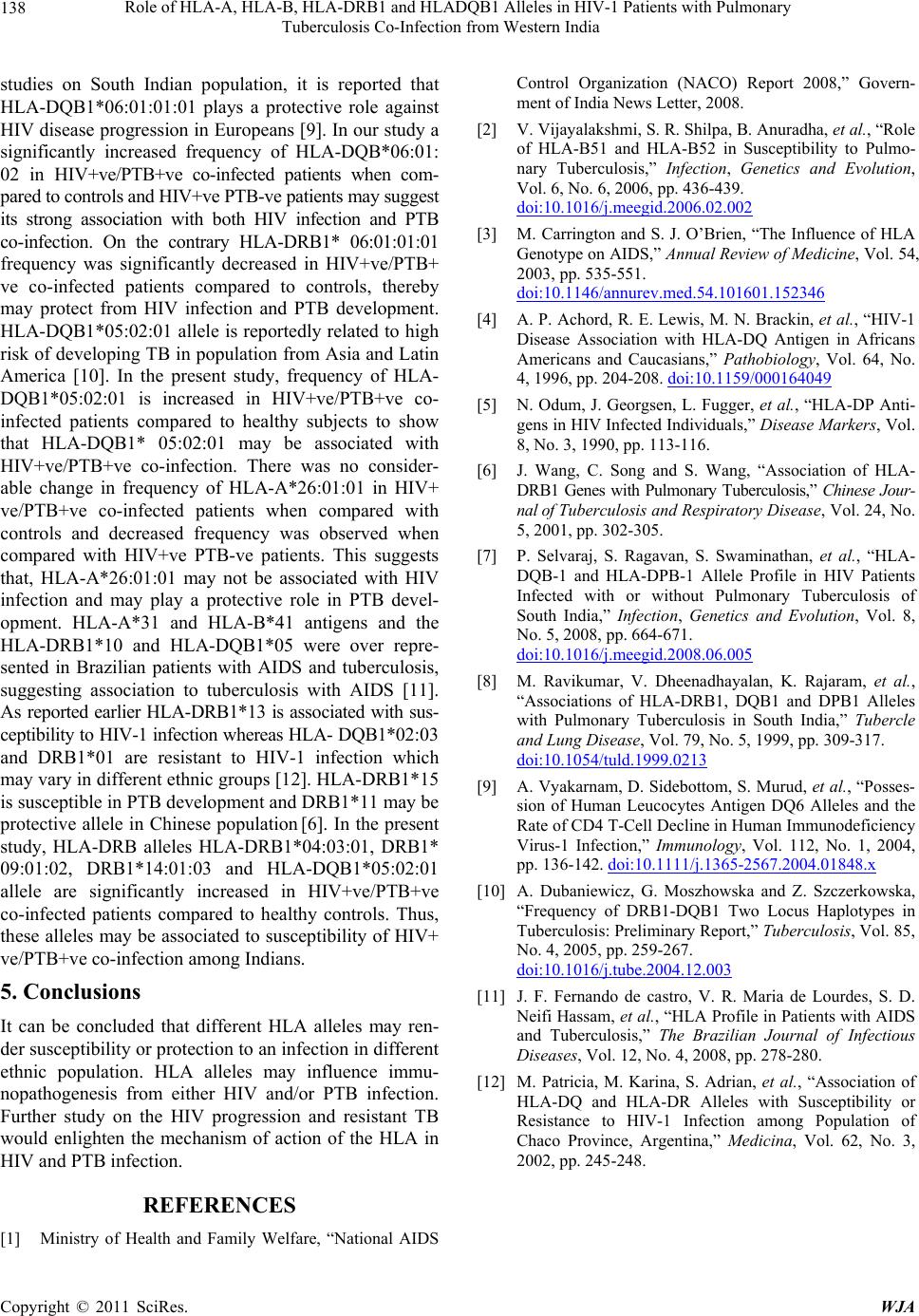
study, HLA-DRB alleles HLA-DRB1*04:03:01, DRB1*
09:01:02, DRB1*14:01:03 and HLA-DQB1*05:02:01
allele are significantly increased in HIV+ve/PTB+ve
co-infected patients compared to healthy controls. Thus,
these alleles may be associated to susceptibility of HIV+
ve/PTB+ve co-infection among Indians.
5. Conclusions
It can be concluded that different HLA alleles may ren-
der susceptibility or pro tection to an infection in differen t
ethnic population. HLA alleles may influence immu-
nopathogenesis from either HIV and/or PTB infection.
Further study on the HIV progression and resistant TB
would enlighten the mechanism of action of the HLA in
HIV and PTB infection.
REFERENCES
[1] Ministry of Health and Family Welfare, “National AIDS
Control Organization (NACO) Report 2008,” Govern-
ment of India News Letter, 2008.
[2] V. Vijayalakshmi, S. R. Shilpa, B. Anuradha, et al., “Role
of HLA-B51 and HLA-B52 in Susceptibility to Pulmo-
nary Tuberculosis,” Infection, Genetics and Evolution,
Vol. 6, No. 6, 2006, pp. 436-439.
doi:10.1016/j.meegid.2006.02.002
[3] M. Carrington and S. J. O’Brien, “The Influence of HLA
Genotype on AIDS,” Annual Review of Medicine, Vol. 54,
2003, pp. 535-551.
doi:10.1146/annurev.med.54.101601.152346
[4] A. P. Achord, R. E. Lewis, M. N. Brackin, et al., “HIV-1
Disease Association with HLA-DQ Antigen in Africans
Americans and Caucasians,” Pathobiology, Vol. 64, No.
4, 1996, pp. 204-208. doi:10.1159/000164049
[5] N. Odum, J. Georgsen, L. Fugger, et al., “HLA-DP Anti-
gens in HIV Infected Individuals,” Disease Markers, Vol.
8, No. 3, 1990, pp. 113-116.
[6] J. Wang, C. Song and S. Wang, “Association of HLA-
DRB1 Genes with Pulmonary Tuberculosis,” Chinese Jour-
nal of Tuberculosis and Respiratory Disease, Vol. 24, No.
5, 2001, pp. 302-305.
[7] P. Selvaraj, S. Ragavan, S. Swaminathan, et al., “HLA-
DQB-1 and HLA-DPB-1 Allele Profile in HIV Patients
Infected with or without Pulmonary Tuberculosis of
South India,” Infection, Genetics and Evolution, Vol. 8,
No. 5, 2008, pp. 664-671.
doi:10.1016/j.meegid.2008.06.005
[8] M. Ravikumar, V. Dheenadhayalan, K. Rajaram, et al.,
“Associations of HLA-DRB1, DQB1 and DPB1 Alleles
with Pulmonary Tuberculosis in South India,” Tubercle
and Lung Disease, Vol. 79, No. 5, 1999, pp. 309-317.
doi:10.1054/tuld.1999.0213
[9] A. Vyakarnam, D. Sidebottom, S. Murud, et al., “Posses-
sion of Human Leucocytes Antigen DQ6 Alleles and the
Rate of CD4 T-Cell Decline in Human Immunodeficiency
Virus-1 Infection,” Immunology, Vol. 112, No. 1, 2004,
pp. 136-142. doi:10.1111/j.1365-2567.2004.01848.x
[10] A. Dubaniewicz, G. Moszhowska and Z. Szczerkowska,
“Frequency of DRB1-DQB1 Two Locus Haplotypes in
Tuberculosis: Preliminary Report,” Tuberculosis, Vol. 85,
No. 4, 2005, pp. 259-267.
doi:10.1016/j.tube.2004.12.003
[11] J. F. Fernando de castro, V. R. Maria de Lourdes, S. D.
Neifi Hassam, et al., “HLA Profile in Pati ents with AIDS
and Tuberculosis,” The Brazilian Journal of Infectious
Diseases, Vol. 12, No. 4, 2008, pp. 278-280.
[12] M. Patricia, M. Karina, S. Adrian, et al., “Association of
HLA-DQ and HLA-DR Alleles with Susceptibility or
Resistance to HIV-1 Infection among Population of
Chaco Province, Argentina,” Medicina, Vol. 62, No. 3,
2002, pp. 245-248.
Copyright © 2011 SciRes. WJA