Open Journal of Nursing
Vol.08 No.11(2018), Article ID:88840,19 pages
10.4236/ojn.2018.811065
Gender Differences in Usage of Over-the-Counter Analgesics among Norwegian Adolescents
Sindre Lorentzen1, Bente Lorentzen2, Britt-Maj Wikström3,4
1University of Stavanger, Stavanger, Norway
2Akershus University Hospital, Lørenskog, Norway
3Department of Public Health Sciences, Karolinska Institute, Solna, Sweden
4Oslo Met (Oslo Metropolian University), Oslo, Norway

Copyright © 2018 by authors and Scientific Research Publishing Inc.
This work is licensed under the Creative Commons Attribution International License (CC BY 4.0).
http://creativecommons.org/licenses/by/4.0/



Received: October 25, 2018; Accepted: November 26, 2018; Published: November 29, 2018
ABSTRACT
Introduction: Usage of over-the-counter (OTC) analgesic has increased among Norwegian adolescents since 2001. It has been noted that females tend to have a higher usage compared to males. In this paper we explore this gender difference. Data: Our dataset consists of 284,674 from Norwegian adolescents attending junior high school and high school between 2014 and 2017. Methods: The econometric approach consists of applying ordered logistic regressions with usage of OTC analgesics as the dependent variable and a dichotomous gender variable as the independent variable. Control variables include variables such as frequency of physical and mental health problems and other sociodemographic variables. Results: Gender, physical and mental health problems and various sociodemographic variables are found to have a significant effect on usage of OTC analgesics. Females are predicted to use significantly more analgesics. A large proportion of the gender difference evaporates when controlling for various other determinants. Conclusion: A considerable part of the observed gender difference in OTC analgesic usage can be traced back to differences in frequency and severity of physical and mental health problems. Part of the gender difference in usage, however remains unexplained.
Keywords:
Over-the-Counter Analgesics, Cross-National Ungdata, Adolescents, Gender

1. Introduction
Evidence from Europe, including Norway, and United States, shows that usage of over-the counter (OTC) analgesics among adolescents is considerable [1] - [8] . Furthermore, statistics indicate that the level of usage is on an increasing trend. The usage of OTC analgesics among Norwegian adolescents has increased since 2001 [3] [9] [10] [11] . Usage of paracetamol and ibuprofen increased by 1.7% and 1% respectively in 2016, where 55% of the sale was conducted in non-pharmacy outlets. The overall OTC sales of paracetamol correspond to a usage of 36 tablets per inhabitant [12] . A study from Germany found that it was very common among adolescents to use self medication such as over-the-counter drugs analgesics [1] . Similar result is found in a meta-analysis with a broader sample [13] . It is well known that over-the-counter analgesics can be effective for adolescents in providing relief from various symptoms. The most widely consumed over-the-counter drugs are analgesics (OTCAs) [14] . The most common OTCAs in Norway are Paracetamol and Ibuprofen [10] [12] . Increased usage of analgesics could be a reason for concern as usage of analgesic medications purchased over the counter is not necessarily harmless. The Norwegian Institute of Public Health reports a significant increase in the number of incidents of self-inflicted paracetamol poisoning among Norwegian girls aged 15 - 19 years. From 2008 to 2016, there was an increase from less than a hundred inquires per year to more than two hundred. Based on a comprehensive review of the literature, a study [15] suggests there could be a considerable degree of toxicity regarding usage of paracetamol―especially for higher usage. Self-medication when adolescents do not follow the recommended dosage might cause liver failure and hepatocellular necrosis when paracetamol is taken in overdose [15] [16] [17] . Several studies have shown that ibuprofen (ibux) can give gastrointestinal symptoms [18] [19] [20] [21] , cardiovascular [22] and renal events [23] .
This paper, however, is concerned with a particular empirical regularity found in the data. Females are consistently found to have a higher usage of OTC analgesics compared to males throughout the literature. Despite being a well-known stylized fact, a study [24] points out that this gender-based difference is not well understood. As argued in another study [6] , frequent usage of analgesics is not necessarily bad. For instance, high usage could be considered both necessary and rational if the intention is to alleviate a medical condition evaluated by a physician. As such, it becomes important to understand the underlying drivers of the observed gender-difference in usage of OTC analgesics. Specifically, it is essential to determine whether higher usage among females is primarily driven by rational or irrational causes.
Several issues related to the use of over-the-counter or non-prescription analgesics and other medications have been investigated throughout the literature. One strain of research within the field pertains to whether adolescents are equipped in terms of literacy, knowledge and attitude to correctly use OTC analgesics. For instance, a study [25] investigated the use of OTC medication among eight graders in New Hampshire between 2010 and 2011. They found that autonomous self-administration of OTC medication was prevalent in their sample of 101 adolescents. Based on this empirical finding the authors found it pertinent to investigate if the level of literacy among these 13 - 14-year olds was sufficiently adequate to properly self-administer. Another study [26] follows a similar line of inquiry by investigating the perception and attitude towards OTC analgesics among 77 Swedish teenagers in the age of 16 - 19 in 2010. Through a focus group discussion, they found heterogeneity in the respondents’ attitude, perception and knowledge on OTC analgesics. While the majority appeared to exhibit a responsible approach to usage, instances of casual to careless attitude were revealed among the teenagers. Analogously, an American study [27] investigated the prevalence of knowledge gaps and misconceptions among adolescents aged 14 to 20 with a sample size of 96. Inquiring about the adolescents’ frequency of usage and knowledge regarding side-effects, risks and interaction between drugs, they found an average overall knowledge score of 44%. Knowledge was, however, heterogeneous across age and different ethnicities. Another study [28] applied multiple logistic regression analysis to inappropriate self-medication with a sample of 6226 students from 99 different primary, middle and high schools from 2016. Variables such as lower medication knowledge, lower self-efficacy, lower medication literacy, consumption of tobacco and alcohol were found to predict inappropriate self-medication.
Another branch of the literature explores the various root causes and determinants of OTC analgesics usage. A Norwegian study [2] investigates the determinants of high-frequency usage of analgesics among Norwegian adolescents. They apply one-on-one in-depth interviews on a sample of three boys and sixteen girls in the age group of 14 to 16 during 2013 and 2014. Several possible drivers of OTC analgesics usage were suggested, such as physical pain (headache, stomach pain, etc.), conflicts with family and peers, a strong need to feel appreciated and appear successful (academic, sport, art and culture), stress and fatigue. In a similar study [3] , a cross-sectional questionnaire-based study is applied to a sample of 626 Norwegian adolescents aged 15 to 16. Comparing high-frequency users to low-frequency users, they find that the former group typically experiences more widespread and frequent pain, binge drinking, lower self-esteem, higher frequency of school abstinence, engaged in more spare-time work, higher consumption of caffeinated drinks, less sleep and lower educational ambitions. Another cross-sectional study [4] with a sample of 646 Norwegian adolescents where postal questioners and telephone interviews were conducted in 2005 and 2012 found an association between parents’ and adolescents’ use of OTC analgesics. Headache was further found to be the most important driver of analgesics usage and females were more frequently found to use analgesics compared to males. Similar results are found regarding the link between parents’ and adolescents’ usage of analgesics [29] . The authors suggest that parent’s usage influences the adolescents’ usage through two main channels of transmission: a socialization pathway and a pathway related to adverse living conditions. A Danish study [5] conducts in-depth interviews with 20 females aged 16 - 20. Their analysis shows that headache is an important driver behind usage of analgesics, and that the participants attributed headache to stressful conditions in their everyday life. In other words, there is evidence suggesting that females use OTC analgesics to combat discomfort, stress, and better enable them to participate in social interactions.
Another study [11] applied logistic regressions to usage of OTC analgesics on a sample consisting of 40,000 Norwegian adult respondents. Their results show that women tend to use more OTC analgesics compared to men, frequency and intensity of pain was a strong predictor of OTC analgesic usage and physical activity was found to predict lower usage. Variation in usage across age was also found. Finnish researchers [6] applied multinomial logistic regression to a sample of 6500 people aged 15 - 74. High frequency usage of analgesics was found to be linked to continuous pain and high intensity pain, low mood and not being employed. A study [1] analyses a sample of 17,450 German children aged 0 - 17 during 2003-2006. Results suggest that self-medication with OTC drugs is higher among children with poor health status and children from families with higher socioeconomic status in terms of household income and mothers’ level of education. A Swedish researcher [30] conducts a study on gender differences in dispensed analgesics with a nationwide sample of all dispensed prescription drugs in Sweden during 2006-2015. Women were found to have a higher usage across most groups of dispensed analgesics. A study [7] applied multilevel logistic regression to a sample of Scottish school-aged children from 1998, 2006 and 2010. Headache, stomach ache, nervousness and health complaint frequency were found to be important determinants of medicine usage. A literature review of 163 papers on selfmedication among adolescents aged 13 to 16 [14] showed that headache, allergies, and fever were found to be the most frequent drivers of self-medication. Other important drivers of self-medication included variables such as gender, age and maternal education. A quantitative cross-sectional survey on 131 children aged 6 to 11 years [31] found that selfmedication was strongly associated with maternal use of OTC analgesics. Table 1 summarizes the various determinants of OTC analgesic usage identified throughout the literature and their respective expected relationships.
1.1. Aim
The aim of this research is to empirically investigate gender differences in usage of OTC analgesics among Norwegian adolescents. By using a large sample of Norwegian adolescents, we attempt to identify the empirical association between OTC analgesic usage and gender while controlling for various variables such as frequency of self-reported physical and mental health problems and several sociodemographic variables.
1.2. Structure of the Paper
The remainder of this paper is structured as follows. In Section 2, the data is presented and the econometric methodology is explained. In Section 3, the obtained results are reported. Section 4 concludes.

Table 1. Evidence on determinants of OTC analgesic usage.
2. Data and Methodology
The dataset utilized throughout this paper was extracted from the Norwegian Ungdata survey1 conducted on Norwegian adolescents attending either junior high school (8th to 10th grade) or high school (1st - 3rd grade) on an annual basis between 2014 and 2017. The Ungdata survey is financed through the national budget and the research center NOVA at the Oslo Metropolitan University (formerly known as the university college in Oslo and Akershus) and the com petence center KoRus and Kommune sektorensorganisasjon (KS) is responsible for developing the survey. The survey is conducted electronically during school hours, where the adolescent respondents are anonymized, and their parents are offered the option to withdraw them from the survey. Further relevant ethical considerations were complied with.
A total of 284,674 respondents participated in the survey between 2014 and 2017 drawn from all 19 counties in Norway. Figure 1 shows temporal development in participation across both gender2 and school level. As observed, the number of self-identified females and males are fairly equal. Males tend to outnumber females for lower percentiles of age, but the discrepancy is more likely driven by gender-based heterogenous willingness to participate and dropout rates. Participation across junior high school and high school, however, experience a more prominent discrepancy, but the number of participants from high-school appears to be colinear with number of participants from high school. As enrolment in junior high school is mandatory while high school is optional, the discrepancy is to be expected.
Our main variable of interest pertains to self-reported usage of over-the-counter analgesics among Norwegian adolescents. The question the respondents are asked to answer, is formulated as follows: “How often have you used non-prescription drugs (Paracet, Ibux, etc.)”. Five possible pre-coded answer alternatives were offered to the respondents. These include: 1) “Never”, 2) “Less than weekly”, 3) “At least weekly”, 4) “Several times a week”, and 5) “Daily”.
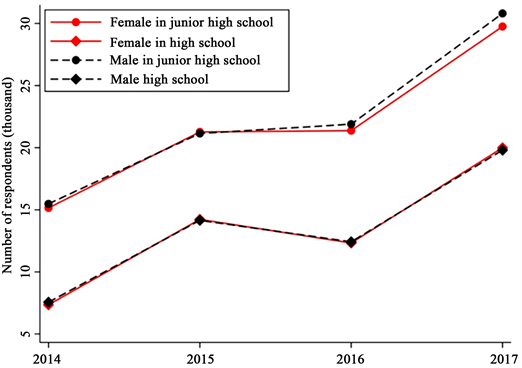
Figure 1. Participation rate across gender and school level. Source: Ungdata survey 2014-2017.
About 99.13% of the 284,674 participants provided an answer to usage of OTC analgesics, while 2484 did not respond. Figure 2 shows variation in response to usage of painkillers across time and gender. As observed in Figure 2(a) frequency in usage is relatively stable across the sample period of 2014 to 2017. On average, 35.39% of the participant reported that they “never” use prescription-free painkillers, while 54.08%, 10.18%, 5.55% and 1.80% reported “less than weekly”, “at least weekly”, “several times a week” and “daily” respectively. From Figure 2(b) we can observe an unequal distribution of gender across different self-reported frequency of prescription-free painkiller usage. With the exception of the first alternative (“never”), females are overrepresented. For “less than weekly”, “at least weekly”, “several times a week” and “daily”, 55%, 67%, 73% and 58% of the respondents are female.
Our econometric approach consists of applying an ordered logit model to usage of over-the counter analgesics on a set of control variables. Following the notion of Wooldrige [32] , let be and ordered response, in our case OTC analgesic usage, taking on the values for some known integer. Further, let a latent variable be derived as in Equation (1)
(1)
In this equation, is a matrix of with independent (explanatory) variables with observations, denotes a vector of coefficients, and is a vector of residuals which are normally distributed conditional on. Let denote the threshold parameter or cut point. For a given value, we have. With the threshold parameters and the latent variable equation, can be derived as in Equation (2).
(2)
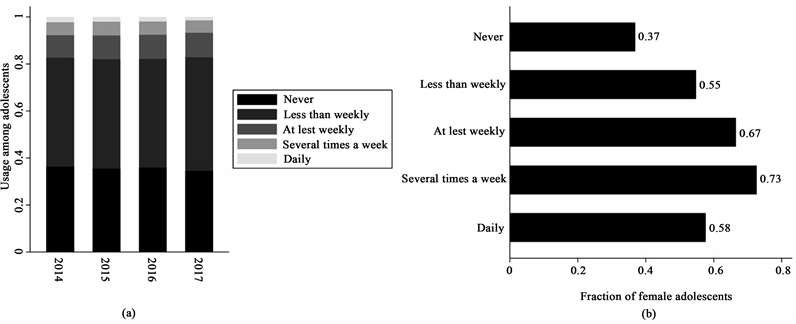
Figure 2. Reported usage of prescription-free painkillers among Norwegian adolescents (20142017). (a) Variation across time; (b) Variation across gender
The parameters to be estimated can be obtained by applying maximum likelihood estimation. The relevant log-likelihood function is given by Equation (3).
(3)
The obtained estimates of the model parameters, the response probabilities can be computed―see Equation (4).
(4)
3. Empirical Results
In this section we report the empirical results from applying an ordered logistic regression model to consumption of over-the-counter analgesics by Norwegian adolescents. Subsection 3.1 applies a univariate model, while 3.2 and 3.3 expands the model with a multivariate specification. Subsection 3.2 investigates the effect of physical and mental health problems and 3.3 investigates the effect from various variables suggested by the literature.
3.1. Variation in Usage across Genders
The aim of this paper is to elucidate how the usage of over-the-counter analgesics varies across gender among Norwegian adolescents between 2014 and 2017. Our econometric approach to answer the proposed research question consists of applying an ordered logit regression model with frequency of self-reported usage of OTC analgesics on a dichotomous gender variable. Both the dependent and independent variables are described in Equations (5) and (6).
(5)
Gender takes on the values of if the respondent reported on being female and if male. No other gender expressions were permitted in the survey. Usage of OTC analgesics is an ordered discrete variable taking on values from to corresponding to: “never”, “less than weekly”, “at least weekly”, “several times a week” and “daily”.
(6)
Table 2 shows the regression results. With an obtained odds ratio of 2.36 for the gender variable, females have a higher odds of being in one frequency higher than the males. In other words, given everything else being equal, the female adolescents are predicted to have a significantly higher usage of OTC analgesics compared to the male adolescents.
3.2. Effect of Physical and Mental Health Problems
In this subsection, we investigate how both physical and mental health problems affect selfreported usage of OTC analgesics. Table 3 shows univariate and multivariate results from regressing OTC analgesic usage on various forms of physical pain and gender. As observed, all form of pain yields a significant odds ratio with positive effect both under univariate and multivariate specification. In other words, increased frequency and severity of neck and shoulder pain, joint and muscle pain, nausea, palpitations, headache and stomach ache predicts higher usage of OTC analgesics. The odds ratios, however, are closer to 1, i.e. no effect, when the model is multivariate. This is to be expected as there is correlation between these variables. The gender dummy for females is found to yield a positive effect on usage of OTC analgesics when controlling for the various physical pain variables. In other words, some of the difference observed between the gender regarding usage can be accounted for by different level of frequency and severity of physical pain. When physical health problems are taken into account, some of the observed gender difference is eliminated.
Table 2. Univariate ordered logit result.
Table 3. Physical health problems (see Table A1 in the Appendix for further variable description).
Analogously, Table 4 shows univariate and multivariate results from regressing OTC analgesic usage on various forms of depression like symptoms and gender. Both under univariate and multivariate specification, increased frequency of tiredness, sleep problems, unhappiness, sadness or depression, tenseness, being worried and being angry or aggressive is found to predict increased usage of OTC analgesics. Hopelessness and loneliness are, however, found to yield conflicting effect depending on whether the model is univariate or multivariate. Again, this is most likely caused by a high extent of correlation between the variables. As with physical pain, when controlling for depression like symptoms, the effect of being female on usage of OTC analgesics is reduced but still positive and significant.
Table 5 shows univariate and multivariate results from regressing OTC analgesic usage on various forms of anxiety like symptoms and gender. Increased
Table 4. Depression like symptoms (see Table A2 in the Appendix for further variable description).
Table 5. Anxiety like symptoms (see Table A2 in the Appendix for further variable description).
frequency and severity of all variables is found to predict increased usage of OTC analgesics under both specifications. Increased frequency of being afraid without any discernible reason, being anxious, felling dizziness, experiencing inner turmoil or nervousness, propensity to cry and self-blaming is found to predict higher usage of OTC analgesics. Being anxious is, however, found to yield conflicting effect on usage depending on model specification. The dichotomous gender variable remains positive and significant when controlling for these various symptoms of anxiety.
3.3. Determinants of Over-the-Counter Analgesic Consumption
In this subsection we investigate the empirical effect of various variables suggested in the extant literature on consumption of OTC analgesics. Table 6 shows summary statistics for a selection of these variables. Based on the summary statistics, we observe that females on average are significantly more bothered with physical and mental health problems, such as headache, stomach ache, sleep problems and depression like symptoms. These variables are measured on a scale from 1 to 4, where a higher number is associated with a higher frequency or severity of the issue. For example, the average score for females is 2.32 with a standard deviation of 0.84, while the average and standard deviation for males are 1.89 and 0.73 respectively. Hence, there is a difference of 0.43 which is found to be significantly different from zero. This implies that females on average have a significantly higher self-reported frequency and severity of headache. The same appears to be the case regarding stomach ache, sleep problem and depression
Table 6. Summary statistics of independent variables (see Table A3 in the Appendix for further variable description).
like symptoms (unhappy, sad or depressed). Further, females are comparatively less satisfied with themselves, quarrel more with their parents3, drink more coffee, less likely to evaluate sport achievements to be important for their status and more likely to have a high academic ambition. Some minor differences exist between the genders regarding frequency of getting intoxicated from drinking alcohol, being bullied, engage in spare-time job and evaluated importance of academic achievements among peers. No significant difference was found in propensity to shirk school.
Table 7 shows both univariate and multivariate regression results from regressing usage of OTC analgesics on proposed explanatory variables suggested in the literature. The variables are sorted from most to least important based on the absolute value of the t-statistics from a univariate regression. Through backward elimination based on AIC and BIC values, we find that the best trade-off between explanatory power (log-likelihood) and model parsimony is found when all proposed variables are included.
Table 7. Multivariate ordered logistic results (see Table A3 in the Appendix for further variable description).
By ordering the variables according to t-statistics, the explanatory variables are sorted from post important to least imports, at least from an empirical perspective. With the exception engaging in spare-time jobs, increased frequency or severity of all other variables predicts increased usage of OTC analgesics. As before, higher frequency of headache, stomach ache, sleep problem and feeling unhappy, sad or depressed exhibit a positive effect on usage. Conforming to expectations, the physical and mental health problems are found to be the most important predictors of OTC analgesic usage. Increased lack of self-esteem predicts increased usage of OTC analgesics. Increased level of conflicts with parents (scale is reversed such that a lower value corresponds to higher frequency) is found to predict increased usage. Accordingly, increased frequency of being bullied (the scale is reversed) by peers corresponds to increased usage. Consumption of coffee is similarly found to have a significant effect on OTC analgesic usage. The more frequently the respondent report on buying coffee, the higher usage of analgesics is predicted to be. Contrary to literature, increased frequency of engaging in spare-time jobs, is found to yield a negative effect on OTC analgesic usage. The more the adolescents work, the lower the frequency of headache. Although, it is possible that the effect is reversed if amount of work exceeds the individual’s capacity. Increased belief in academic achievement being important for the respondents’ social status, predicts increased usage of OTC analgesics. Belief in sport achievement to important for social status and academic ambitions, is found to have conflicting result depending on whether the model is multivariate or univariate. In a univariate setting these variables have a positive effect on usage and vice versa under a multivariate setting.
Table 8 reports the predicted response probabilities for each frequency of OTC analgesic usage across gender-based on both univariate and multivariate regression results. Response probability is plotted against frequency of OTC analgesic usage in Figure 3. As observed, based the univariate regression results, there is a noticeable difference across all level of usage between the genders. The largest discrepancy is related to those who report to never use OTC analgesics. For females and males, the response probability is 25.97% and 45.43%
Table 8. Response probabilities.
Predicted response probabilities derived by using regression results from Table 1 and Table 6 using Equation (4). Sample averages, unconditional on gender, is used as input for the response probabilities derived from multivariate regression results.
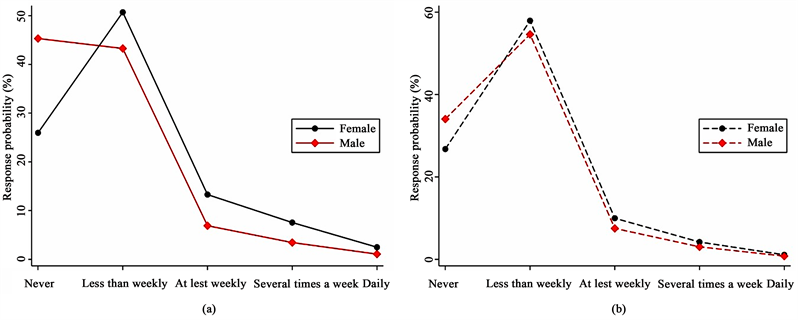
Figure 3. Response probabilities. (a) Univariate; (b) Multivariate.
respectively. The smallest difference in probability is found for the highest frequency of usage. Here, the difference is only 1.43 percentage-points. Interestingly, when adding control variables (see Table 5 and Table 6) most of the gender-based difference evaporates.
4. Discussion and Conclusions
Usage of over-the-counter (OTC) analgesics has been documented to be both high and on an increasing trend. Another stylized fact shows that usage among females is considerably higher compared to males. It is, however, not clear what is driving this gender-based difference.
Using a large dataset of 284,674 observations of Norwegian adolescents attending junior high school and high school between 2014 and 2017, we investigate the prevalence of gender differences in usage of OTC analgesics. In a univariate setting, regressing only usage on a dichotomous gender variable, we find that females tend to have a significantly higher level of consuming OTC analgesics. Expanding the list of potential determinants, physical and mental health problems and sociodemographic variables are found to have a significant effect. Summary statistics show that females tend to score higher on several variables that predict higher usage. Consequently, when controlling for these differences, most of the observed gender difference in OTC analgesic usage evaporates. While reduced, the effect of gender remains significant. Hence, some of the gender-based difference is still unexplained. Furthermore, goodness of fit statistics from our multivariate model suggests that there are additional determinants to be found. We leave these issues to further research.
Acknowledgements
We would like to thank all the adolescents for participating and the NSD for providing authors access to the Ungdata survey.
Conflicts of Interest
No conflict of interest.
Cite this paper
Lorentzen, S., Lorentzen, B. and Wikström, B.-M. (2018) Gender Differences in Usage of Over-the-Counter Analgesics among Norwegian Adolescents. Open Journal of Nursing, 8, 860-878. https://doi.org/10.4236/ojn.2018.811065
References
- 1. Du, Y. and Knopf, H. (2009) Self-Medication among Children and Adolescents in Germany: Results of the National Health Survey for Children and Adolescents (KiGGS). British Journal of Clinical Pharmacology, 68, 599-608. https://doi.org/10.1111/j.1365-2125.2009.03477.x
- 2. Skarstein, S., Lagerløv, P., Kvarme, L.G. and Helseth, S. (2016) High Use of Over-the-Counter Analgesic; Possible Warnings of Reduced Quality of Life in Adolescents—A Qualitative Study. BMC Nursing, 15, 16. https://doi.org/10.1186/s12912-016-0135-9
- 3. Skarstein, S., Rosvold, E.O., Helseth, S., Kvarme, L.G., Holager, T., Småstuen, M.C. and Lagerløv, P. (2014) High Frequency Use of Over-the-Counter Analgesics among Adolescents: Reflections of an Emerging Difficult Life, a Cross Sectional Study. Scandinavian Journal of Caring Sciences, 28, 49-56. https://doi.org/10.1111/scs.12039
- 4. Hasseleid, S.N., Clench-Aas, J., Raanaas, R.K. and Lundqvist, C. (2017) The Association between Adolescent and Parental Use of Non-Prescription Analgesics for Headache and Other Somatic Pain—A Cross-Sectional Study. Scandinavian Journal of Pain, 16, 114-121. https://doi.org/10.1016/j.sjpain.2017.04.069
- 5. Hansen, D.L., Hansen, E.H. and Holstein, B.E. (2008) Using Analgesics as Tools: Young Women’s Treatment for Headache. Qualitative Health Research, 18, 234-243. https://doi.org/10.1177/1049732307312303
- 6. Turunen, J.H., Mäntyselkä, P.T., Kumpusalo, E.A. and Ahonen, R.S. (2005) Frequent Analgesic Use at Population Level: Prevalence and Patterns of Use. Pain, 115, 374-381. https://doi.org/10.1016/j.pain.2005.03.013
- 7. Levin, K.A., Whitehead, R., Andersen, A., Levin, D., Gobina, I. and Holstein, B. (2014) Changes in the Association between Health Complaint Frequency and Medicine Use among Adolescents in Scotland between 1998 and 2010. Journal of Psychosomatic Research, 78, 371-376. https://doi.org/10.1016/j.jpsychores.2014.12.006
- 8. Miech, R., Bohnert, A., Heard, K. and Boardman, J. (2012) Increasing Use of Nonmedical Analgesics among Younger Cohorts in the United States: A Birth Cohort Effect. Journal of Adolescent Health, 52, 35-41. https://doi.org/10.1016/j.jadohealth.2012.07.016
- 9. Bakken, A. (2017) Ungdata 2017 Nasjonale resultater. Norwegian Social Research. https://file:///C:/Users/Bruker/AppData/Local/Packages/Microsoft.MicrosoftEdge_8wekyb3d8bbwe/TempState/Downloads/Opprettet-Ungdata-rapport-2017-4-august-2017-webutg-med-omslag%20(1).pdf
- 10. Dale, O., Borchgrevink, P.C., Fredheim, O.M.S., Mahic, M., Romundstad, P. and Skurtveit, S. (2015) Prevalence of Use of Non-Prescription Analgesics in the Norwegian HUNT3 Population: Impact of Gender, Age, Exercise and Prescription of Opioids. BMC Publichealth, 15, 461. https://doi.org/10.1186/s12889-015-1774-6
- 11. Lagerløv, P., Holager, T., Helseth, S. and Rosvold, E.O. (2009) Selvmedisinering med reseptfrie smertestillende legemidler hos 15-16-åringer. Tidsskrift for Den norske Legeforening, 129, 1447-1450. https://doi.org/10.4045/tidsskr.09.32759
- 12. Sakshaug, S., Strøm, H., Berg, C., Blix, H.S., Litleskare, I. and Granum, T. (2017) Drug Consumption in Norway 2012-2016. Norwegian Institute of Public Health, Oslo. https://www.fhi.no/contentassets/0a8afbeb4c904d14b7b8a773bc25766e/legemiddelforbruket-2012-2016.pdf
- 13. Gualano, M.R., Bert, F., Passi, S., Stillo, M., Galis, V., Manzoli, L. and Siliquini, R. (2014) Use of Self-Medication among Adolescents: A Systematic Review and Meta-Analysis. The European Journal of Public Health, 25, 444-450. https://doi.org/10.1093/eurpub/cku207
- 14. Shehnaz, S.I., Agarwal, A.K. and Khan, N. (2014) A Systematic Review of Self-Medication Practices among Adolescents. Journal of Adolescent Health, 55, 467-483. https://doi.org/10.1016/j.jadohealth.2014.07.001
- 15. Roberts, E., Nunes, V.D., Buckner, S., Latchem, S., Constanti, M., Miller, P. and Dziedzic, K. (2015) Paracetamol: Not as Safe as we Thought? A Systematic Literature Review of Observational Studies. Annals of the Rheumatic Diseases, 75, 552-559.
- 16. Haga, C., Muan, B., Cheung, M., Lyngra, M., Strømsæter, C.E., Lutro, O. and Andrew, E. (2011) Paracetamol for gift ninger eter innføring av ny salgsordning. Tidsskrift for Den norske Legeforening, 131, 2115-2118.
- 17. Vaja, R. and Ghuman, N. (2015) Drugs and the Liver. Anaesthesia & Intensive Care Medicine, 16, 30-34. https://doi.org/10.1016/j.mpaic.2014.10.011
- 18. Bjarnason, I., Scarpignato, C., Holmgren, E., Olszewski, M., Rainsford, K.D. and Lanas, A. (2017) Mechanisms of Damage to the Gastrointestinal Tract from Nonsteroidal Anti-Inflammatory Drugs. Gastroenterology, 154, 500-514. https://doi.org/10.1053/j.gastro.2017.10.049
- 19. Jazbar, J., Locatelli, I., Horvat, N. and Kos, M. (2017) Clinically Relevant Potential Drug-Drug Interactions among Outpatients: A Nationwide Database Study. Research in Social and Administrative Pharmacy, 14, 572-580. https://doi.org/10.1016/j.sapharm.2017.07.004
- 20. Yeomans, N.D., Graham, D.Y., Husni, M.E., Solomon, D.H., Stevens, T., Vargo, J. and Libby, P. (2018) Randomised Clinical Trial: Gastrointestinal Events in Arthritis Patients Treated with Celecoxib, Ibuprofen or Naproxen in the PRECISION Trial. Alimentary Pharmacology & Therapeutics, 47, 1453-1463. https://doi.org/10.1111/apt.14610
- 21. Wood, D.M., Monaghan, J., Streete, P., Jones, A.L. and Dargan, P.I. (2006) Fatality after Deliberate Ingestion of Sustained-Release Ibuprofen: A Case Report. Critical Care, 10, R44. https://doi.org/10.1186/cc4850
- 22. Arfè, A., Scotti, L., Varas-Lorenzo, C., Nicotra, F., Zambon, A., Kollhorst, B. and Schade, R. (2016) Non-Steroidal Anti-Inflammatory Drugs and Risk of Heart Failure in Four European Countries: Nested Case-Control Study. BMJ, 354, i4857. https://doi.org/10.1136/bmj.i4857
- 23. Reed, G.W., Abdallah, M.S., Shao, M., Wolski, K., Wisniewski, L., Yeomans, N. and Nissen, S.E. (2018) Effect of Aspirin Coadministration on the Safety of Celecoxib, Naproxen or Ibuprofen. Journal of the American college of Cardologi, 71, 1741-1751. https://doi.org/10.1016/j.jacc.2018.02.036
- 24. Richardson, J. and Holdcroft, A. (2009) Gender Differences and Pain Medication. Women’s Health, 5, 79-88. https://doi.org/10.2217/17455057.5.1.79
- 25. Abel, C., Johnson, K., Waller, D., Abdalla, M. and Goldsmith, C.A.W. (2012) Nonprescription Medication Use and Literacy among New Hampshire Eighth Graders. Journal of the American Pharmacists Association, 52, 777-782. https://doi.org/10.1331/JAPhA.2012.11158
- 26. Holmström, I.K., Bastholm-Rahmner, P., Bernsten, C., Röing, M. and Björkman, I. (2014) Swedish Teenagers and Over-the-Counter Analgesics-Responsible, Casual or Careless Use. Research in Social and Administrative Pharmacy, 10, 408-418. https://doi.org/10.1016/j.sapharm.2013.06.004
- 27. Wilson, K.M., Singh, P., Blumkin, A.K., Dallas, L. and Klein, J.D. (2010) Knowledge Gaps and Misconceptions about Over-the-Counter Analgesics among Adolescents Attending a Hospital-Based Clinic. Academicpediatrics, 10, 228-232. https://doi.org/10.1016/j.acap.2010.04.002
- 28. Lee, C.H., Chang, F.C., Hsu, S.D., Chi, H.Y., Huang, L.J. and Yeh, M.K. (2017) Inappropriate Self-Medication among Adolescents and Its Association with Lower Medication Literacy and Substance Use. PLoS ONE, 12, e0189199. https://doi.org/10.1371/journal.pone.0189199
- 29. Andersen, A., Holstein, B.E., Berntsson, L. and Hansen, E.H. (2012) Parental Symptoms and Children’s Use of Medicine for Headache: Data Reported by Parents from Five Nordic Countries. International Journal of Public Health, 57, 217-223. https://doi.org/10.1007/s00038-011-0284-2
- 30. Bäckryd, E. (2018) Gender Differences in Dispensed Analgesics in Sweden during 2006-2015 an Observational, Nationwide, Whole-Population Study. International Journal of Women’s Health, 10, 55-64. https://doi.org/10.2147/IJWH.S142052
- 31. Jensen, J.F., Gottschau, M., Siersma, V.D., Graungaard, A.H., Holstein, B.E. and Knudsen, L.E. (2014) Association of Maternal Self-Medication and Over-the-Counter Analgesics for Children. Pediatrics, 133, e291-e298. https://doi.org/10.1542/peds.2013-1107
- 32. Wooldridge, J.M. (2010) Econometric Analysis of Cross Section and Panel Data. 2nd Edition, The MIT Press, Cambridge.
Appendix
Table A1. Physical health problem variables (Section 3.2 Table 3).
Table A2. Depression and anxiety variables (Section 3.2 Table 4 and Table 5).
Table A3. Other variables (Section 3.3 Table 6 and Table 7).
NOTES
1“(A part of) the data that is used here is obtained from “Ungdata 2010-2016”. The survey is financed by the Norwegian Directorate of Health, the Ministry of Justice and Public Security, the Ministry of Children, Equality and Social Inclusion and the Ministry of Education and Research. Data in anonymised form is made available by NOVA through NSD―Norwegian Centre for Research Data A. Neither NOVA, the Norwegian Directorate of Health, the Ministry of Justice and Public Security, the Ministry of Children, Equality and Social Inclusion and the Ministry of Education and Research nor NSD are responsible for the analysis of the data, or the interpretations that are done here.”
2Gender is self-reported and allows only for a binary response―either “boy” or “girl”―in the survey.
3The scale is opposite in this question. A lower score is associated with higher frequency of conflicts with parents.