A. HEGELE ET AL.
84
testicle is significantly more existent in spermatic cord
torsion compared to other painful entities causing acute
scrotum. Additionally, patients with spermatic cord tor-
sion haunted hospital significantly faster. Other clinical
signs like reddening and swelling seem not to be suffi-
ciently reliable. Our clinical predictors associated with
higher likelihood of spermatic cord torsion are in line
with others [3,9,10,11]. These authors described also that
high position of testicle and short time duration until
haunting hospital are associated with existence of sper-
matic cord torsion.
Our data underline the impact of duplex sonography in
this emergency situation and in the diagnostic workup of
acute scrotum [1,12,13]. In our large cohort we found
significant reduction or loss of testicular perfusion in
spermatic cord torsion. However, the performance and
interpretation are operator-dependent and are supported
by history and physical findings thus in clinical unclear
cases surgical exploration is still indicated [14]. Some
authors described a seasonal variation of spermatic cord
torsion incidence. Lyronis and co-workers described a
significant increased appearance of spermatic cord tor-
sion during greek winter in 140 boys [15]. Srinivasan
and co-workers found, using multivariate analysis, a sig-
nificant correlation between spermatic cord torsion and
decreasing atmospheric temperature in 58 US children
[16]. Malakindiah and co-workers described an increased
occurrence from October to March in India [17]. Wil-
liams and co-workers did not see statistical relevant dif-
ferences between the different seasons but they also de-
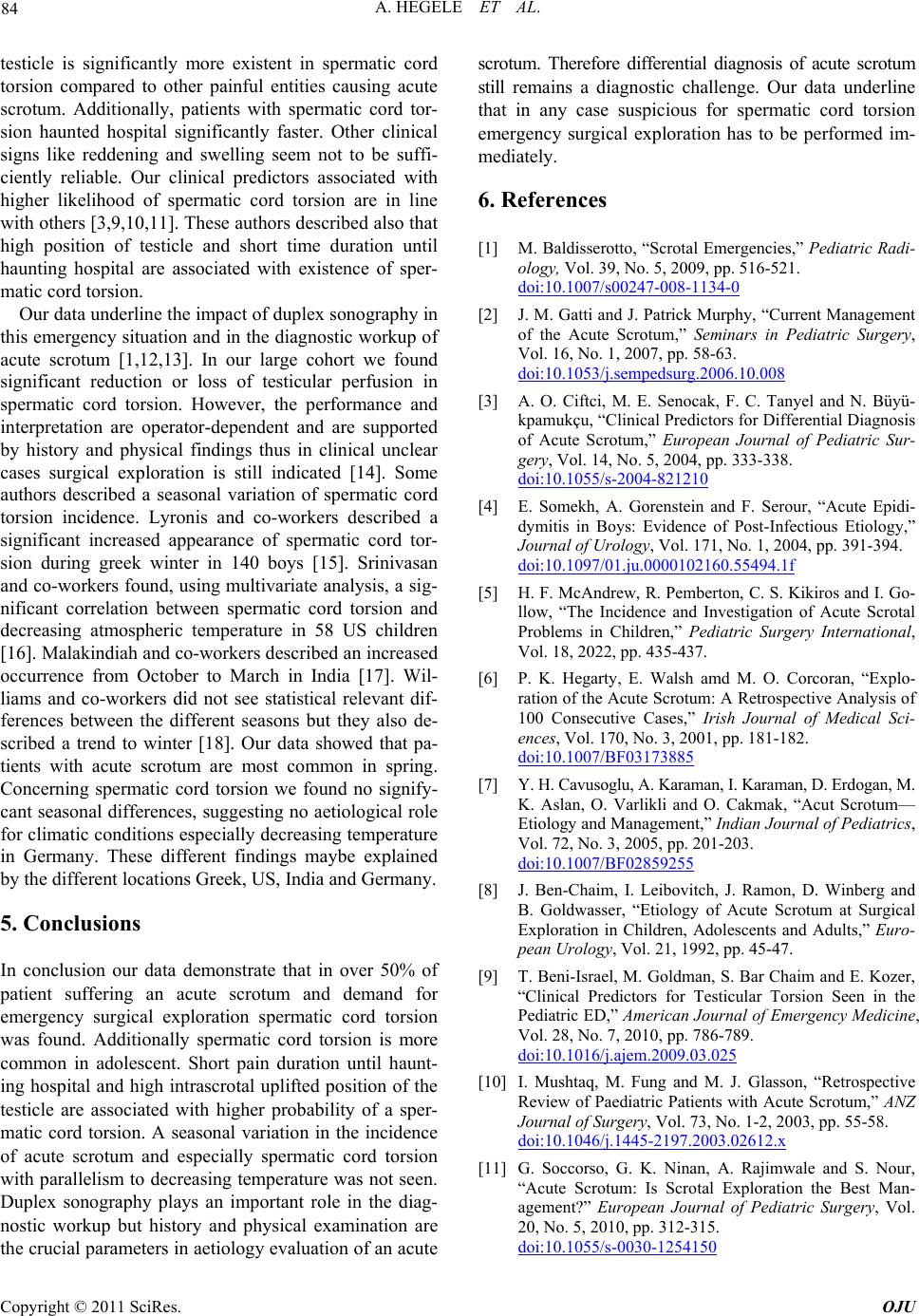
scribed a trend to winter [18]. Our data showed that pa-
tients with acute scrotum are most common in spring.
Concerning spermatic cord torsion we found no signify-
cant seasonal differences, suggesting no aetiological role
for climatic conditions especially decreasing te mperature
in Germany. These different findings maybe explained
by the different locations Greek, US, India and Germany.
5. Conclusions
In conclusion our data demonstrate that in over 50% of
patient suffering an acute scrotum and demand for
emergency surgical exploration spermatic cord torsion
was found. Additionally spermatic cord torsion is more
common in adolescent. Short pain duration until haunt-
ing hospital and high intrascrotal uplifted position of the
testicle are associated with higher probability of a sper-
matic cord torsion. A seasonal variation in the incidence
of acute scrotum and especially spermatic cord torsion
with parallelism to d ecreasing temperature was not seen.
Duplex sonography plays an important role in the diag-
nostic workup but history and physical examination are
the crucial parameters in aetio logy evaluation of an acu te
scrotum. Therefore differential diagnosis of acute scrotum
still remains a diagnostic challenge. Our data underline
that in any case suspicious for spermatic cord torsion
emergency surgical exploration has to be performed im-
mediately.
6. References
[1] M. Baldisserotto, “Scrotal Eme rgencies,” Pediatric Radi-
ology, Vol. 39, No. 5, 2009, pp. 516-521.
doi:10.1007/s00247-008-1134-0
[2] J. M. Gatti and J. Patrick Murphy, “Current Management
of the Acute Scrotum,” Seminars in Pediatric Surgery,
Vol. 16, No. 1, 2007, pp. 58-63.
doi:10.1053/j.sempedsurg.2006.10.008
[3] A. O. Ciftci, M. E. Senocak, F. C. Tanyel and N. Büyü-
kpamukçu, “Clinical Predictors for Differential Diagnosis
of Acute Scrotum,” European Journal of Pediatric Sur-
gery, Vol. 14, No. 5, 2004, pp. 333-338.
doi:10.1055/s-2004-821210
[4] E. Somekh, A. Gorenstein and F. Serour, “Acute Epidi-
dymitis in Boys: Evidence of Post-Infectious Etiology,”
Journal of Urology, Vol. 171, No. 1, 2004, pp. 391-394.
doi:10.1097/01.ju.0000102160.55494.1f
[5] H. F. McAndrew, R. Pemberton, C. S. Kikiros and I. Go-
llow, “The Incidence and Investigation of Acute Scrotal
Problems in Children,” Pediatric Surgery International,
Vol. 18, 2022, pp. 435-437.
[6] P. K. Hegarty, E. Walsh amd M. O. Corcoran, “Explo-
ration of the Acute Scrotum: A Retrospective Analysis of
100 Consecutive Cases,” Irish Journal of Medical Sci-
ences, Vol. 170, No. 3, 2001, pp. 181-182.
doi:10.1007/BF03173885
[7] Y. H. Cavusoglu, A. Karaman, I. Karaman, D. Erdogan, M.
K. Aslan, O. Varlikli and O. Cakmak, “Acut Scrotum—
Etiology and Management,” Indian Journal of Pediatrics,
Vol. 72, No. 3, 2005, pp. 201-203.
doi:10.1007/BF02859255
[8] J. Ben-Chaim, I. Leibovitch, J. Ramon, D. Winberg and
B. Goldwasser, “Etiology of Acute Scrotum at Surgical
Exploration in Children, Adolescents and Adults,” Euro-
pean Urology, Vol. 21, 1992, pp. 45-47.
[9] T. Beni-Israel, M. Goldman, S. Bar Chaim and E. Kozer,
“Clinical Predictors for Testicular Torsion Seen in the
Pediatric ED,” American Journal of Emergency Medicine,
Vol. 28, No. 7, 2010, pp. 786-789.
doi:10.1016/j.ajem.2009.03.025
[10] I. Mushtaq, M. Fung and M. J. Glasson, “Retrospective
Review of Paediatric Patients with Acute Scrotum,” ANZ
Journal of Surgery, Vol. 73, No. 1-2, 2003, pp. 55-58.
doi:10.1046/j.1445-2197.2003.02612.x
[11] G. Soccorso, G. K. Ninan, A. Rajimwale and S. Nour,
“Acute Scrotum: Is Scrotal Exploration the Best Man-
agement?” European Journal of Pediatric Surgery, Vol.
20, No. 5, 2010, pp. 312-315.
doi:10.1055/s-0030-1254150
Copyright © 2011 SciRes. OJU