79
G.-Y. DENG ET AL.
4. Discussion
UPJO is common in children, for which Anderson–Hynes
pyeloplasty is the classic surgical treatment [5,6] < B1
B2 > < /C< B3 B4 > <, and there have been some reports
concerning about UTI in patients with UPJO [1,2].
Unlike previous studies, in the present study, urine taken
directly from the renal pelvis was cultured. The risk fac-
tors for developing bacteriuria or funguria were also
been determined by Logistic test.
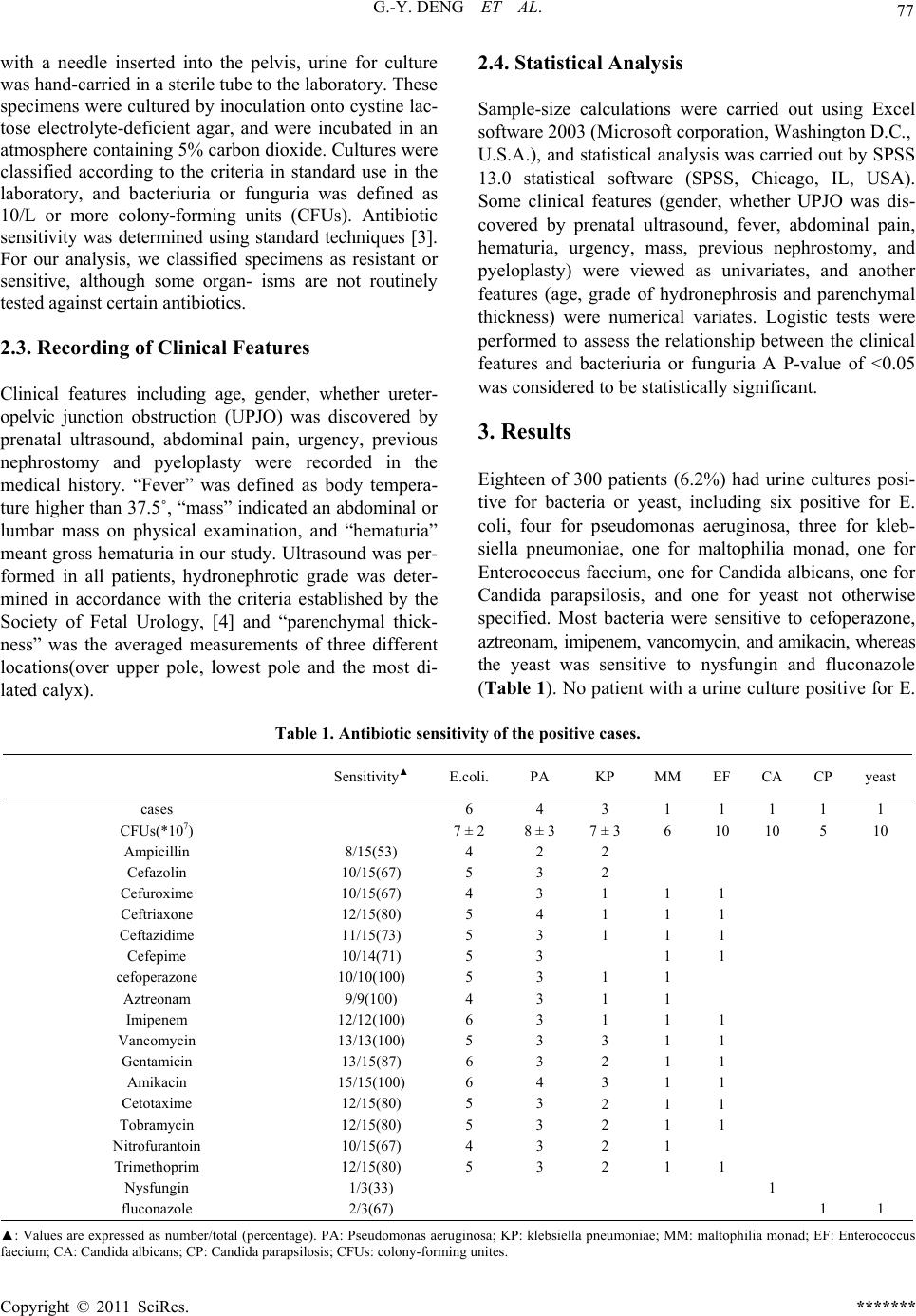
As has been described in previous reports, [8] our
study found that E. coli, pseudomonas aeruginosa, and
klebsiella pneumoniae were the most common organisms
cultured from urine. No patient with a urine culture posi-
tive for E. coli had a history of nephrostomy or pye-
loplasty, unlike patients with urine cultures positive for
other organisms. No previous study has reported this. As
has been reported previously, urinary tract abnormalities
increase the incidence of bacteriuria or funguria [7]. Be-
cause E. coli has better adhesive and migratory capabili-
ties, translocation to the renal pelvis is more likely for this
organism, even in patients with no history of nephrostomy
or pyeloplasty. Our study also found that most bacteria
were sensitive for cefoperazone, aztreonam, imipenem,
vancomycin, and amikacin; however, the conclusion was
less persuasive, because some patients had received pro-
phylactic antibacterial agents.
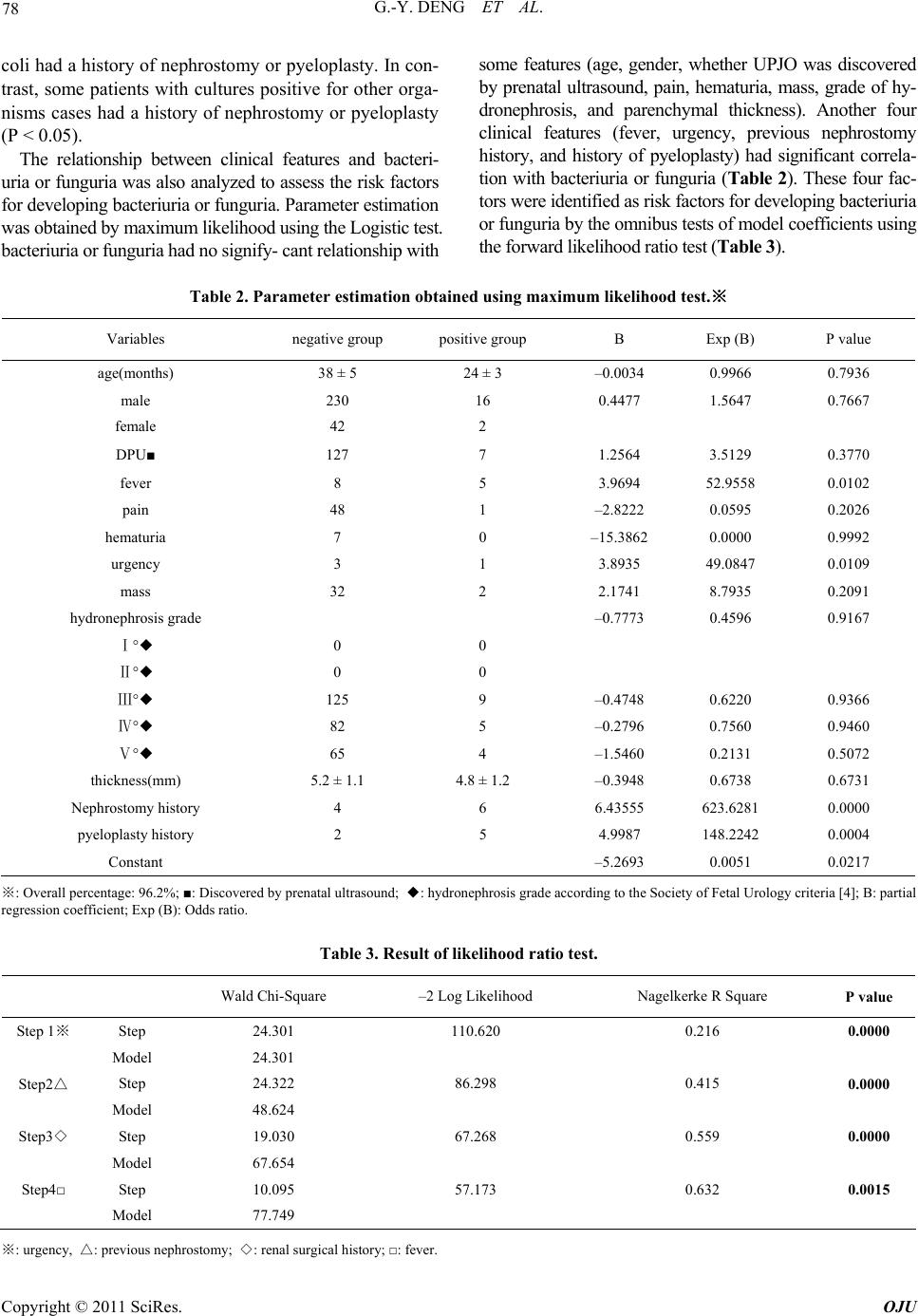
There has been no study of the relationship between
age or gender and bacteriuria or funguria in patients with
UPJO. Our study found that there was no significant re-
lationship between age or gender and bacteriuria or fun-
guria, perhaps because boys were more likely develop
UPJO, [5,6] whereas girls were much more likely to de-
velop a UTI after 1 year [9]. Increasingly, UPJO is dis-
covered by prenatal ultrasound [6], but being diagnosed
by prenatal ultrasound was not a risk factor to develop
bacteriuria or funguria. In addition, hydronephrosis [5],
abdominal pain, hematuria, and mass were not risk fac-
tors.
As has been discussed in some studies [1], the degree
of hydronephrosis was not a risk factor for developing
bacteriuria or funguria in our study. No previous study
has reported a relationship between parenchymal thick-
ness and bacteriuria or funguria. We found that paren-
chymal thickness was not a risk factor, although, deterio-
ration in renal function was associated with exacerbation
of hydronephrosis and decrease in parenchymal thickness
in some patients [5,6]. Prophylactic antibacterial agents
were probably necessary in those patients who had signs
of urinary tract infection (UTI), or history of nephrostomy
or pyeloplasty.
This retrospective study has some limitations. Firstly,
prophylactic antibacterial agents had been administrated
to those patients who had a nephrostomy catheter or had
signs/symptoms of UTI (fever and urgency) prior to the
operation. Some patients with negative urine cultures had
had signs/symptoms of UTI (Table 2). Thus, some im-
portant information might have been lost [2]. In addition,
one of the main important factors responsible for resis-
tance or sensitivity of uropathogens is antibiotic pre-
treatment and the use of prophylactic antibacterial agents
[10]. In this study, five patients (27%) in the bacteri-
uria/funguria group and eight patients (2.9%) in the cul-
ture-negative group had received antibiotics before the
urine was cultured. The antibiotic sensitivity results were
less reliable when urine culture was not performed prior
to administration of prophylactic antibacterial agents,
This issue is a topic for future.
5. Conclusions
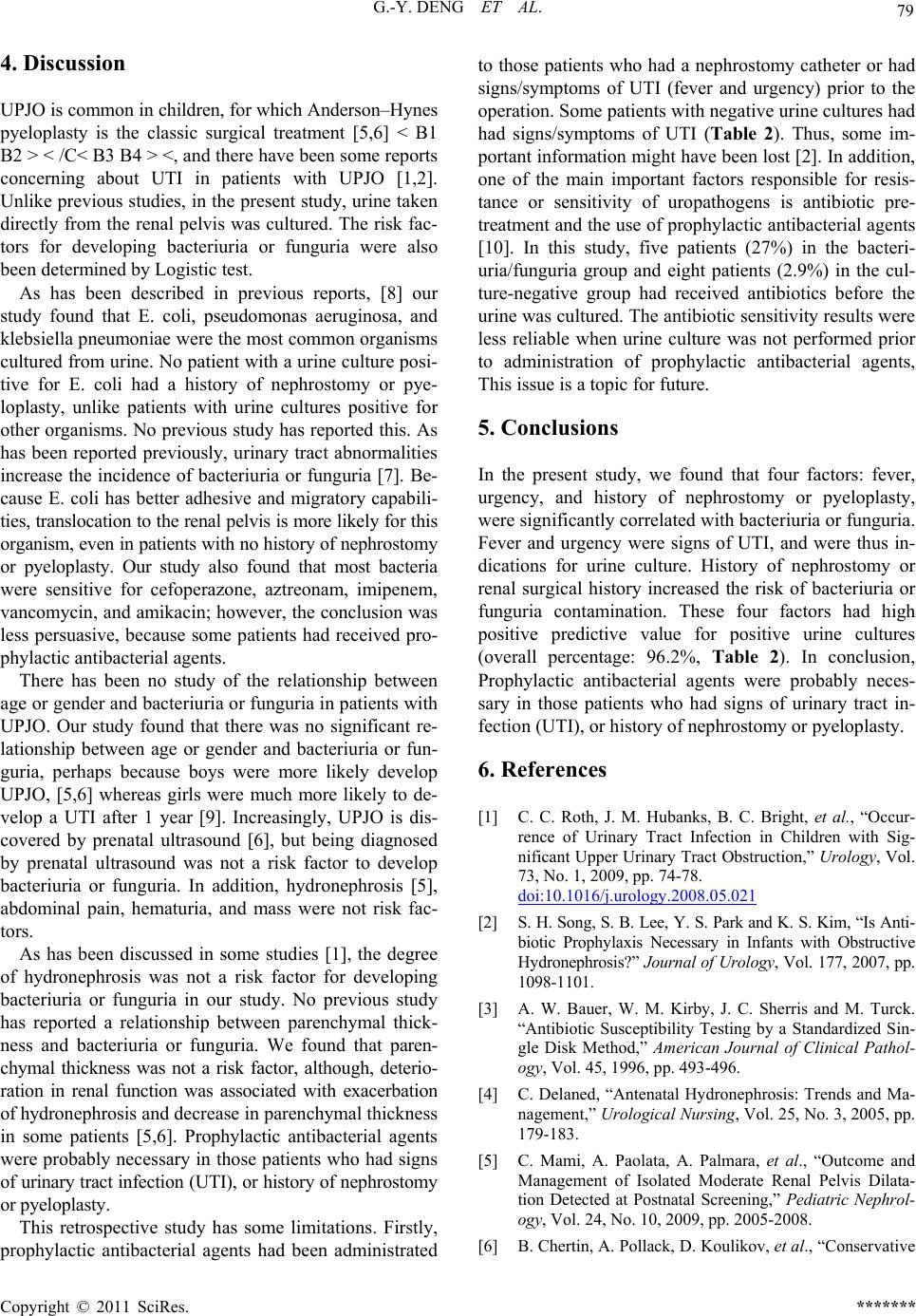
In the present study, we found that four factors: fever,
urgency, and history of nephrostomy or pyeloplasty,
were significantly correlated with bacteriuria or funguria.
Fever and urgency were signs of UTI, and were thus in-
dications for urine culture. History of nephrostomy or
renal surgical history increased the risk of bacteriuria or
funguria contamination. These four factors had high
positive predictive value for positive urine cultures
(overall percentage: 96.2%, Table 2). In conclusion,
Prophylactic antibacterial agents were probably neces-
sary in those patients who had signs of urinary tract in-
fection (UTI), or history of nephrostomy or pyeloplasty.
6. References
[1] C. C. Roth, J. M. Hubanks, B. C. Bright, et al., “Occur-
rence of Urinary Tract Infection in Children with Sig-
nificant Upper Urinary Tract Obstruction,” Urology, Vol.
73, No. 1, 2009, pp. 74-78.
doi:10.1016/j.urology.2008.05.021
[2] S. H. Song, S. B. Lee, Y. S. Park and K. S. Kim, “Is Anti-
biotic Prophylaxis Necessary in Infants with Obstructive
Hydronephrosis?” Journal of Urology, Vol. 177, 2007, pp.
1098-1101.
[3] A. W. Bauer, W. M. Kirby, J. C. Sherris and M. Turck.
“Antibiotic Susceptibility Testing by a Standardized Sin-
gle Disk Method,” American Journal of Clinical Pathol-
ogy, Vol. 45, 1996, pp. 493-496.
[4] C. Delaned, “Antenatal Hydronephrosis: Trends and Ma-
nagement,” Urological Nursing, Vol. 25, No. 3, 2005, pp.
179-183.
[5] C. Mami, A. Paolata, A. Palmara, et al., “Outcome and
Management of Isolated Moderate Renal Pelvis Dilata-
tion Detected at Postnatal Screening,” Pediatric Nephrol-
ogy, Vol. 24, No. 10, 2009, pp. 2005-2008.
[6] B. Chertin, A. Pollack, D. Koulikov, et al., “Conservative
Copyright © 2011 SciRes. *******