Health
Vol. 5 No. 7 (2013) , Article ID: 35096 , 9 pages DOI:10.4236/health.2013.57153
Family and women decide child nutrition—The role of human development, capabilities and lifestyles
![]()
Latin American Faculty of Social Sciences, Facultad Latinoamericana de Ciencias Sociales (FLACSO), Mexico; cristinagomesmx@gmail.com
Copyright © 2013 Cristina Gomes. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received 23 April 2013; revised 26 May 2013; accepted 15 June 2013
Keywords: Mal Nourishment; Children; Women; Family; Lifestyles
ABSTRACT
In this article, capacities and freedom approach, as well as lifestyles are explored taking into account child nutrition, and other relevant dimensions of human life more than just economic and other elementary resources, and also social, cultural, psychological, values and freedom dimensions. Nourishment, health and survival are considered some of the elementary capabilities, and the concept of malnutrition, including under and over-nutrition, is discussed, based upon the comparison of data on food production and distribution from the macro level context, as well as from the family and individual levels included anthropometrical measurements. The advantages and limits of different kinds of measurements are discussed, suggesting more complex approaches, based also upon family and gender equality. The double burden of malnutrition, under and overnourishment of children is highlighted as a public health issue to be resolved by adequate policies and considering the role of female empowerment, nutrition-knowledge and education as relevant keys to achieve equality in family food and resource distribution, healthy lifestyles and human development.
1. INTRODUCTION
Nutrition is an elementary dimension of quality of life, which can be analysed from three different conceptual approaches. According to Stiglitz, Sen and Fitoussi [1], the psychological subjective approach considers that individuals are the best judges of their own conditions as to how satisfied they are with their lives; the welfare economics approach uses the notions of willingness and individual preferences to weight goods, services and nonmonetary dimensions in defining wellbeing as a quality of life; and the capabilities approach conceives a person’s life as a combination of various opportunities and capabilities, according to his or her freedom to choose among the set of opportunities available, in order to achieve those things that each person has reason to value.
Nourishment, health and survival are some elementary capabilities, and education is required to achieve other capabilities and to participate actively in political life, as well as security and social-connectivity [2]. As the capabilities and freedom approach is based on a sense of justice, ethics and values, they can be related to the lifestyle’s perspective, currently used in psychology, economics and communication research.
Lifestyle perspectives are based on shared values, in the worldviews from which people define as desirable goals, as guiding principles in people’s lives, which include market, reflexive, ethical, political, religious and intimacy values and preferences [3,4]. In consumption studies, lifestyles are defined as patterns in which people live and spend their time and money, based on how they interpret their own and others’ values and behaviours [3,5]. Lifestyles patterns vary by market groups and individuals, since consumers have different demographic characteristics, social and economic status, as well as different product or service interests, needs and desires, attitudes, preferences, behaviour and motives underlying consumption decisions [6].
These diverse individual characteristics influence also the dietary intake consumption patterns. For example, around the world, men, elderly, less educated and poor consumers are likely to have more difficulty reading, understanding and using available information in labels at packaged food to make healthy choices [7].
In this article, capacities and the freedom approach, combined with lifestyle perspectives, are explored to analyse child nutrition and to suggest relevant dimensions that are neglected, but should be taken into account in data construction and measurements of nutrition. Measurements of food and nutrition would be defined based on context, family or individual perspectives, comparing diverse concepts and different sources of information.
Socio-economic, market and policy contexts are analysed using the indicators developed by FAO, WFP and IFAD on context of food production and distribution, small farmers and local markets, community linkages [8].
Changes in dietary consumption level, frequency and composition are related to increasing availability and demand of processed and hyper-caloric foods with protein and saturated fats, sugars and refined grains, low in fibre, with decreasing prices; and corresponding decreases in the supply and demand of fruits, vegetables, integral grains and vegetables, whose prices increased.
Food industrialization and globalization promote a higher food availability, accessibility and diversity with low food prices, complemented with increases in per capita income, and in the purchasing power of a growing middle and upper class, promoting changes in consumption preferences and lifestyles.
Malthus assumptions about the insufficiency of future reduction of food production, facing population growth is far from being the cause of hunger and undernourishment.
Food production incorporates industrialization and high technology, increasing productivity. In developing countries, the expansion of arable area and multiple cropping and shorter fallow periods have promoted nearly 70% of the increase in crop production [9], decreasing food prices and promoting higher global consumption. Urban development and changes in the social role of women increased per capita family income, promoting changes in lifestyles and consumption patterns, in diet levels and composition, improvements in health, survival and nutrition [10,11].
Economic growth and increases in per capita incomes in the last three decades achieved nearly 2 percent per year globally. Food intake increased from 86 kcal per person per day in the developed countries and about 275 kcal in developing countries, mainly Asia and LAC. As income, diet composition and diversity improved and changed worldwide, from decreasing shares of cereals, roots and tubers to increase fruits and vegetables and animal-protein products in Asia and LAC, except in sub-Saharan Africa. Consumption of milk per person has almost doubled in developing countries, meat and fish consumption has tripled, and egg consumption has increased five times [8].
Diets are converging to form a more uniform pattern, while traditional local diet diversity is replaced, for example, the Mexican indigenous diet is based upon corn, beans, tomatoes, squash and chili and the Chinese, Bangladesh, Japanese, Indian and other original diets are consumed less, while new food products have been introduced, adapting to a Western diet pattern [12-15].
Despite of the fact that food overproduction, food distribution and consumption are unequal, monopolies and price volatility create market imbalances, leaving 700 million people hungry in the world [10,16]. The same imbalances and inequalities also underlie the emergence of overweight and obesity as a public health problem.
Some components of the set of opportunities defined by Amartya Sen and individual freedom to participate in the global consumer society are combined and underlying new standards of diet and lifestyles, and its unexpected consequences for health [2].
Family and community networks share knowledge and information, make decisions and establish relationships to access and distribute food among family members. Women, particularly mothers, are considered central agents in making decisions on diet composition and food distribution within the family.
At the individual level, the consumption and intake of food and calories reflect the quantity, frequency and quality of diet intake, the products, calories, macro and micronutrients intake per day or per week; while anthropometric measures reflect the outcomes of diet intake on the physical weight and height, at middle and large term.
The concept of malnutrition includes under and overnutrition, and is related to the concept of lifestyles as diverse forms to act upon and interprets the reality according to individual and family opportunities, capabilities, values and preferences.
2. METHOD
The study uses a descriptive comparison of quantitative international data developed by the United Nations on child mal nutrition across the world, based upon different approaches and methods. Results are organized in graphics and processed in new rate estimations to compare regions around the world; national and local research are analysed to highlight the relevance to generate more complex analysis on the determinants, mediations, consequences and inequalities in child mal nourishment, in order to suggest improvements in indicators and more effective policies to prevent both under and over nutrition.
3. RESULTS
FAO, IFAD and WPF measure food production as the national average number and proportion of under nourished children, represented as the “average consumer”, which declined since 1990, mainly before 2007-2008, but since the global crisis, the rate of decrease has slowed. More relevant reductions occurred in South Eastern, Eastern, Central and Southern Asia and in Latin America and the Caribbean. The reduction in Sub-Saharan Africa is slower and increases occurred only in Western Asia. In 2010 there were 100 million underweight children under the age of five, but the MDG in nutrition is closer to being reached (18.6% to 12.5%) [8].
Why there were such important improvements in reducing under-nourishment in almost all developing countries? Governments made increasing investments to strengthen small farmers, who represent 500 million farms in the world and produce 80% of food consumed. In Brazil, China, Vietnam, Ghana, Tanzania, Malawi, Rwanda, Ethiopia and Uganda, investments were made, credits, financial savings, services, infrastructure, storage, distribution, transportation, waste and markets, mainly at local and family agriculture, transformed peasant agriculture to more commercial, productive and profitable agriculture, oriented to the internal market and also to export. Governments promoted counter-cyclical measures to control increases in domestic food prices and developed public safety networks, regional and south-south cooperation and people have organized themselves to take collective actions. As a result, from 1990 to 2010, under-nourishment fell from 23.2 to 14.9 percent, poverty decreased from 47.5 to 22.4 percent and child mortality decreased from 9.5 to 6.1 percent [8].
The WHO, UNICEF and The World Bank report harmonized concepts and anthropometric indicators to estimate mal nourishment among children under five years old. International comparisons from 1985 to 2011 included 639 national surveys from 142 countries, made adjustments by age and urban-rural residence, conversions of child growth to the WHO-2006 standards and estimated prevalence by region and income group based upon linear mixed-effect modelling. This standardized data on child nutrition is internationally comparable, but differs from national country reports [17].
Four categories of malnourishment are defined: Stunting (low height for age), wasting (low weight for height), being underweight (low weight for age) and overweight (high weight for age). The results are similar to those estimated by FAO, IFAD and WFP using food production.
More than 90% of undernourished children lived in developing countries. Stunting is related to chronically insufficient diet intake and infections since the first and second year of age, with irreversible effects in health, motor and cognitive development and performance [18]. In 2011, there were 165 million of stunted children under five years of age in the world, corresponding to 26% of all children in this age group [17] (Figure 1).
Wasting is related to acute food shortage, morbidity and mortality under five years old. In 2011, there were 52 million of wasting children under five in the world (8%); and it is estimated that 1.5 million annual deaths of children under five could be attributed to being underweight. Moreover, 101million children under five (17%) were underweight [17].
Changes in the pattern of nutrition includes under and over-nutrition, in both developed and developing countries and in different social groups in the same population, diversifying inequalities within and among social groups
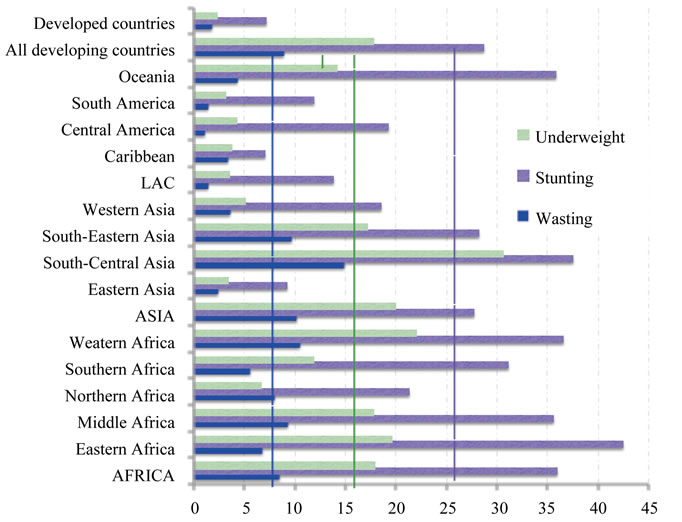
Figure 1. Prevalence of undernourished children, 2010. Source: WHO, UNICEF, WB report, 2012 [17].
and countries.
Malnutrition has multiple faces. While undernourishment is decreasing even in developing countries, being overweight is globally increasing, and both negatively affects child health and development.
Young children in particular benefit from animalsource foods. However, excessive consumption of red meat and salt, dairy products and eggs can increase the risk of heart disease, cancer, diabetes and obesity. And an adequate intake of fruits and vegetables contributes to the prevention of micronutrient deficiencies.
Persistent poverty and inequalities combined with a hyper-caloric diet and unhealthy lifestyles underlay the emergence of overweight and obesity as a public health problem.
In 2011, 43 million children over five years of age (7% of the total) were overweight or obese, of whom 32 million lived in developing countries (6.1% of the total) and 8 million in developed countries (11.7%). The prevalence of overweight children increased by 44%, compared to 1990, and the number of overweight children is expected to increase to about 60 million over the next decade.
The data in Figure 2 indicates that the prevalence of overweight children is much higher in developed countries, and in Southern and Northern Africa, followed by Western Asia and the LAC region. In South Central Asia there are 10 underweight children for each overweight child; in Eastern Africa this rate is 4 to 1, in Western and Middle Africa it’s 3 to 1, as well as in South Eastern Asia. In all other regions there are more overweight children, when compared to underweight.
The multiple faces of malnutrition show contradictory changes in the period from 1990 to 2010. Prevalence of stunted and undernourished children declined by 35%, and wasting declined by 11% wide the world, except in Western and Southern Africa, where decreases were lower than 20% and even there were increases in wasting children (20%, 45%). There are still important gaps and disadvantages for children in poorest African countries. (Figure 3).
Contrary to global trends, developed countries unexpectedly experienced increases in underweight and stunted children. Globally the prevalence of overweight children increased by over 40%, but in South Eastern Asia and Western Africa it increased by more than 220%, and in Western Asia and Southern Africa by around 150%.
Globally, being overweight at over 5 years of age is increasing at a higher rate than being underweight at under 5 years of age is decreasing.
Being overweight is an undesirable outcome of nutrition improvements, but is also considered to be malnutrition, accompanied by some types of micronutrient deficiencies or “hidden hunger”, which were overcome in a number of countries. For example, in Brazil, undernourishment and the deficiency of vitamin A decreased, whereas anaemia increased, even in metropolis such as Sao Paulo and Salvador, and in rural areas it can be much higher [19]. In India, even today, although undernourishment has declined, close to half of all Indian children are already underweight, and about half suffered from anemia [20].
Anthropometric measurements have to be analysed as
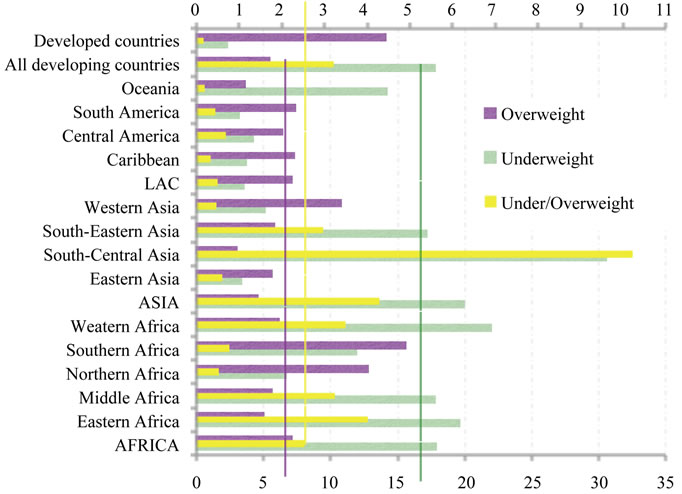
Figure 2. Underweight under 5/Overweight over 5, 2010. Source: Own estimations based on data from the WHO, UNICEF, WB report, 2012 [17].
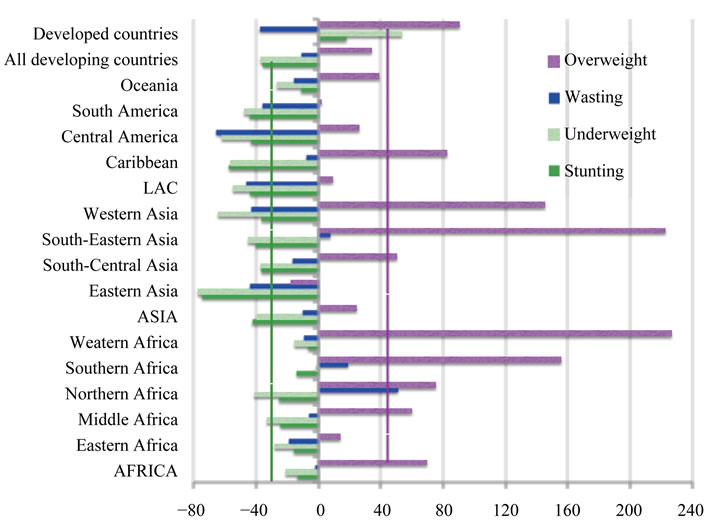
Figure 3. Changes in malnutrition, 1990-2010. Source: WHO, UNICEF, WB report, 2012 [17].
a cumulative indicator of nutritional deprivation from birth, independent of immediate circumstances. Height changes in the long-term, while weight and wasting change in the short-term, while the relationship of weight-for-age captures stunting and wasting, and reflects variations in nutrition status in both the short and large term, and is used as a more sensitive and efficient indicator. In a specific population the distribution of anthropometric measures is used as a standard reference to apply two standard deviations and define the adequate child growth in the country [20], and in international comparisons they are adjusted to estimate universal anthropometric standards for children.
4. DISCUSSION
4.1. Sources of Information, Data and Comparative Measurements
International comparisons are indispensable in a globalized world, to establish goals and share commitments to improve nutrition and equality within and among countries, and standardizations are necessary to estimate comparable data on nutrition, poverty, employment and other relevant components of economic and human development.
As in population projections, data from past years are adjusted based on long-term trends, and standardization can underestimate current trends, mainly the most recent data. For example, in Latin American and the Caribbean countries population projections were not able to foresee that the aging process would be much faster than estimations suggested, because projections were based upon past censuses from previous decades, when this process was already slower than in the 21st Century. After the 2010 censuses round, projections should be reviewed in most of the countries, to update data with recent trends, such as fertility decreased quicker than expected and youth mortality emerged as a social problem.
Standardized indicators on malnutrition are probably underestimated too, since recent surveys from 2006 to 2012 indicated great improvements in child nutrition in populous and developing countries, which were not considered in the set of 20 years databases analysed from 1985 to 2005, nor taken into account in the last standardized estimations. For example, Brazil, China, South Africa recently applied health surveys that indicate new great improvements in nutrition [12,21,22].
Developing countries had greater gaps and achieved higher improvements in child nutrition in the last decade, whereas developed countries achieved excellent results in the past, but are currently worsening child nutrition conditions, facing unemployment and decreases in social protection coverage.
As recent trends were not considered in available international comparisons, the results presented may be considered underestimated for developing countries, considering improvements achieved, and overestimated for developed countries, when compared to their recent worse nutritional results.
The contrast of standardized estimations with national data from original censuses and surveys is relevant to highlight new trends and to prevent that data being anchored in the past.
Another methodological concern in analysing compared data among countries is the diversity in national culture and diet lifestyles, such as vegetarian diet, and the reproduction of gender inequalities and social discrimination systems. For example, India presents a paradox. While economy and real per capita income have grown at historically unprecedented rates since 1980, per capita consumption and calorie intake declined, but the proportion of underweight children remained virtuallyunchanged [20]. Some explanations rely on the reduction in calorie requirements, supposedly related to declines in levels of physical activity and improvements in the health environment. A higher quantity of calories and a balanced diet containing not only cereals but also fruits and vegetables, as well as a higher access to clean water, sanitation, good hygiene practices and vaccinations and means of transport such as bicycles, could improve health and decrease activities which high consume calories. However, other approaches highlight that health and transportation services have remained constant and the inflation has considerably increased [23,24].
Therefore, data on nutrition involves complex factors. Not exclusively dietary intake, but also the amounts of energy and nutrients available for metabolism and socio-economic context. However, even dietary intake is measured in terms of food intake and not in terms of energy for individual metabolism. Moreover, food intake varies day-to-day and in short periods of time, while surveys ask for the food consumption in the last day or in the last week and cannot reflect the long-term habitual intake of individuals [25]. And diet intake varies in the life course, according to changes in food prices and availability, to family purchasing power, preferences and lifestyles.
4.2. Poverty, Inequalities and the Role of Women and Family in Nutrition
Poor and rural families have low purchasing power, capacities and possibility to get adequate food within an accessible price-range [10], since they depend mostly upon the impact of barriers, prices volatility, market accessibility, distance and cost of transport to access and get adequate food, as well as the accessibility and price of combustibles to cook. Poor families spend most of their income on food and are more vulnerable to price variations, for example during economic crisis and disasters [8].
Other dimensions are involved in the relationship between poverty and inequalities and child underweight, wasting, overweight, anaemia, infections and mortality. Stronger determinants are deficient mothers’ level of education and empowerment, health assistance and sanitary conditions [26]. Both trends, under-nourishment decreases and overweight increases, have as common determinants inequalities in food distribution made by mothers’ with poor capacities and resources. Gender disparities are much larger among young women of poor households, who are less educated and empowered and with poor nutritional knowledge levels; they are more likely to be exposed to unemployment, unskilled, informal and low remunerated jobs, to marry earlier and have more children to share income and food.
Families with more children, and particularly young couples with small children are likely to be poor and, therefore, malnourished. All these factors are also related to child malnutrition, as well as low access and inadequate services of water, sanitation and health, domestic violence, illness and dedicated care for children by their maternal grand-mothers [27-29].
Food distribution within the family is a women’s decision. Mainly in developing countries, women and girls have less access to food and receive poorer, less healthy, and unsafe food than men and boys, and are more likely to be stunted than boys [18,24].
Most of the income of poor families is used to buy food, and women/mothers make the relevant decisions about food expenses and food distribution among the family members. Mothers are mainly responsible for buying, cooking and distributing food among the members of the household, women’s position in decisionmaking within and outside the household, and their decisions and behaviour in getting a job, allocating income, childcare and accessing healthcare are at the centre of all other children nutritional determinants. Nutrition is defined by women and within families. The care and nurturing of children depend on the mothers’ nutritional knowledge, decisions and behaviours [24,28,30].
However, poverty and gender inequalities are reproduced within households, through cultural and imbalanced power relationships between genders and generations, promoting ambiguities in the role assumed by women in distributing food among family members and can limit their capacity in guaranteeing equal and adequate nourishment for the most vulnerable family members. For example, in Gambia men receive food firstly and in higher quantities and quality than women and children [28].
As women are much more likely than men to spend additional income on nutrition and healthcare [31-33], policies focus adequate nutritional and health knowledge and food provision in women. However, women can adopt traditional values and behaviours and not always translate it into appropriate actions [28,34]. Education and the additional income from women contribute to women empowerment, but also to poverty and child under-nourishment reduction, family equality and human development.
Community and social networks and services play an important role in children nutrition. For example, in rural Africa, the survival of maternal grand mothers and their support of adult mothers have a significant effect on the grand children survival and nutrition [28,35,36].
In contrast, youth women are quickly changing their diet consumption patterns, increasing the intake of unhealthy food, which are highly consumed at home and in fast food restaurants. Adolescent and young women, mainly those who combine study with work, the poorer and African descendants, have adopted these unhealthy food consumption patterns and experience barriers to access healthy food, despite their own perception, maternal and peer concerns about healthy eating and its consequences [37, 38].
Women’s education and empowerment promote healthier and equalitarian decisions and behaviour within the household, as well as community networks and market. These are important keys to analysing the multiple faces of child malnutrition and are relevant dimensions in shaping and changing lifestyles in food consumption, reducing risks of malnutrition, and in guaranteeing adequate and equal food access by generations and gender and the distribution within the family.
4.3. Social Policies, Poverty and Family
Policies to reduce poverty are oriented to families, mainly to mothers and children, and can be strategically linked to local agriculture, child-care institutions, school and health services, food complement, information, education and support to accessing food and adopting healthy diets and life-styles.
LAC countries have achieved good results in reducing poverty and under-nourishment adopting, among other programmes, Conditioned Cash Transfers (CCTs), implemented for more than ten years in 20 countries in the region, with coverage of more than 100 million people, and which rein forces child nutrition and education, family health, and women empowerment.
CCT programmes have also been implemented in Asia, Bangladesh, Sri Lanka and the Philippines, and recently in Africa: Nigeria, Uganda, Kenya, Zambia and Malawi, Ethiopia, South Africa, Angola and Mozambique, countries where nutrition trends have also presented relevant improvements in the last decade.
The next step in CCT programmes could be linking food production, food distribution and mothers’ food knowledge and decisions components, in order to accelerate the achievements in reducing under-nourishment, to promote healthier diets and life-styles, and to control recent increases in child overweight and obesity and its unhealthy consequences.
5. CONCLUSIONS
Currently food is abundantly produced, but unequally distribution and access of food reinforce inequalities and disadvantages for poorest families, who spend most of their income to purchase food and are more vulnerable to price volatility and natural disasters.
Anthropometric measurements represent the results of diet intake, food security and women’s capacities and decisions regarding family budgets, food consumption, distribution and lifestyles.
The measurement of food and nutrition should combine quantitative data with qualitative research, to produce more complex explanations and policy suggestions by asking about mothers’ knowledge, decisions and practices on nutrition and lifestyles. For example, how do mothers make decisions about food consumption and distribution in the market and within the family? What are the barriers they face, the economic and time cost in accessing, preparing and distributing healthy food close to and inside home? What are women’s and mothers’ preferences and resilience to adopt a diverse and healthy diet and promote its equalitarian consumption among family members?
Female decisions and empowerment and a family approach are relevant to change lifestyles in order to ensure a healthier nourishment, survival and human development for children.
Collaboration among national programmes, child-care, education and health sectors can promote continuous knowledge, regular checks of children nutritional status, and the integration of activities and policies to involve and empower mothers, based on scientific evidence from family indicators included in research, surveys, and policies.
REFERENCES
- Stiglitz, J., Sen, A. and Fitoussi, J.P. (2009) The measurement of economic performance and social progress revisited. Reflections and overview. Commission on the Measurement of Economic Performance and Social Progress, Paris.
- Sen, A. (1985) Well being, agency and freedom: The dewey lectures. The Journal of Philosophy, 82, 169-221.
- Solomon, M.R. (1994) Consumer behavior: Buying, having, being. Allyn and Bacon, Boston.
- Vyncke, P. (2002) Lifestyle segmentation. From attitudes, interests and opinions, to values, aesthetic styles, life visions and media preferences. European Journal of Communication, 17, 445-463. doi:10.1177/02673231020170040301
- Gunter, B. and Furnham, A. (1992) Consumer profiles: An introduction to psychographics. Routledge, London.
- Demby, E. (1974) Psychographics and from whence it came. In: Wells, Ed., Life Style and Psychographics, American Marketing Association, Chicago, 9-30.
- Cowburn, G. and Lynn, S. (2004) Consumer understanding and use of nutrition labelling: A systematic review. Public Health Nutrition, 8, 21-28. doi:10.1079/PHN2005666
- FAO, WFP and IFAD (2012) The state of food insecurity in the world. Economic growth is necessary but not sufficient to accelerate reduction of hunger and malnutrition. Joint FAO/WFP/IFAD report. FAO, Rome.
- FAO, WFP and IFAD (2011) The state of food insecurity in the world. How does international price volatility affect domestic economies and food security? Joint FAO/ WFP/IFAD report. FAO, Rome.
- Sen, A. (1999) Development as freedom. Oxford University Press, Oxford.
- Popkin, B.M. (1993) Nutritional patterns and transitions. Population and Development Review, 19, 138-157. doi:10.2307/2938388
- Castañon, R., Solleiro, J. and Del Valle, M. (2003) Structure and perspective of the food industry in Mexico. National Bank of International Trade, 53, 104-113.
- The National Institute of Nutrition and Food Safety at the Chinese Centre for Disease Control and Prevention & the Carolina Population Centre at the University of North Carolina at Chapel Hill (2009) China health and nutrition survey (CHNS). http://www.cpc.unc.edu/projects/china
- Ahmed, T., Mustafa, M., Santhia, I.A.M., et al. (2012) Nutrition of children and women in Bangladesh: Trends and directions for the future. Journal of Health, Population and Nutrition, 30, 1-11. doi:10.3329/jhpn.v30i1.11268
- Misra, A., Singhal, N., Sivakumar, B., et al. (2011) Nutrition transition in India: Secular trends in dietary intake and their relationship to diet-related non-communicable diseases. Journal of Diabetes, 3, 278-292. doi:10.1111/j.1753-0407.2011.00139.x
- FAO (2010) Measuring food and nutrition security: What has been your experience? Summary of discussion 74. FAO, Rome.
- WHO, UNICEF and The World Bank (2012) Joint child malnutrition estimates—Levels and trends. Joint WHO/ UNICEF/The World Bank report. WHO, New York.
- UNICEF (2007) Progress for children 2007—Stunting, wasting and overweight. WHO, New York.
- Leal, L.P., Batista, M., Cabral, P.I., et al. (2011) Prevalence of anemy and related factors in children from 6 to 59 months of age. Journal of Public Health, 45, 457-466. doi:10.1590/S0034-89102011000300003
- Deaton, A. and Drèze, J. (2009) Nutrition in India: Facts and interpretations. Economic and Political Weekly, 44, 42-65.
- Brazil (2013) Summary of indicators on food security and nutrition—Brazil and regions. Health Ministry & National Institute of Geography and Statistics, survey on family budgets 2008-2009. http://www4.planalto.gov.br/consea/consea-1/arquivos/indicadores-brasil-e-regioes
- South Africa Human Sciences Research Council (HSRC), National Department of Health (NDOH), The Medical Research Council (MRC), et al. (2013) South-African national health and nutrition examination survey (SANHANES).
- Basu, D. and Basóle, A. (2009) Relations of production and modes of surplus extraction in India: An aggregate study. Working Paper.
- Shagun, S., Subramanian, S.V., McCormick, M.C., et al. (2012) Husband’s preference for a son and women’s nutrition: Examining the role of actual and desired family composition on women’s anaemia and body mass index in India. Paediatric and Perinatal Epidemiology, 26, 77- 88.
- Rutishauser, I.H.E. (2005) Dietary intake measurements. Public Health Nutrition, 8, 1100-1107. doi:10.1079/PHN2005798
- Monteiro, C.A., Benício, M.H.D., Konno, S.C., et al. (2009) Causes of the diminution of the child undernourishment in Brazil. 1996-2007. Journal of Public Health, 43, 35-43. doi:10.1590/S0034-89102009000100005
- Commission on the Social Determinants of Health (2008) Closing the gap in a generation: Health equity through action on the social determinants of health. Final report. Commission on the Social Determinants of Health, Geneva.
- Mwangome, M., Prentice, A., Plugge, E., et al. (2010) Determinants of appropriate child health and nutrition practices among women in rural Gambia. Journal of Health, Population and Nutrition, 28, 167-172. doi:10.3329/jhpn.v28i2.4887
- Kamiya, Y. (2011) Socioeconomic determinants of nutriational status of children in Lao PDR: Effects of household and community factors. Journal of Health, Population and Nutrition, 29, 339-348. doi:10.3329/jhpn.v29i4.8449
- Lloyd, C.B., Kaufman, C.E. and Hewett, P.C. (2000) The spread of primary schooling in sub-Saharan Africa: Implications for fertility change. Population and Development Review, 26, 483-515. doi:10.1111/j.1728-4457.2000.00483.x
- Chant, S. (1999) Informal sector activity in the third world city. In: Pacione, M., Ed., Applied Geography: An Introduction to Useful Research in Physical, Environmental and Human Geography, Routledge, London, 509- 527.
- Gomes, C. (2006) Households living in moderate poverty in Mexico. Socio-demographic profile and interrelations. In: Venzor, A., Gomes, C. and Valenti, G., Eds., The Challenge of the Informality and Moderate Poverty, Miguel Angel Porrua, Mexico City, 47-184.
- Gomes, C. (2007) Population situation analysis, Latin America and the Caribbean. Diversities and inequalities. UNFPA, Panama.
- Lee, G.R. and Garvin T. (2003) Moving from information transfer to information exchange in health and health care. Social Science & Medicine, 56, 449-464. doi:10.1016/S0277-9536(02)00045-X
- Sear, R., Mace, R. and McGregor, I.A. (2000) Maternal grandmothers improve nutritional status and survival of children in rural Gambia. Proceedings of the Royal Society—biological sciences, 267, 1641-1647. doi:10.1098/rspb.2000.1190
- Aubel, J., Touré, I. and Diagne, M. (2004) Senegalese grandmothers promote improved maternal and child nutrition practices: The guardians of tradition are not averse to change. Social Science & Medicine, 59, 945-959. doi:10.1016/j.socscimed.2003.11.044
- French, S.A., Harnack, L. and Jeffery, R.W. (2000) Fast food restaurant use among women in the pound of prevention study: Dietary, behavioral and demographic correlates. International Journal of Obesity and Related Metabolic Disorders, 24, 1353-1359. doi:10.1038/sj.ijo.0801429
- French, S.A., Story, M., Neumark-Sztainer, D., et al. (2001) Fast food restaurant use among adolescents: Associations with nutrient intake, food choices and behavioral and psychosocial variables. International Journal of Obesity and Related Metabolic Disorders, 25, 1823-1833. doi:10.1038/sj.ijo.0801820