S. SHIN ET AL. 9
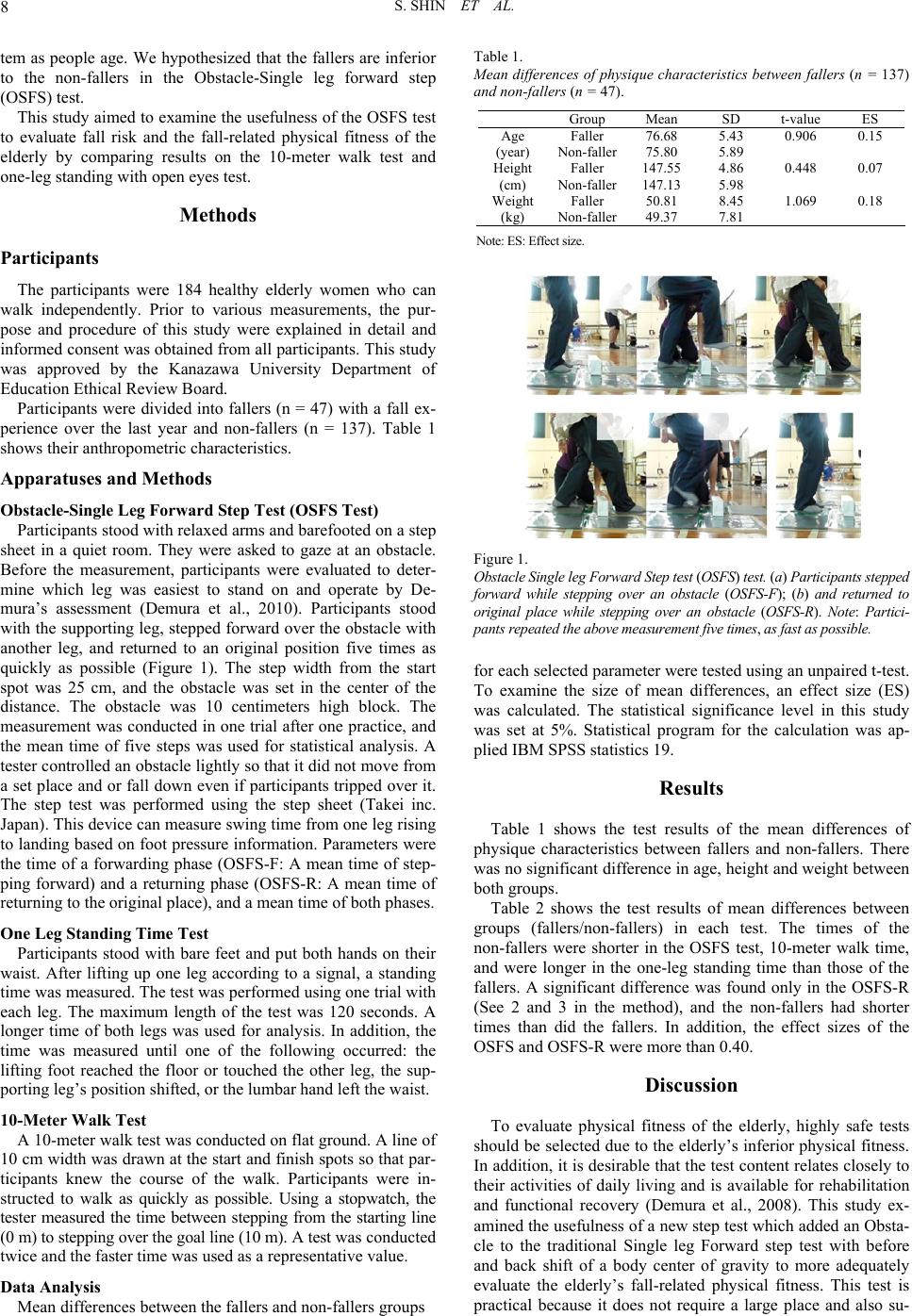
Table 2.
Mean differences between Fallers (n = 47) a nd No n-fallers (n = 137) in each test.
Group Mean SD t-value ES
Faller 0.64 0.16
OSFS (sec.) Non-faller 0.59 0.13 2.254 0.40
Faller 0.60 0.16
OSFS-F (sec.) Non-faller 0.58 0.15 0.929 0.16
Faller 0.67 0.18
OSFS-R (sec.) Non-faller 0.60 0.15 2.596 0.46
Faller 6.93 1.24
10-meter walk
time (sec.) Non-faller 6.48 1.31 2.013 0.35
Faller 20.37 28.18
One leg standing
time with eye open
(sec.) Non-faller 32.77 34.68 2.213 0.35
Note―OSFS: Obstacle Single leg Forward Step; ES: Effect size; OSFS(F): Forward phase; OSFS(R): Returning phase.
perior in safety because it involves simple movement that even
the elderly can understand easily.
Fallers were inferior in the OSFS (Obstacle single leg for-
ward step) test to non-fallers. The 10-meter walk time and
one-leg standing time with eyes open also showed similar re-
sults. Mano reported the following: a cause of walking speed
decline depends on shortening of a stride length and a decrease
of pace, and the former attributes this to slight bending of the
knees, a small flexion angle of hip joints, and a small dorsi-
flexion angle of ankles when heels contact the ground. It is a
so-called “shuffle” (a senile walk) (Mano, 2008). Both single
and double stance phases become longer, and kicking out pow-
er also decreases with a leg strength decrease. According to
physiological studies (Vandervoot and Hays, 1989; Era and
Heikkinen, 1985; Gottasdanker, 1982), a cause of falls among
the elderly is a decrease in consciousness-motor system func-
tion which contributes to posture and balance maintenance
during walking in old age. Hence, a decline in physical fitness
factors such as walk ability, balance ability etc. is also consid-
ered to be important in screening the elderly’s fall risk.
The OSFS test as well as the 10-meter walk and one-leg
standing time tests showed that the fallers are inferior to the
non-fallers. In this connection, the former effect size was equal
or somewhat larger than the two later ones. The OSFS test was
constructed by considering the following four standpoints; 1.
When almost falling, the elderly step forward to one step to
keep their base of support (BOS) and prevent fall. 2. A decrease
in leg strength and balance ability as well as the range of mo-
tion (ROM) of the hip, knee and ankle joints are connected with
factors related to fall. 3. The elderly fall frequently by tripping
over an obstacle or a step. 4. The test for screening should use
movements which the elderly can easily understand. Because
the OSFS test demands that the elderly step over the obstacle
while supporting the body with one leg and then return to the
stepped leg’s original position again, it may be difficult for
them with decreased physical fitness as compared with the
movements of walking and one-leg standing.
A significant difference was found in the OSFS-R between
fallers and non-fallers but not in the OSFS-F. Therefore, a fall
risk may be better explained by the movement (OSFS-R) in
returning the stepped leg to the original place than the move-
ment in stepping over an obstacle (OSFS-F). Because of de-
creased leg strength or the fear that one may fall forward, the
elderly cannot stretch their legs sufficiently when their body is
inclined forward (Ryushi, 2008). The movement that is required
when the elderly step forward and return to an original position
again exerts more force on the supporting leg in addition to
maintaining balance. Hence, the elderly with decreased leg
strength, balance ability, and ROM of leg joints may difficulty
in achieving it successfully.
Mano (2008) reported that the elderly’s shuffle contributes to
maintaining balance during walking because a single-leg sup-
port time becomes shorter according to posture changes, and
instability during direction change with age is due to a decline
in sensory function and a delay in central response time. As
confirmed in the movement used in this study and the previous
study, the elderly’s shuffle or senile walk may be a compensa-
tory locomotor way to transfer to the next movement smoothly.
Conclusions
In conclusion, the OSFS test can discriminate between the
fallers and non-fallers as well as 10meter walk time and one-leg
standing time tests. Hence, it may be effective to evaluate the
elderly’s fall-related physical fitness. Additionally, the OSFS-R
may be a better evaluation tool than the OSFS-F.
References
Aoyagi, Y., Togo, F., Furuna, T., Nishizawa, S., Sugiura, M., Sugita, S.,
Matsuki, S., Kumazaki, Y., Naka, M., Inoue, S., Takamiya, T., Ono,
F., Uchida, Y., & Inokuchi, C. (2001). Research-aid report: Devel-
opment of a new method for determining exercise intensity based on
the walking velocity of the elderly. Tokyo: Meiji Yasuda Life foun-
dation of Health and Welfare. (in Japanese)
Demura, S., Sato, S., & Sugiura, H. (2010). Lower limb laterality char-
acteristics based on the relationship between activities and individual
laterality. Gazzeta Medica Italiana, 169, 181-191.
Demura, S., Shin, S., & Yamaji, S. (2008). Sex and age differences of
relationships among stepping parameters for evaluating dynamic ba-
lance in the elderly. Journal of Physiological Anthropology, 27, 207-
215. doi:10.2114/jpa2.27.207
Era, P., & Heikkinen, E. (1985). Postural sway during standing and
unexpected disturbance of balance in random samples of men of dif-
ferent ages. The Journals of Gerontolog y, 40, 287-295.
Gottasdanker, R. (1982). Age and simple RT. The Journals of Geron-
tology, 37, 342-348.
Hosoda, T. (2001). Handbook of physical therapy (2nd ed.). Tokyo:
Kyodoisyo Press. (in Japanese).
Hsiao-Wecksler, E. T. (2007). Assessing quiet and perturbed balance:
A review. Japanese Journal of Biomechanics in Sports and Exercise,
11, 291-302.
Mano, Y. (2008). Falls in the elderly and measurements. Tokyo: Ishi-
yaku Press. (in Japanese).
Rogers, M., Hedman, L. D., Johnson, M. E., Cain, T. D., & Hanke, T.
A. (2001). Lateral stability during forward-induced stepping for dy-
namic balance recovery in young and older adults. Journal of Ger-