 Psychology 2011. Vol.2, No.9, 953-960 Copyright © 2011 SciRes. DOI:10.4236/psych.2011.29144 Assessing Effects of National Trauma on Adaptive Functioning of Mentally Healthy Adults: An Exploratory Rorschach Study Shira Tibon1,2, Lily Rothschild2,3, Liat Appel2, Ruth Zeligman1 1Department of Psychology, Academic College of Tel-Aviv Yaffo, Tel-Aviv, Israel; 2Department of Psychology, Bar Ilan University, Ramat Gan, Israel; 3Department of Psychology, University of Haifa, Haifa, Israel. Email: stibon@mta.ac.il Received September 13th, 2011; revised October 15th, 2011; accepted November 18th, 2011. The study evaluates deviations in Rorschach indices, usually related to effects of exposure to trauma, in three samples of Israeli adult non-patients. Data collected from 41 Israeli undergraduates in 1996-1997, during a pe- riod of increased rate of terror attacks in central cities of the country (Tibon, 2007), are compared to those of two similar samples of 49 and 30 undergraduates collected in 2005-2007, before and after the Second Lebanon War respectively. During this period, the rate and severity of terror attacks were lower. The results point out the 1996-1997 sample (High Terror Exposure) as showing prominent difficulties in the capacity to minimize felt distress, in comparison to the other two samples, collected between January 2005 and January 2006 (Low Terror Exposure) and between October 2006 and January 2007 (Lebanon War Exposure) respectively. Nonetheless, the Lebanon War Exposure sample showed a tendency towards being alert and suspicious in interpersonal relation- ships. The data are interpreted as demonstrating the utility of the Rorschach as an assessment tool that is more responsive than previously thought to non-personality contextual factors such as national trauma. Keywords: National Trauma, Terror, Mental Functioning, Distress Measures, Rorschach Introduction Empirical research and clinical experience with people who were exposed to national traumatic events such as war or terror attacks have shown that both children and adults who were present at the events would most frequently develop severe stress reactions and psychopathological syndromes (Barenbaum, Ruchkin, & Schwab-Stone, 2004; Fremont, 2004; Joshi & O’Donnell, 2003; Sadeh, Hen-Gal, & Tikotzky, 2008; Shaw, 2003; Twemelow, 2004). Moreover, there is evidence that a person needs not be present to have stress symptoms. Repli- cated findings of studies conducted in the US following Sep- tember 11, 2001, and in the UK following the terror attacks in 2005 describe substantial levels of stress in large numbers of nonpatients who do not fit into the traditional definition of ex- posure to trauma. These studies suggest that deliberate inflic- tion of distress, as occurring in a collective traumatic event, is a particularly potent psychological stressor. Furthermore, an on- going threat of terrorism has been shown to affect both the severity and duration of posttraumatic stress responses (Gidron, 2002; Rubin, Brewin, Greenberg, Simpson, & Wessely, 2005; Schuster et al., 2001; Shalev, 2000; Silver, Holman, McIntosh, Poulin, & Gil-Rivas, 2002; Torabi & Seo, 2004). Apart from posttraumatic stress responses, effects of trau- matic incidents have been shown in various psychopathological syndromes commonly encountered in clinical settings, include- ing dissociative reactions, depression, anxiety, substance abuse, and even psychotic conditions (Galea et al., 2002; Gold, 2008; Sautter et al., 1999; Shalev et al., 1998). Studies that examine the inner experience of people who were under extreme threat- ening situations such as persecution, arrest, deportation, and imprisonment consistently show that these people are prone to perceive reality in a constrained, dissociative, or paranoid-like manner devoid of continuity and structure. These studies con- clude that cognitive distortions, such as proneness to confuse inner and outer worlds, would be one of the inevitable cones- quences of persecution (Schreuder, 2001). The systematic study of the impact of trauma on psychology- cal functioning is relatively new and the standard assessment protocol for evaluating traumatized people has typically been restricted to a clinical interview and self-report psychometric scales. However, there has been growing empirical evidence that point out the Rorschach Inkblot Method (Rorschach, 1921) as a valid tool that might be very useful for clarifying psycho- logical experiences in both children and adult traumatized pa- tients (Armstrong & Loewenstein, 1990; Brand, Armstrong, & Loewenstein, 2006; Brand, Armstrong, Loewe nstein, & McNary , 2009; Carlson & Armstrong, 1994; Clinton, & Jenkins-Monroe, 1994; Goldfinger, Amdur, & Liberzon, 1998; Hartman et al., 1990; Holaday, 2000; Leavitt & Labott, 1998; Lerner, 1998; Sloan, Arseault, Hilsenrot h, Harvill, & Handler, 1995; Steinberg, 1996; Swanson, Blount, & Bruno,1990; Viglione, 1990; Zelig- man, Smith, & Tibon, 2011). Unlike self-report measures, the nature of the Rorschach task does not require awareness to internal experience of the trau- matized person and is not vulnerable to over reporting. The method can therefore be especially useful for unveiling dy- namic processes (e.g., dissoci ative distancing from inner reality) that often characterize people who were exposed to trauma. Rorschach indices that have been usually explored in relation to effects of trauma are based on the Comprehensive System (CS; Exner, 1974, 2003), currently the most frequently used method for applying the Rorschach in research and practice. These indices include both markers that point out incapacity to mini- mize subjective distress, and those demonstrating proneness to  S. TIBON ET AL. 954 psychopathological manifestations in the affective, interper- sonal and cognitive realms. Rorschach Markers of Trauma Effects Rorschach Markers of Incapacity to Minimize Subjective Distress D and AdjD. The D and AdjD scores are CS indices that rep- resent situationally-related and chronic failure to maintain a sense of psychological equilibrium respectively (Exner, 2003; Weiner, 2003; Weiner & Greene, 2008). These are the most comprehensive CS constellation indices, composed of all the major variables of available mental resources as compared to the experienced demands of reality. Several studies showed that a high percentage of traumatized people present D and AdjD scores that are below the cutoff point of 0, presumed to indicate incapacity to minimize situational and chronic distress respect- tively. Lowered D and AdjD have consistently been found among veterans from Vietnam or those who served at the Gulf War, and were significantly different from those found in a control group of soldiers who did not participate in war (Hart- man et al., 1990; Levin, 1993; Sloan et al., 1995). These find- ings demonstrate how coping is undetermined by the acute and chronic management of intrusive thoughts and sense of help- lessness that constitute substantial factors in traumatic experi- ence (Wilson & Keane, 1997). Furthermore, Sloan, Arsenault, Hilsenroth, Handler, and Harvill (1996) found that the signify- cantly lowered D and AdjD scores of those exposed to war stressors disappeared in a follow-up study conducted three years after the initial collection of data. Rorschach Markers of Pronessness to Psychopathological Manifestations S-CON. The S-CON is a CS constellation index that was validated as a measure of self-destructiveness in adolescents and adults. The index was found to be significant in samples of adult patients indicating high level of distress (Exner, 2003; Fowler, Piers, Hilsenroth, Holdwick, & Padawer, 2001). Al- though usually not applicable for children, Clinton and Jen- kins-Monroe (1994), found significant S-CON in children who were sexually abused. Thus, within the clinical setting the S-CON is suggested to be used in all cases of traumatized ado- lescents and adults. DEPI. The Depression Index (DEPI) is a CS measure of general distress. Exner and Weiner (1995) pointed to a signify- cant DEPI as being associated primarily with a persistent dis- position towards recurring episodes of depression. Review of Rorschach studies of patients in different age groups shows mixed findings as to the predictive power of the DEPI in rela- tion to DSM interview-based diagnoses (Jorgensen, Andersen, & Dam, 2000). These studies show that a significant DEPI is unrelated to observable behaviors that fit into DSM diagnoses of mood disorders. Nonetheless, it can be used as a constella- tion index for evaluating level of subjective distress. Elevated DEPI was found among children and adolescents diagnosed with Post Traumatic Stress Disorder (PTSD) as compared to American reference data (Holaday, 2000), and in sexually abused girls being compared to a matched clinical group with- out history of abuse (Leifer, Shapiro, Martone, & Kassem, 1991), pointing out the depressive component of PTSD in chil- dren and adolescents. Nonetheless, Rorschach depressive indi- cators in protocols of traumatized adults seem to be less obvi- ous (Frueh, Leverett, & Kinder, 1995). HVI. The Hypevigilance Index (HVI) is a CS measure of high alertness to potential sources of threat and is scored posi- tive when the protocol does not include any Texture responses (T) and four or more of seven other findings included in the index are significant. A positive HVI is considered to be related to projection of anger and hostility (Exner, 2003; Weiner, 2003; Weiner & Greene, 2008). Exner (2003) found a positive HVI in 88% of patients diagnosed with paranoid schizophrenia and in 90% of a sample of patients with paranoid personality disorder. Studies in traumatized people showed elevated HVI scores, representing over-alertness and watchfulness associated with traumatic experiences (Levin, 1993). HVI was used in the cur- rent study as a dimensional variable (independent of T). As such, it captures a cautious and detail oriented approach in scanning the environment, underlying alertness, suspiciousness, anger, and a need to protect and distance oneself in interper- sonal relationships. PTI. The Perceptual Thinking Index (PTI) is a CS constella- tion index of impaired cognitive functioning. It was developed as a revised version of the Schizophrenia Index (SCZI), both evaluating ideational clarity and perceptual accuracy. These indices were consistently found as valid measures in differenti- ating schizophrenia-spectrum patients from non-patients and patients diagnosed with other psychopathological conditions including mood disorder with no psychotic features (Exner, 2003; Dao, & Prevatt, 2006). The PTI was empirically vali- dated as a measure of thinking disturbances when used cate- gorically with a cutoff score of 3 (Weiner & Greene, 2008). Elevated SCZI or PTI were found in Rorschach protocols of adults with traumatic background as compared to those without history of trauma (Smith, Chang, Kochinski, Patz, & Nowinski, 2010), and in those of traumatized children and adolescents (Holaday, 2000; Viglione, 1990) as compared to reference data. These findings were interpreted as showing cognitive disrupt- tion, when victims cannot comprehend or make sense of the irrational, illogical, and confusing experiences. TCI. The Trauma Content Index (TCI; Armstrong & Loewen- stein, 1990) is a constellation index based on CS variables that measures traumatic associations as being revealed in the Ror- schach protocol. Elevated TCI scores are considered to be in- dicative of intrusion of traumatic related material, bodily pre- occupation, a sense of being impaired, and concerns about physical integrity. Previous research found elevated TCI among traumatized children, adolescents and adults with or without diagnosis of dissociative disorders (Brand et al., 2006; Brand et al., 2009; Kamphuis, Kugeares, & Finn, 2000; Scroppo, Drob, Weinberger, & Eagle, 1998; Smith et al., 2010). RFS. The Reality-Fantasy Scale (RFS; Tibon, Handelzalts, & Weinberger, 2005) is a Rorschach index designed to operation- alize Winnicott’s (1971) construct of potential or transitional space between reality and fantasy, as explored by Ogden (1989) in relation to different psychopathological states. Following Smith (1990), the RFS applies Ogden’s model to Rorschach work, defining a person’s proneness to show psychopathologi- cal manifestations (e.g., psychotic thinking) in terms of differ- ent forms of collapse of potential space. Previous research in traumatized patients diagnosed with dissociative disorders showed significantly lowered RFS scores, indicating psy- chotic-like cognitive functioning as being revealed by collapse of reality into fantasy (Zeligman, Smith, & Tibon 2010). Normative D ata The Rorschach CS has stimulated many empirical studies addressed at measuring and improving the reliability, validity,  S. TIBON ET AL. 955 and normative data of the test (Exner & Erdberg, 2006; Vig- lione & Meyer, 2008; Weiner, 1996, 2001; Weiner & Greene, 2008). Recently, Meyer, Erdberg, and Schaffer (2007) con- ducted an international project that compared CS normative data across 17 samples of adults and 31 samples of children and adolescents from around the world. Overall, the data concern- ing the adult samples in this project revealed a reasonable de- gree of cross-national similarity, further confirming the Ror- schach as a valid tool of personality assessment. The Israeli sample of 41 students (Tibon, 2007), which was included in the composite international sample, showed devia- tions in CS markers of subjective distress. These deviations in CS affective markers were not demonstrated in other realms of mental functioning (e.g., cognitive, interpersonal) as compared to the usually accepted CS cutoff scores of these measures. Thus, although each of the participants in this sample fitted into the definition of non-patients, the whole group showed substan- tial signs of distress. The deviations found in the Israeli sample were interpreted as related to the traumatic events within the political context of the Middle East. The Rorschach protocols were collected in two periods during 1996-1997 (January 1996-February 1996; July 1997-September 1997) which followed the assassination of Prime Minister Rabin in November 1995, and the collapse of the Middle East peace process, resulting in prominent escala- tion in the relationships between the State of Israel and the Palestinian Authority. Data published by the Israeli Ministry of Foreign Affairs (2008) show that during these months there were 10 terror attacks with 52 people killed and hundreds in- jured. These terror attacks were conducted mostly in major cities in the center of the country and exposed the entire Israeli population to constant unpredictable threat of terror. When the published data are organized into quarterly sum- maries for the years 1993 through 2008 it is clear that the 1996- 1997 sample was obtained during extreme stress. In fact, these dates correspond to the two quarters that documented the greatest number of attacks and the greatest number of people who were killed or injured from 1994 to 2000. The national trauma of Rabin’s assassination and the collapse of the peace process was thus exacerbated by the terror attacks extremely threatening the daily experience of the Israeli citizens. As re- vealed by the data another spike in terror threat was in 2002. However, since 2002 there was a gradual decrease in the num- ber of people killed in terror attacks to15 in 2006 and 3 in 2007. Furthermore, the Second Lebanon War in 2006 was felt as a real threat mainly in northern Israel, while people in the center of the country, who were not exposed to the direct threat of war, did not change their daily routine. The focus of the present study was to compare markers of distress in a sample of Israeli non-patients collected during a period of increased rate of terror attacks (High Terror Exposure) to samples collected during periods of reduced rate of terror attacks before and after the Second Lebanon War. In line with the published data on terror attacks and empirical Rorschach data that point out elevation in Rorschach distress markers in traumatized patients, it was hypothesized that the deviations in the CS markers of subjective distress, shown in the Israeli sample, actually reflected the fact that the sample was collected within the context of national trauma (Tibon, 2007; Meyer et al., 2007). The present study was aimed at fur- ther exploring this hypothesis. Accordingly, the main hypothe- sis was that similar samples of non-patients that were collected in less traumatic periods, would differ from the High Terror Exposure sample, collected in 1996-1997, as to Rorschach markers of incapacity to minimize felt distress (D, AdjD). The study further explored the differences between the samples as to Rorschach markers of proneness to psychopathological manifestations in the affective (S-CON, DEPI), interpersonal (HVI), and cognitive (TCI, PTI, RFS-P) functioning. Method Participants Participants were drawn from three samples of Israeli under- graduates studying in academic institutes in major cities at the center of the country. Data collection for the first sample (High Terror Exposure) took place in two distinct periods: January 1996-February 1996 (N = 24); and July 1997-September 1997 (N = 26). From the 50 participants originally included in this sample, nine individuals were dropped by applying exclusion criteria of severe psychopathological symptoms, past psy- chiatric hospitalization or receiving mental health services within the past two years including the time of testing (Tibon, 2007). The sample of 41 participants, within the age range of 19 - 35 years, was composed of 20 males and 21 females, all of them Jewish who were born in Israel. Data collection for the second sample (Low Terror Exposure) took place in January 2005-January 2006. In this sample, 36 protocols were administered between January and July 2005, and 23 between October 2005 and January 2006. From the 59 participants originally included in this sample, ten were dropped by applying the same exclusion criteria as in the 1996-1997 sample. The sample of 49 participants, within the same age range as the High Terror Exposure sample, was composed of 19 males and 30 females, all of them Jewish who were born in Israel. Comparing the two samples as to the percentage of males and fema les did not show significant difference (χ2 = .91, p = ns, r = .10). The third sample (Lebanon War Exposure) originally in- cluded 36 participants who were administered the Rorschach in October 2006-January 2007, following the war. From the 36 participants, two were excluded by applying the same psychiat- ric criteria applied in the previous samples, two were excluded because they served in the Israeli army during the war, and two by applying an exclusion criterion of place of permanent resi- dence in the northern part of country, which was exposed to the missiles and rockets lunched by the Hizbollah during the war. The sample of 30 participants, within the same age range of 19 - 35 years, was composed of 5 males and 25 females, al l of them Jewish who were born in Israel. Because comparison with the High Terror Exposure sample showed significant relation- ship between gender and sample affiliation (χ2 = 7.83, p < .05, r = .33), preliminary analyses were conducted to control for the gender distribution in the three samples, using ANOVA for gender × sample for all the dependent variables. These analyses did not show any main effect for gender. Participants in all three samples were in Israel for most of the time during which the terrorist attacks and war took place. However, none of the respondents was personally involved in any of the war or terror occurrences that took place in the country at the time of the study. Rorschach Measures Following Rorschach studies in traumatized people, we have selected eight indices for comparing the samples. The decision of selecting constellation indices rather than individual vari-  S. TIBON ET AL. 956 ables was based on the assumption that essentially scales with a greater number of items from a conceptually related category would be more reliable and more stable than a single item from the same pool (Nunnally & Bernstein, 1994). Six of the con- stellations, D and AdjD scores, S-CON, DEPI, HVI, and PTI, are included in the CS (Exner, 2003). Although the two addi- tional indices, the Traumatic Content Index (TCI; Armstrong & Lowenstein, 1990) and the Reality-Fantasy Scale (RFS; Tibon, Handelzalts, & Weinberger, 2005), are not included in the CS, they are based on the system’s original variables and can there- fore be applied by its users. As noted, the D and AdjD are assumed to measure incapacity to minimize situational and chronic distress respectively when their value is below the cutoff point of 0. The S-CON is a statis- tically generated constellation index designed to predict self- destructive potential. The index consists of 12 variables and ratios that together yield a single score in which 8 is used as a cutoff point. The DEPI is a measure of general distress that consists of 15 variables organized in seven conditions and is considered to be clinically significant when it exceeds the cut- off point of 5, indicating proneness to show mood disorders or a chronic disposition to recurrent depressive episodes. The HVI is a measure of high alertness to potential sources of threat. HVI was used in the current study as a dimensional variable, captur- ing a hyper vigilant approach in scanning the environment, and a need to protect and distance oneself in interpersonal relation- ships. The PTI is a global index of impaired cognitive func- tioning, composed of eight Rorschach variables that are in- cluded in five-criteria constellations based on combination of different values. The TCI is a measure of traumatic associations composed of five CS variables of Anatomy (An), Blood (Bl), Sex (Sx), Ag- gressive (AG), and Morbid (MOR) responses, divided by the total number of responses in the protocol. Since there are no published cutoff points for the TCI, the study used the average TCI scores found in traumatized inpatients (M = .50; SD = .40) and outpatients (M = .21; SD = .14) as a reference point against which to assess whether the TCI should be considered clinically significant (Brand et al., 2006; Kamphuis et al., 2000; Smith et al., 2010). The RFS is an evidence-based psychoanalytically oriented index that is composed of CS variables and an additional spe- cial score of Reality Collapse (RC). The 11-point scale ranges from –5 (reality collapse into fantasy) to +5 (fantasy collapse into reality). A score of –5 represents the most extreme reliance on fantasy with minimum contact with external reality and a score of +5 represents a strong reliance on the real features of the blot with minimal input of fantasy. A mean RFS score of a given protocol (RFS-P) is expected to be within the range of –.51 to +.65 in m entally health y adults. Procedure Participants in all three samples were recruited through word of mouth and were neither paid nor given extra credit in their psychology classes for participation. However, they were of- fered a meeting with a senior psychologist in which they would be provided with feedback on testing results in exchange for their participation. Half of the participants in each of the sam- ples applied for a feedback meeting that was conducted by the examiner a few weeks following the administration of the test. The administration and scoring procedures of the three sam- ples followed the CS guidelines available at the time of the study. Accordingly, the administration and scoring procedures for the High Terror Exposure sample followed the guidelines of Exner (1995) and those for the two other samples followed the guidelines as presented by Exner (2001). There are minor dif- ferences between the two versions consisting mainly of addi- tional prompts given to the subject in the 2001 edition. In line with previous research (e.g. Meyer et al., 2007) the different administration procedures did not produce significant differ- ences as to the number of responses. Since seating next to the testee, as recommended by Exner (1995, 2001), might raise hurdles in some groups in Israel because of religious constrict- tions regarding physical closeness, seating procedures were diagonally opposite. These procedures are in line with the guidelines provided by Allen and Dana (2004) stating that cul- tural adaptations may dictate departures from CS procedures in research studies. In all three studies test responses were pro- vided by the participants in Hebrew. In the High Terror Expo- sure sample the examiners coded their own protocols and then an advanced student or an expert recoded each of the protocols. Following this initial phase, a sample of the recoded responses were examined by six groups of raters, each of them included the two raters that originally scored the protocol. Interrater reliability was computed for a sample of 35 protocols randomly selected from the original sample. In the Low Terror Exposure and Lebanon War Exposure samples, we used a similar scoring procedure, in which all responses were first coded by the ex- aminer and then by another coder, an advanced student super- vised by a senior clinician. Following this initial phase, the scoring of all the responses was reexamined by a senior clini- cian. Interrater reliability for all the protocols in both samples was computed. Results of interrater reliability, computed for the different CS segments (Location & Space; Developmental Quality; Deter- minants; Form Quality; Pairs; Contents; Popular Responses; Special Scores), showed agreement percentages ranging fro m .90 to 1.00 in the High Terror Exposure Sample, from .80 to .96 in the Low Terror Exposure Sample, and from .96 to 1.00 for the Lebanon War Exposure Sample. The results of interrater reli- ability in all the three samples meet the recommended criteria for agreement statistics in Rorschach studies. Results Results of oneway ANOVA which compared the three sam- ples as to the number of responses (R) did not show significant differences (High Terror Exposure: M = 22.12, SD = 8.02; Low Terror Exposure: M = 23.08, SD = 8.53; Lebanon War Expo- sure: M = 23.30, SD = 9.24). Furthermore, the mean number of responses did not deviate from that of the composed interna- tional sample (M = 22.31, SD = 7.90). Table 1 presents the means and standard deviations for Ror- schach markers of incapacity to minimize distress in the three samples. Results of oneway ANOVA show that the D and AdjD scores, indicating incapacity to minimize situational and chronic distress respectively, significantly differed across the three samples, with F(2, 117) = 9.61, p < .001, d = .38 for D, and F(2, 117) = 9.82, p < .001, d = .38 for AdjD respectively. Scheffe post-hoc comparisons indicated that the High Terror Exposure respondents showed significantly lowered D and AdjD as com- pared to those of Low Terror Exposure sample. Furthermore, these results were also shown when post-hoc Bonferroni cor- rection (p < .05/8 = .006) was applied. Table 2 presents the means and standard deviations for Ror- schach markers of proneness to psychopathological manifesta- tions in the affective (S-CON, DEPI), interpersonal (HVI), and 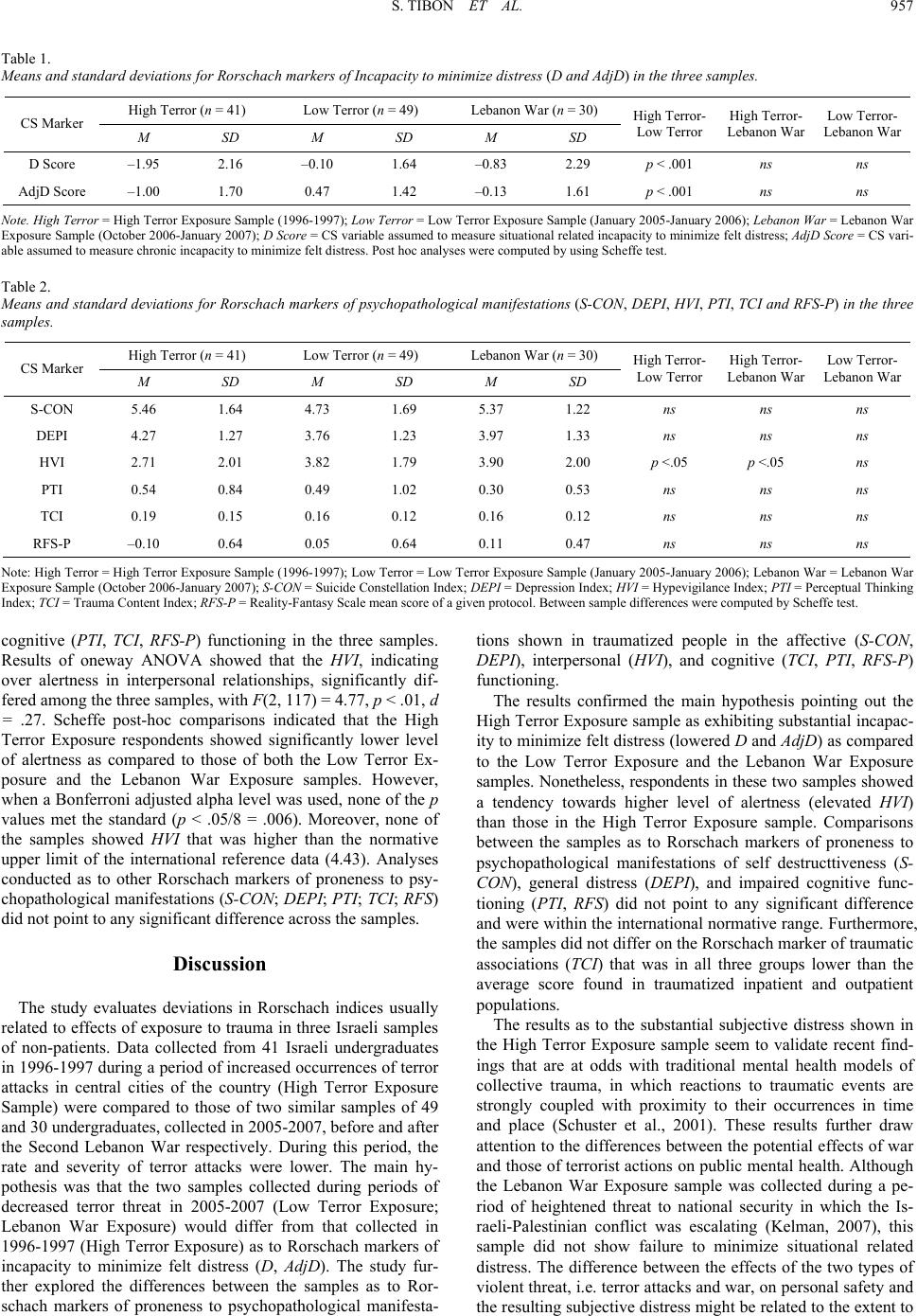 S. TIBON ET AL. 957 Table 1. Means and standard deviations for Rorschach markers of Incapacity to minimize distress (D and AdjD) in the three samples. High Terror (n = 41) Low Terror (n = 49) Lebanon Wa r ( n = 30) CS Marker M SD M SD M SD High Terro r - Low Terror High Terro r - Lebanon War Low Terror- Lebanon War D Score –1.95 2.16 –0.10 1.64 –0.83 2.29 p < .001 ns ns AdjD Score –1.00 1.70 0.47 1.42 –0.13 1.61 p < .001 ns ns Note. High Terror = High Terro r Exposure Sample (1 996-1997); Low Terror = Low Terror Exposure Sample (January 2005-Jan uary 2006); Lebanon War = Lebanon War Exposure Sample (Octob er 2006-Janua ry 2007); D Score = CS variable assumed to measure situational related incapacity to minimize felt distress; AdjD Score = CS vari- able assumed to measure c hronic incapacity to minimize felt di stress. Post hoc analyses were computed by using Scheffe tes t. Table 2. Means and standard deviations for Rorschach markers of psychopathological manifestations (S-CON, DEPI, HVI, PTI, TCI and RFS-P) in the three samples. High Terror (n = 41) Low Terror (n = 49) Lebanon Wa r ( n = 30) CS Marker M SD M SD M SD High Terro r - Low Terror High Terro r - Lebanon War Low Terror- Lebanon War S-CON 5.46 1.64 4.73 1.69 5.37 1.22 ns ns ns DEPI 4.27 1.27 3.76 1.23 3.97 1.33 ns ns ns HVI 2.71 2.01 3.82 1.79 3.90 2.00 p <.05 p <.05 ns PTI 0.54 0.84 0.49 1.02 0.30 0.53 ns ns ns TCI 0.19 0.15 0.16 0.12 0.16 0.12 ns ns ns RFS-P –0.10 0.64 0.05 0.64 0.11 0.47 ns ns ns Note: High Terror = High Terror Exposure Sample (1996-1997); Low Terror = Low Terror Exposure Sample (January 2005-January 2006); Lebanon War = Lebanon War Exposure Sample (Octob er 2006 -January 2007); S-CON = Suicide Constellation Index; DEPI = Depression Index; HVI = Hypevigilance Index; PTI = Perceptual Thinking Index; TCI = Trauma Conte nt Index; RFS-P = Reality-Fantasy Scale mean score of a given protocol. Between sample differences were computed by Scheffe test. cognitive (PTI, TCI, RFS-P) functioning in the three samples. Results of oneway ANOVA showed that the HVI, indicating over alertness in interpersonal relationships, significantly dif- fered among the three samples, with F(2, 117) = 4.77, p < .01, d = .27. Scheffe post-hoc comparisons indicated that the High Terror Exposure respondents showed significantly lower level of alertness as compared to those of both the Low Terror Ex- posure and the Lebanon War Exposure samples. However, when a Bonferroni adjusted alpha level was used, none of the p values met the standard (p < .05/8 = .006). Moreover, none of the samples showed HVI that was higher than the normative upper limit of the international reference data (4.43). Analyses conducted as to other Rorschach markers of proneness to psy- chopathological manifestations (S-CON; DEPI; PTI; TCI; RFS) did not point to any significant difference across the samples. Discussion The study evaluates deviations in Rorschach indices usually related to effects of exposure to trauma in three Israeli samples of non-patients. Data collected from 41 Israeli undergraduates in 1996-1997 during a period of increased occurrences of terror attacks in central cities of the country (High Terror Exposure Sample) were compared to those of two similar samples of 49 and 30 undergraduates, collected in 2005-2007, before and after the Second Lebanon War respectively. During this period, the rate and severity of terror attacks were lower. The main hy- pothesis was that the two samples collected during periods of decreased terror threat in 2005-2007 (Low Terror Exposure; Lebanon War Exposure) would differ from that collected in 1996-1997 (High Terror Exposure) as to Rorschach markers of incapacity to minimize felt distress (D, AdjD). The study fur- ther explored the differences between the samples as to Ror- schach markers of proneness to psychopathological manifesta- tions shown in traumatized people in the affective (S-CON, DEPI), interpersonal (HVI), and cognitive (TCI, PTI, RFS-P) functioning. The results confirmed the main hypothesis pointing out the High Terror Exposure sample as exhibiting substantial incapac- ity to minimize felt distress (lowered D and AdjD) as compared to the Low Terror Exposure and the Lebanon War Exposure samples. Nonetheless, respondents in these two samples sho wed a tendency towards higher level of alertness (elevated HVI) than those in the High Terror Exposure sample. Comparisons between the samples as to Rorschach markers of proneness to psychopathological manifestations of self destructtiveness (S- CON), general distress (DEPI), and impaired cognitive func- tioning (PTI, RFS) did not point to any significant difference and were within the international normative range. Furthermore, the samples did not differ on the Rorschach marker of traumatic associations (TCI) that was in all three groups lower than the average score found in traumatized inpatient and outpatient populations. The results as to the substantial subjective distress shown in the High Terror Exposure sample seem to validate recent find- ings that are at odds with traditional mental health models of collective trauma, in which reactions to traumatic events are strongly coupled with proximity to their occurrences in time and place (Schuster et al., 2001). These results further draw attention to the differences between the potential effects of war and those of terrorist actions on public mental health. Although the Lebanon War Exposure sample was collected during a pe- riod of heightened threat to national security in which the Is- raeli-Palestinian conflict was escalating (Kelman, 2007), this sample did not show failure to minimize situational related distress. The difference between the effects of the two types of violent threat, i.e. terror attacks and war, on personal safety and the resulting subjective distress might be related to the extent to  S. TIBON ET AL. 958 which civilians were able to be actively engaged in their own defense. Research indicates that unlike the perils of war, threat of terrorism offers no trusted safety signal such as siren nor safe places (Shalev, 2006). On the other hand, factors decreasing feelings of helplessness during war (e.g., anti-aircraft batteries) might give people a sense of being in control. Furthermore, mass terrorist attacks are highly visible disasters that are de- signed to affect not only those in direct vicinity of the attacks but the population at large. Consequently, the boundaries be- tween direct and indirect exposure are blurred, resulting in sub- stantial consequences among those who are directly as well as indirectly affected by the attacks (Galea et al., 2002; Galea & Resnick, 2005). Another factor that magnifies the traumatic impact of terrorism is its impersonal and apparently random nature. Terror attacks innocent civilians rather than professional soldiers, and is promoted by violence detached from symbolic meaning. A culture is often unable to cope and to come up with useful solutions to something that is perceived as impersonal and lacking symbolic meaning (Fonagy, 2003; Twemlow & Sacco, 2002). With respect to the inferences drawn from the results as to public mental health, the nature of the conclusions touches on the differences between absolute and relative perspectives on normality. Ordinarily, normative Rorschach non-patient data provide descriptive information about groups and offer refer- ence points for comparing individual scores. Most important is the basis they provide for developing some general interpretive guidelines, using the deviation principle for evaluating whether or not specific findings fit into the normative range (Exner & Erdberg, 2005). The present results demonstrate that CS coun- try-specific normative data, collected at different points of time, might show deviations from the international norms because of changing external conditions rather than because of personality predispositions. Indeed, when a group of people is exposed to collective traumatic events some may develop a stress disorder while others may not. However, assessing what circumstances may have led to a stress disorder may have implications for treatment and prognosis. Showing acute, reactive disturbances following national traumatic events requires different therapeu- tic intervention than a chronic, persistent disorder. Nonetheless, in Israel and other immigrant countries, in which the popula- tions receive mental health services and assessment outside of their country of origin, where certain collective traumatic events would not be accounted for in the country’s norms, cli- nicians should be aware of the patients’ historical context. Nonetheless, the individuals who showed substantially ele- vated distress in the High Terror Exposure sample were unlikely to function as effectively as they would be able to with less experienced stress. The mean D Score shown in this sam- ple was deviant relative to what is expected even though it ap- pears to be deviant because the Rorschach seems to be sensitive to contextual factors. Thus, although a specific Rorschach marker is found to be normative and adaptive in a certain coun- try, it does not mean that one can ignore its implications for clinical practice and/or mental health policy. The Rorschach, when used for diagnostic purposes, shows a person’s status with respect to deviations from normative standards. If a large majority in a certain country shows signs of being distressed, their stress is not deviant from a cultural perspective, but it is certainly deviant from a clinical perspective. Being highly stressed is not a normal state. It causes people psychological difficulties, it detracts them from effective functioning, and it should be regarded as a psychopathological condition that calls for treatment, even if it is common. Indeed, there has recently been a growing interest in studying the manner in which pro- fessional communities of mental health clinicians, policy mak- ers, and researchers should respond to the emerging needs fol- lowing mass trauma (Miller, 2002). In line with the implications of the deviated Rorschach mark- ers of incapacity to minimize distress (D and AdjD) we can also suggest possible implications of the tendency being revealed in the Low Terror Exposure and Lebanon War Exposure samples to exhibit paranoid-like positions (elevated HVI) in interper- sonal relationships. Accordingly, when the real threat of terror decreased, people might have been, as in paranoia, handling their internal fear by projecting it outwards. If so, this could make it easier for them to feel hurt and misunderstood, when this was not intended, feelings that could have clinical and dip- lomatic implications. The results seem to have some important implications con- cerning the validity of the Rorschach and its sensitivity to pick up generalized environmental stressors affecting large groups of people. Studies with other assessment tools have shown that when evaluating the effects of war or terror threat on public mental health, the timing of assessment is crucial and should always be taken into consideration (Silver et al., 2002). In line with these studies our data suggest that the Rorschach is more responsive than previously thought to non-personality contex- tual factors. This conclusion might be viewed as challenging the belief that non-personality variance plays little part or can be fully controlled in interpreting Rorschach data. To a degree, this belief prompted the present study in which the validation procedure is based on independent variables that are lodged in documented facts of terror attacks rather than in inferences. The present data further validate the D Score as the most comprehensive CS marker of experienced distress (Weiner, 1996; Weiner & Greene, 2008), and are in line with previous studies conducted among war veterans with PTSD. The inca- pacity to minimize situation-related distress during a period of increased terror threat, as shown in the present study, might therefore be interpreted as demonstrating the validity of the D Score in picking up more stress at a time when there is good reason to expect there to be more stress. With respect to the lowered AdjD in the High Terror Exposure sample, which al- though not exceeding the normative range differed significantly from to the other samples, a question might be raised as to whether this index is more sensitive than presumed to contex- tual factors. One of the limitations of the present study relates to the in- dependent variable (exposure to terror threat), not taking into consideration other factors that could influence the reported results. Thus, for example, direct exposure to trauma such as childhood abuse might have been responsible for the elevated subjective distress or for the over alertness, rather than the less direct exposure to threat of terrorist attacks and living in a country during a period of war. Nonetheless, there is no reason to assume that these three non-patient samples differed in rela- tion to direct exposure to trauma in the past and the reported period of High Terror Exposure was indeed characterized by severe terror attacks that extremely threatened the daily life of the Israeli citizens (Israeli Ministry of Foreign Affairs, 2008). This limitation is however related to the basic characteristics of any convenient sample and the recruitment procedures, par- ticularly in Rorschach studies that have implications for the generalizability of the results. Another limitation that bears upon generalizability of the re- sults is the small size of the sample that might raise a question as to the extent of which the findings can be generalized. How-  S. TIBON ET AL. 959 ever, a relatively small sample size seems to be the norm in Rorschach research because the administering and scoring pro- cedure can be extremely time consuming and requires special skills of the examiner. The homogeneity of the sample as to age and level of education might also limit the application of the results to other groups of adult non-patients. Further research is needed to substantiate and validate our findings suggesting different dynamic processes in coping with effects of national trauma. Acknowledgements We would like to thank Roni Tibon and Roni Suchowski for programming the Rorschach Reality-Fantasy Scale (RFS) that served for processing the data in this study. We also thank Ba- rak Rand and Ayala Ellis who coordinated and supervised the work on Rorschach data. References Allen, J., & Dana, R. H. (2004). Methodological issues in cross cultural and multicultural Rorschach research. Journal of Personality As- sessment, 82, 189-206. doi:10.1207/s15327752jpa8202_7 Armstrong, J. G., & Loewenstein, R. J. (1990). Characteristics of pa- tients with multiple personality and dissociative disorders on psy- chological testing. Journal of Nervous and Mental Disease, 178, 448-454. doi:10.1097/00005053-199007000-00006 Barenbaum, J., Ruchkin, V., & Schwab-Stone, M. (2004). The psycho- social aspects of children exposed to war: practice and policy initia- tives. Journal of Child Psychology and Psychiatry, 45, 41-62. doi:10.1046/j.0021-9630.2003.00304.x Brand, B. L., Armstrong, J. G., & Loewenstein, R. J. (2006). Psycho- logical assessment of patients with dissociative identity disorder. Psychiatric Clinics of North America, 29, 145-168. doi:10.1016/j.psc.2005.10.014 Brand, B. L., Armstrong, J. G., Loewenstein, R. J., & McNary, S. W. (2009). Personality differences on the Rorschach of dissociative identity disorder, borderline personality disorder, and psychotic inpa- tients. Psychological Trauma: Theory, Research, Practice, and Pol- icy, 1, 188-205. doi:10.1037/a0016561 Carlson, E. B., & Armstrong, J. G. (1994). The diagnostic and assess- ment of dissociative disorders. In S. J. Lynn, & J. W. Rhue (Eds.), Dissociation: Clinical and theoretical perspectives (pp. 159-174). New York: Guilford. Clinton, G., & Jenkins-Monroe, V. (1994). Rorschach responses of sexually abused children: An exploratory study. Journal of Child Sexual Abuse, 3, 67-84. doi:10.1300/J070v03n01_05 Dao, T. K., & Prevatt, F. (2006). Psychometric evaluation of the Ror- schach Comprehensive System’s Perceptual Thinking Index. Journal of Personality Assessment, 86, 180-189. doi:10.1207/s15327752jpa8602_07 Exner, J. E. (l995). A Rorschach workbook for the comprehensive sys- tem (4th ed.). Asheville, NC: Rorschach Workshops. Exner, J. E. (2001). A Rorschach workbook for the comprehensive system (5th ed.). Asheville, NC: Rorschach Workshops. Exner, J. E. (2003). Basic foundations. The Rorschach: A comprehen- sive system, 1 (4th ed.). New York, NY: Wiley. Exner, J. E., & Erdberg, P. (2005). Interpretation. The Rorschach: A comprehensive system, 2 (3rd ed.). New York, NY: Wiley. Exner, J. E., & Weiner, I. B. (2005). Assessment of children and ado- lescents. The Rorschach: A Comprehensive System, 3. (2nd ed.). New York, NY: Wiley. Fonagy, P. (2003). The violence in our schools: What can a psycho- analytically informed approach contribute? Journal of Applied Psy- choanalytic Studies, 2, 223-238. doi:10.1023/A:1022943921048 Fowler, J. C., Pier s, C., Hilsenroth, M. J., Hold wick, D. J., & Padawer, J. R. (2001). The Rorschach suicide constellation: Assessing various degrees of lethality. Journal of Personality Assessment, 76, 333-351. doi:10.1207/S15327752JPA7602_13 Fremont, W. P. (2004). Childhood reactions to terrorism-induced trauma: A review of the past 10 years. Journal of American Academy of Child & Adolescents Psychiatry, 43, 381-392. doi:10.1097/00004583-200404000-00004 Frueh, B. C., Leverett, J. P., & Kinder, B. N. (1995). Interrelationship between MMPI-2 and Rorschach variables in a sample of Vietnam veterans with PTSD. Journal of Personality Assessment, 64, 312- 318. doi:10.1207/s15327752jpa6402_10 Galea, S., Ahern, J., Resnick, H., Kilpatrick, D., Bucuvalas, M., Gold, J., & Vlahov, D. (2002). Psychological sequelae of the September 11 terrorist attacks in New York City. New England Journal of Medi- cine, 346, 982-987. doi:10.1056/NEJMsa013404 Galea, S., & Resnick, H. (2005). Posttraumatic stress disorder in the general population after mass terrorist incidents: considerations about the nature of exposure. CNS Spectrums, 10, 107-115. Gidron, Y. (2002). Posttraumatic stress disorder after terrorist attacks: A review. Journal of Nervous and Mental Disease, 190, 118-121. doi:10.1097/00005053-200202000-00010 Gold, S. N. (2008). The relevance of trauma to general clinical practice. Psychological Trauma: Theory, Research, Practice, and Policy, 5, 114-124. doi:10.1037/1942-9681.S.1.114 Goldfinger, D. A., Amdur, R. L., & Liberzon, I. (1998). Rorschach patterns of response in Vietnam veterans with posttraumatic stress disorder vs. combat and normal controls. Depression and Anxiety, 8, 104-111. doi:10.1002/(SICI)1520-6394(1998)8:3<104::AID-DA2>3.0.CO;2- Y Hartman, W., Clark, N., Morgan, M., Dunn, V., Fine, A., Perry, G., & Winsch, D. (1990). Rorschach structure of hospitalized sample of Vietnam veterans with PTSD. Journal of Personality Assessment, 54, 149-159. doi:10.1207/s15327752jpa5401&2_15 Holaday, M. (2000). Rorschach protocols from children and adoles- cents diagnosed with posttraumatic stress disorder. Journal of Per- sonality Assessment, 75, 143-157. doi:10.1207/S15327752JPA7501_10 Israeli Central Bureau of Statistics (2000). Statistical abstract of Israel, 51, 22. Jerusalem. Israel Ministry of Foreign Affairs (2008). Bombing attacks in Israel since the declaration of principles (September, 1993). MFA Newslet- ter, State of Israel. Jorgensen, K., Andersen T. J., & Dam, H. (2000). The diagnostic effi- ciency of the Rorschach depression index. Assessment, 7, 259-280. doi:10.1177/107319110000700306 Joshi, P. T., & O’Donnell, D. A. (2003). Consequences of child expo- sure to war and terrorism. Clinical Child and Family Psychology Re- view, 6, 275-292. doi:10.1023/B:CCFP.0000006294.88201.68 Kamphuis, J. H., Kugeares, S. L., & Finn, S. E. (2000). Rorschach correlates of sexual abuse: Trauma content and aggression indices. Journal of Personality Assessment, 75, 212-224. doi:10.1207/S15327752JPA7502_3 Kelman, H. C. (2007). The Israeli-Palestinian peace process and its vicissitudes: Insights from attitude theory. American Psychologist, 62, 287-303. doi:10.1037/0003-066X.62.4.287 Leifer, M., Shapir o, J. P., Martone, M. W., & Kassem, L. (1991). Ror- schach assessment of psychological functioning in sexually abused girls. Journal of Personality Assessment, 56, 14-28. doi:10.1207/s15327752jpa5601_2 Leavitt, F., & Labott, S. M. (1998). Rorschach indicators of Dissocia- tive Identity Disorders: Clinical utility and theoretical implications. Journal of Clinical Psychology, 54, 803-810. doi:10.1002/(SICI)1097-4679(199810)54:6<803::AID-JCLP7>3.0.C O;2-H Lerner, P. M. (1998). Psychoanalytic perspectives on the Rorschach. Hillsdale, NJ: The Analytic Press. Levin, P. (1993). Assessing PTSD with the Rorschach assessing tech- nique. In J. Wilson, & B. Raphael (Eds.), The international hand- book of traumatic stress syndrome (pp. 189-200). New York, NY: Plenum Press. doi:10.1007/978-1-4615-2820-3_16 Meyer, G, J., Erdberg, P., & Shaffer, T. W. (2007). Toward interntional normative reference data for the comprehensive system. Journal of Personality Assessment, 89, S201-S220. doi:10.1080/00223890701629342 Miller, L. (2002). Psychological interventions for terroristic trauma:  S. TIBON ET AL. 960 Symptoms, syndromes, and treatment strategies. Psychotherapy: Theory, Research, Practice, Training, 39, 283- 296. doi:10.1037/0033-3204.39.4.283 Nunnally, J. C., & Bernstein, I. H. (1994). Psychometric theory. New York: McGraw Hill. Ogden, T. H. (1989). Playing, dreaming and interpreting experience: Comments on potential space. In M. Fromm, & B. Smith (Eds.), The facilitating environment: Clinical applications of Winnicott’s theory (pp. 255-278). Madison, CT: International Universities Press. Rorschach, H. (1921). Psychodiagnostik. Bern: Bircher. Rubin, G. J., Brewin, C. R., Greenberg, N., Simpson, J., & Wessely, S. (2005). Psychological and behavioral reactions to the bombings in London on July 7, 2005: Cross sectional survey of a representative sample of L o ndo ners. British Medical Journal, 331, 606. doi:10.1136/bmj.38583.728484.3A Sadeh, A., Hen-Gal, S., & Tikotzki, L. (2008). Young children’s reac- tions to war-related stress: A survey and assessment of an innovative intervention. Pediatrics, 121, 46-53. doi:10.1542/peds.2007-1348 Sautter F. J., Brailey K., Uddo M. M., Hamilton M. F., Beard M. G., & Borges A. H. (1999). PTSD and comorbid psychotic disorder: Com- parison with veterans diagnosed with PTSD or psychotic disorder. Journal of Traumatic Stress, 12, 73-78. doi:10.1023/A:1024794232175 Schuster, M. A., Stein, B. D., Jaycox, L. H., Collins, R. L., Marshall, G. N., Elliott, M. N., Zhou, A. J., Kanouse, D. E ., Morrison, J. L., & Berry, S. H. (2001). A national survey of stress reactions after Sep- tember 11, 2001, Terrorist attacks. New England Journal of Medicine, 345, 1507-1512. doi:10.1056/NEJM200111153452024 Schreuder, J. N. (2001). The violation of inner and outer boundaries in political persecution. Journal of Applied Psychoanalytic Studies, 3, 231-242. doi:10.1023/A:1011527500301 Scroppo, J. C., Drob, S. L., Weinberger, J. L., & Eagle, P. (1998). Iden- tifying dissociative identity disorder: A self-report and projective study. Journal of Abnormal Psychology, 107, 272-284. doi:10.1037/0021-843X.107.2.272 Shalev, A. Y. (2000). Measuring outcome in posttraumatic stress dis- order. Journal of Clinical Psychiatry, 61, 33-39. Shalev, A. Y. (2006). Lessons learned from 9/11: The boundaries of a mental health approach to mass casualty events. In Y. Neira, R. Gross, R. Marshall, & E Susser (Eds), 9/11: Mental health in the wake of terrorist attacks (pp. 605-616). Cambridge: Cambridge Uni- versity Press. Shalev, A. Y., Fre edman, S., Pe ri, T., Bran des, D., Sahar, T., Orr, S. P ., & Pitman, R. K. (1998). Prospective study of posttraumatic stress disorder and depression following trauma. American Journal of Psy- chiatry, 155, 630-637. Shaw, J. A. (2003). Children exposed to war/terrorism. Clinical Child and Family Psychology Review, 6, 237-246. doi:10.1023/B:CCFP.0000006291.10180.bd Silver, R. C., Holman, E. A. , McIn tosh, D. N., Po ulin, M., & Gil -Rivas, V. (2002). Nationwide longitudinal study of psychological responses to September 11. Journal of the American Medical Association, 288, 1235-1244. doi:10.1001/jama.288.10.1235 Sloan, P., Arsenault, L., Hilsenroth, M., Handler, L., & Harvill, L. (1996). Rorschach measures of posttraumatic stress in Persian Gulf War veterans: A three-year follow-up study. Journal of Personality Assessment, 66, 55- 64. doi:10.1207/s15327752jpa6601_4 Smith, B. (1990). Potential space and the Rorschach: Application of object relations theory. Journal of Personality Assessment, 55, 756-767. Smith, S. R., Chang, J., Kochinski, S., Patz, S., & Nowinski, L. A. (2010). Initial validity of the logical Rorschach in the assessment of trauma. Journal of Personality Assessment, 92, 222-231. doi:10.1080/00223891003670174 Steinberg, M. (1996). Assessment of dissociation in trauma survivors and PTSD. Assessing Psychological trauma and PTSD: A handbook for practitioners. New York: Guilford Press. Swanson, G. S., Blount, J., & Bruno, R. (1990). Comprehensive system Rorschach data of Vietnam combat veterans. Journal of Personality Assessment, 54, 160-169. doi:10.1207/s15327752jpa5401&2_16 Tibon, S. (2005). On potential space in psychosomatics and psychosis: A Rorschach study. Journal of the American Psychoanalytic Association, 53, 1296-1298. Tibon, S. (2007). Rorschach comprehensive system data for a sample of 41 adult non-patients from Israel. Journal of Personality Assessment, 89, S74-S79. doi:10.1080/00223890701583218 Tibon, S., Handelzalts, J. E., & Weinberger, Y. (2005). Using the Ror- schach for exploring the concept of transitional space within the po- litical context of the Middle East. International Journal of Applied Psychoanalytic Studies, 2, 40-57. doi:10.1002/aps.30 Tibon, S., Weinberger, Y., Handelzalts, J., & Porcelli, P. (2005). Con- struct validation of the Rorschach Reality-Fantasy Scale in Alexithymia. Psychoanalytic Psychology, 22, 508-523. doi:10.1037/0736-9735.22.4.508 Torabi, M. R., & Seo, D. C. (2004). National study of behavioral and life changes since September 11. Health Education Behavior, 31, 179-192. doi:10.1177/1090198103259183 Twemlow, S. W. (2004). Psychoanalytic understanding of terrorism and massive social trauma. Journal of the American Psychoanalytic Association, 52, 709-716. Twemelow, S. W., & Sacco, F. C. (2002). Reflections on the making of a terrorist. In C. Covington, P. Williams, J. Arundale, & J. Knox (Eds.), Terrorism and political violence (pp. 97-123). London: Kar- nac. Viglione, D. J. (1990). Severe disturbance or trauma-induced adaptive reaction: A Rorschach child case study. Journal of Personality As- sessment, 55, 280-295. doi:10.1207/s15327752jpa5501&2_27 Viglione, D. J., & Meyer, G. J. (2008). An overview of Rorschach psychometrics for forensic practice. In C. B. Gacono, & B. Evans (Eds.), The handbook of Rorschach forensic assessment (pp. 21-52). New York: Rutledge. Weiner, I. B. (1996). Some observations on the validity of the Ror- schach Inkblot Method. Psychological Assessment, 8, 206-213. doi:10.1037/1040-3590.8.2.206 Weiner, I. B. (2001). Advancing the science of psychological assess- ment: The Rorschach Inkblot Method as exemplar. Psychological As- sessment, 13, 423-432. doi:10.1037/1040-3590.13.4.423 Weiner, I. B. (2003). Principles of Rorschach Interpretation. Hillsdale, NJ: Lawrence Erlbaum. Weiner, I. B., & Greene, R. L. (2008). Handbook of personality as- sessment. New York, NY: Wiley. Wilson, J. P., & Keane, T. M. (1997). Assessing psychological trauma and PTSD. New York, NY: Guilford Press. Winnicott, D. W. (1971). Playing and reality. New York, NY: Basic Books. Zeligman, R., Smith, B. L., & Tibon, S. (2011). The failure to preserve potential space in dissociative disorders: A Rorschach study. Psy- choanalytic Psychology, 22, 508-523.
|