T. H. Zhu et al. / Health 3 (2011) 689-697
Copyright © 2011 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/
691691
Health Institutional Review Board to undertake this
study was obtained in April 2008.
2.4. Definitions
Helmet use was defined as a child wearing a helmet
“always” or “most of the time” while riding, and non-
use was defined as when the child “did not wear” or
wore a helmet “some of the time” while riding the ve-
hicle [9].
The definitions for head and facial injuries followed
closely to those of Thompson et al. [10] and were
phrased understandable to the caregivers. A head injury
was defined as consisting of superficial cuts/scrapes
(lacerations/abrasions), bruises on the scalp, bumps to
the head and passing out (possible concussion) and bro-
ken bones in the head (skull fractures). A facial injury
for all areas consisted of superficial cuts/scrapes, and
bruises to the face, including the forehead, eye (external),
nose, mouth (intra-oral), cheek, ear (external), chin (lower
jaw), and facial bone fractures. The upper and mid-por-
tion of face was taken as occurring to the forehead, eye,
nose, cheek or ear.
2.5. Data Sources and Measurement
2.5.1. Helmet Use Study Component
The nurses provided a simple, self-administered, pre-
tested, and structured questionnaire to the caregivers to
record helmet use in HE and E groups at the beginning
(1st Survey) and end of study (2nd Survey). H’E was
identified after the 1st Survey. The questionnaire con-
tained data on the caregivers including highest education
attained, ethnicity, and language spoken. The data gath-
ered on the children included sex, type of vehicle pos-
sessed, helmet ownership, and the numbers of helmet
use while riding the vehicle. To supplement the helmet
use by questionnaire method, the nurse used observation
method by asking the caregiver during the home visit
(see below) to let the child ride the bicycle or other rid-
ing vehicle, and observed whether the child rode and
wore a helmet with or without prompting in the HE
group as was done in one study [11].
2.5.2. Injury Study Component
Another simple, self-administered, pretested, and
structured questionnaire was also given to the caregivers
for recording demographic information of both caregiv-
ers and children, and injuries that occurred during the
follow-up. The variables for each injury included,
among others, the date of injury, helmet wearing status,
nature of injury, anatomic location of injury, and type of
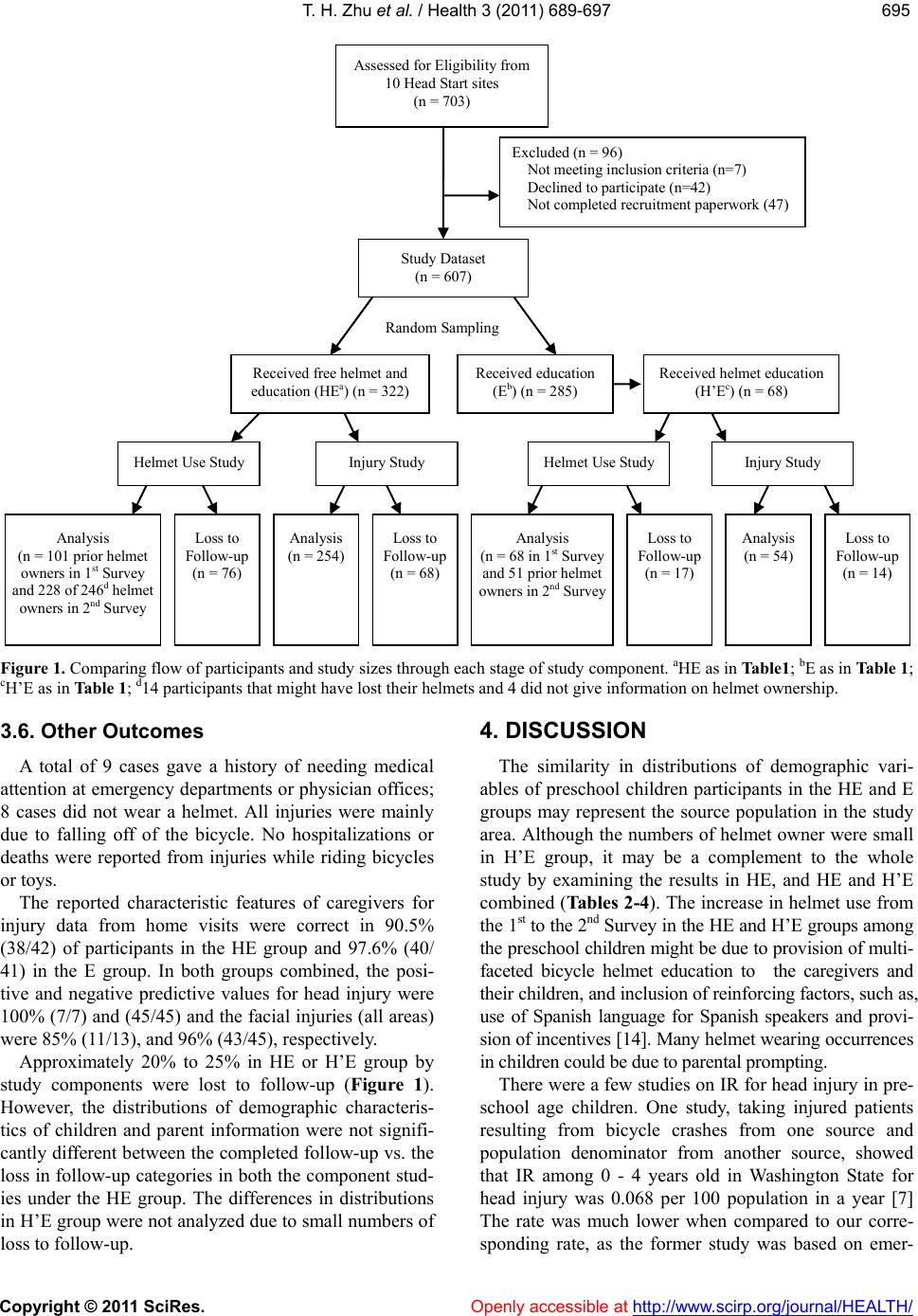
treatment sought. In addition, a systematic random sam-
ple of 20% of families by site from the HE and E groups
were selected to use as a validation subsample of study
subjects to carry out a one-time home visit by the field
team members. It began 4 weeks after the recruitment
for determining any discrepancies on recording injuries
and to verify injury location diagnoses.
All questionnaires were collected at the Head Start
sites, by US mail services, and at home visits. Telephone
calls were periodically made to increase the response
rate.
2.6. Statistical Analysis
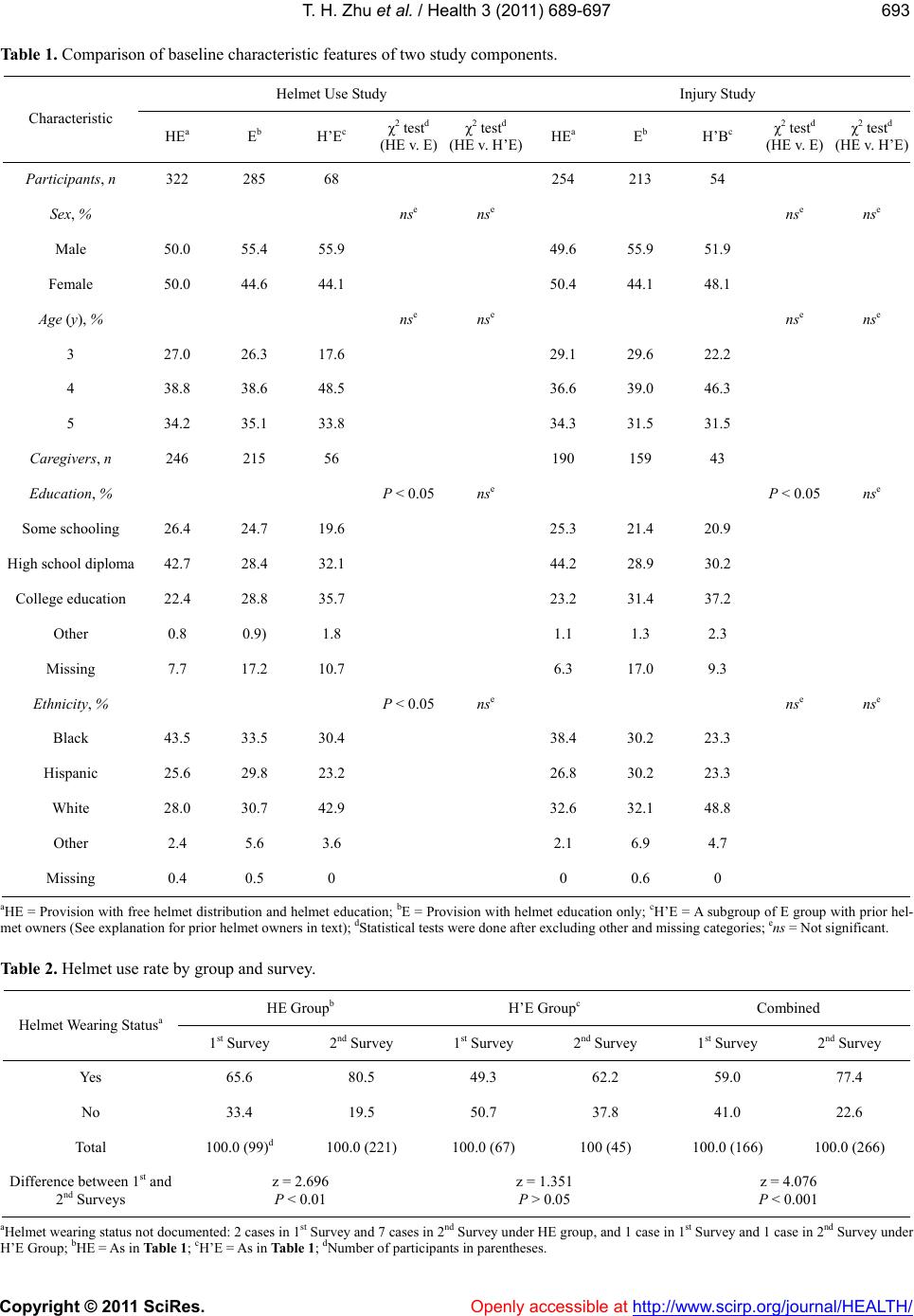
Helmet uses among helmet owners were analyzed by
HE and H’E groups and Survey. Statistical tests were
performed using 2-tail P value <0.05 as statistical sig-
nificance [12].
A child possessing a helmet could have multiple epi-
sodes of bodily injuries including head and/or face from
falls while riding, switching helmet wearing to non-
wearing and vice versa, during the following-up period.
Based on this context, assignment of person-time (per-
son-days) contributing to an injury including the head
and face within a child was determined as the period of
exposure up to the moment of that injury event while
riding by wearing a helmet or period of non-exposure
without wearing a helmet. In other words, a child could
have a number of exposure and non-exposure person-
days depending upon helmet wearing status at the time
of injury event while riding. Those children without re-
porting any injuries and therefore unable to know their
helmet wearing experience were excluded from the per-
son time determination. Based on these assumptions, the
person-days for incidence rates (IRs) were computed
from the participants’ start and end dates of follow-up
and the dates of injuries as follows:
1) For a child, either with one or more injury events,
wearing or not wearing a helmet at one or all injury
dates, person-days = End Date – Start Date.
2) For a child with 2 or more events, person-days for
the 1st or with the same continuously wearing or not
wearing occurring events = Injury Date (of 1st or that of
last continuous event) – Start Date. For subsequent dif-
fering wearing event (s), person-days = Injury Date (of
that or last event] – Injury Date (of previous event) and
were repeated if such alternate (s) of wearing/non-
wearing continued to occur. But the person-days for the
final injury event = End Date – Last Counted Injury
Date so that the child total person-days were completely
distributed by helmet wearing status.
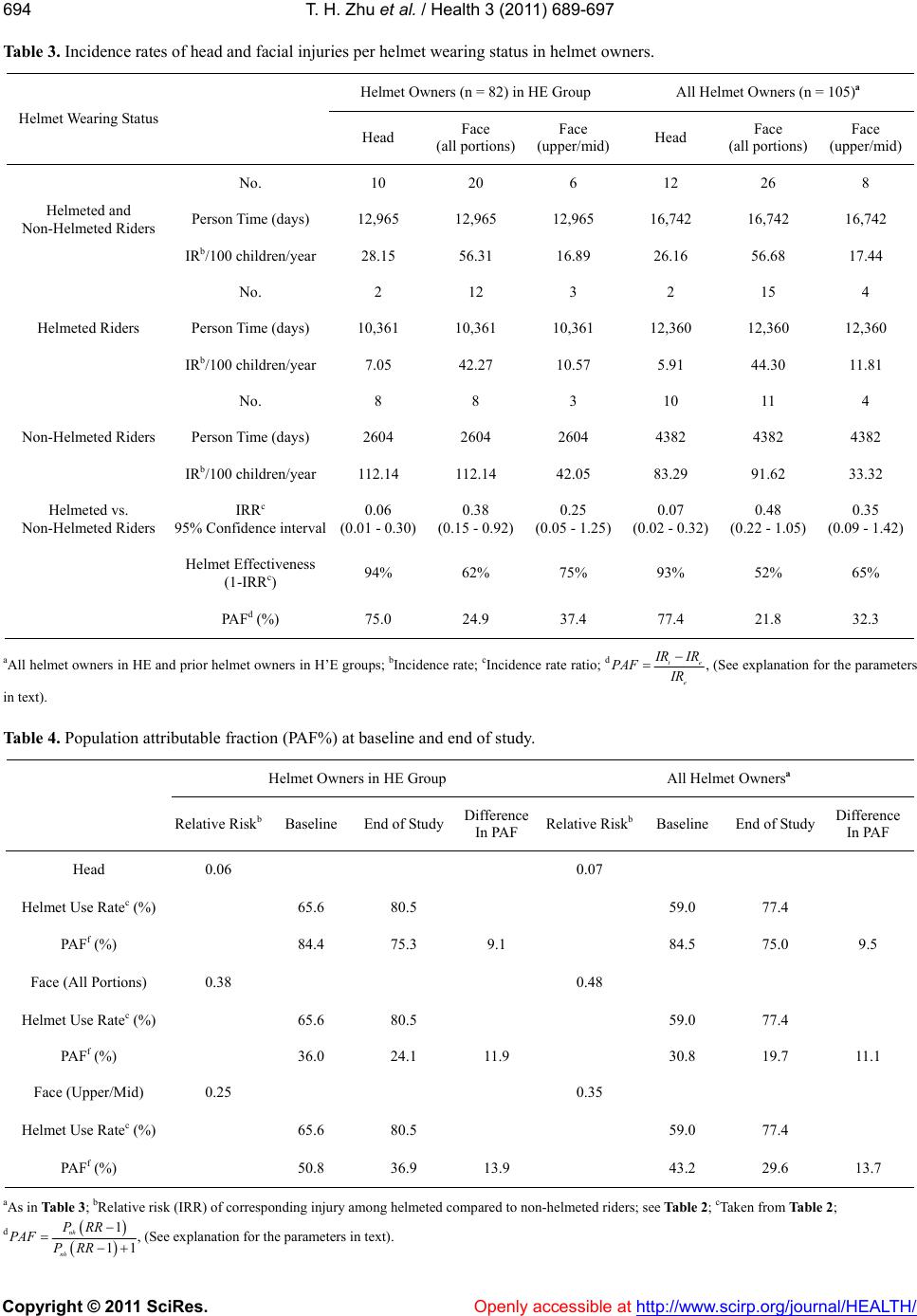
The sum of helmeted or non-helmeted person-days
was taken as the denominator for respective IR. Inci-
dence rate ratios (IRRs) along with 95% CI values were
calculated and the values of helmet effectiveness [13] in
this preschool age were derived. PAFs for head and fa-