Open Journal of Nursing
Vol. 3 No. 8A (2013) , Article ID: 41433 , 6 pages DOI:10.4236/ojn.2013.38A008
Unfavorable staffing and resources adequacy impact on patient outcomes and quality of care in the three university hospitals in Malaysia
![]()
1Department of Nursing, Faculty of Medicine, Universiti Kebangsaan Malaysia Medical Centre, Kuala Lumpur, Malaysia
2Faculty of Nursing, Chiang Mai, Thailand
Email: *mzie@ppukm.ukm.edu.my
Copyright © 2013 Maziah Marzuki et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received 23 October 2013; revised 25 November 2013; accepted 6 December 2013
Keywords: Patient Outcomes; Adverse Events; Nursing Quality; Nursing Practice Environment; Staffing and Resources Adequacy
ABSTRACT
The nursing shortage is a global issue that because there is a growing consensus that identifying flaws and opportunities for improving the working environment in hospital is vital to maintain positive patient outcomes, adequate staffing, high-quality care, nurses’ job satisfaction and hence their retention. The aim of this study was to explore the staffing and resource adequacy in NPE and the association with POs (adverse events). A descriptive correlational study was conducted and participated 395 staff nurses (94.3%) from three university hospitals in Malaysia over two months, from January to February 2011. In this paper, the results showed that 344 (87.1%) staff nurses rated that was unfavorable ( < 2.50) of “staffing and resources adequacy” in their nursing environment. The findings also indicated a significant negative association between “enough time and opportunity to discuss patient care problems with other staff nurses” and “patient falls” (p = 0.017), and medication errors (p = 0.027), and patient complaints (p = 0.021). In conclusion, adequate staffing and resources remain as an essential aspect in the working environment and thus, this study recommended that management would be well advised to deal with this aspect of creation of healthy work environments to worth the effort to maintain positive patient outcomes, adequate staffing and high quality care.
< 2.50) of “staffing and resources adequacy” in their nursing environment. The findings also indicated a significant negative association between “enough time and opportunity to discuss patient care problems with other staff nurses” and “patient falls” (p = 0.017), and medication errors (p = 0.027), and patient complaints (p = 0.021). In conclusion, adequate staffing and resources remain as an essential aspect in the working environment and thus, this study recommended that management would be well advised to deal with this aspect of creation of healthy work environments to worth the effort to maintain positive patient outcomes, adequate staffing and high quality care.
1. INTRODUCTION
To date, the nursing shortage has been debated as a shortage in a number of nurse scientists who are developing the science and are crucial for improving the quality of care, who transform knowledge to guide practice; and who make certain that science affects policy changes that can translate to nursing care [1]. It is not only more nurses are required, but it also includes enough resources with more science in complex healthcare systems which are significant in the ongoing pursuit to attain cost-effective [1], high quality nursing care [1], high job satisfaction [2] and positive patient outcomes [3,4].
In healthcare system which consists of healthcare managers, policy-makers and regulators and healthcare professionals that show that healthcare is complex and patient outcomes is possible various along with is influenced by many factors. Nurses also as one of the largest health professional groups in the healthcare system are taking part in an essential role in the delivery of health care services, influencing the patient health and wellbeing [5-7]. In fact, the quality of care is strongly associated with the well-being and job-satisfaction among health care team [2]. Meanwhile job satisfaction emerges among other stuffs from the perception of resources allocated for caring and the care quality within the division [8].
We should concern that health care team should provide services to patients, however there is an alarming issue worldwide, a true story as well as a sad fact that health care itself is able to truly harm the people. Healthcare has actually been a complex process, and thus patient outcomes which can be threatened may not be shocking. It was not surprising when statistics showed 2572 cases of medication errors per 33,945 in-patient admissions a year were reported in 142 hospitals in Malaysia [9]. As health care providers, patient outcomes (POs) should be aimed as a major concern which we need to minimize patients’ may experience harm once they are being treated and cared for [10]. Therefore, this shows that adequate staffing and resources are important to provide high quality patient care, recruit and manage workload, enough time and opportunity to discuss patient care problems with other staff nurses, adequate support services that allow nurses to spend time with their patients and enough staff to get the work done on time [11].
Staffing and resources adequacy refers to having adequate number of staff and support resources to provide quality patient care, which has two key components for providing quality patient care that are 1) being able to spend time with patients; and 2) being able to discuss patient care problems with other nurses [11]. This means that enough staffing is vital for an organizational human resource in which nurses were able to contribute to effective patient care as well as to be a predictor of nurse job satisfaction [5,6,12,13]. Otherwise, inadequate nurse staffing levels would interfere nurses’ capability to properly manage patient care requires and these are a source of nurse frustration, heavier workloads and job dissatisfaction [7,12,14]. Besides, poor nurse staffing levels have also been associated with increased risk for poor patient health, increasing the risk of inpatient complications, inpatient complaints, patient mortality and patient morbidity [5,6,15]. Therefore, comprehensively complete care and effective intervention are requirements in between the hospitals that should carefully plan and manage the structure of care for instance, the ratio of registered nurses in the staff mix, and practice use of care maps to minimize adverse events [16].
A study by Chiang and Lin (2008) [17] revealed that nurses reported least agreement that their nursing practice environment had enough number of staffing and resources ( = 2.35). Similarly, a study by Friese et al. (2008) [18] showed that nurses rated their hospital as unfavorable NPE due to the wards having an inadequate number of staffing and resources which represent 12 hospitals in Pennsylvania. Besides, a retrospective study was conducted to examine the impact of hospital nursing care on 30 day mortality for acute medical care in Ontarion, Canada. The findings showed that lower 30-day mortality rates were related to hospitals that had a higher percentage of registered nurse staff and higher nurses’ perceived staffing and resource adequacy [16]. A study that uses multiple regression tests also revealed that nurses reported staffing and resource adequacy were important predictors of job satisfaction [19].
= 2.35). Similarly, a study by Friese et al. (2008) [18] showed that nurses rated their hospital as unfavorable NPE due to the wards having an inadequate number of staffing and resources which represent 12 hospitals in Pennsylvania. Besides, a retrospective study was conducted to examine the impact of hospital nursing care on 30 day mortality for acute medical care in Ontarion, Canada. The findings showed that lower 30-day mortality rates were related to hospitals that had a higher percentage of registered nurse staff and higher nurses’ perceived staffing and resource adequacy [16]. A study that uses multiple regression tests also revealed that nurses reported staffing and resource adequacy were important predictors of job satisfaction [19].
A study was conducted on nurses’ perception using the nursing practice environment (NPE) model which is defined as an essential environmental condition that can facilitate or constrain professional nursing practice from delivering care to patients. The NPE model was chosen in this study for the reason that the domain contained in this model had characteristics of an establishing a healthy work environment [11]. Moreover, staff nurses who perceived that their wards had a positive or healthy practice environment were more committed to the organization, were more satisfied, can create a culture of safety and were competent to provide the highest quality of care [20]. The NPE model can also change nurses’ practice setting as well as a mechanism for improving POs, along with tackle flaw inside the NPE. In Malaysian university hospitals (UHs), statistic revealed that patient falls in the NPE is 52 cases out of 2672 patients in 2009 [21]. Additionally, concerning the issue of insufficient staff nurse and patient ratio that may contribute to staff nurses working extra time, thus having less time to focus on care, to complete documentation and paperwork is time consuming too. Recently scenario of skill mix nursing-staffing in UHs is 1: 1 or 2 patients in ICU, 1: 8 - 10 patients in general wards, and 1: 1 - 4 patients at the High Dependency Unit (HDU). This situation is contrasted with recommendation of skill mix nursing staffing by WHO that is 1: 4 to 5 patients in medical-surgical unit, rehabilitation unit and general wards, 1: 1 patient in the operating room, and 1: 1 patient in the critical nursing department [22]. Therefore, the aim of this study is to explore the staffing and resource adequacy in NPE and the association with POs (adverse events).
2. METHODOLOGY
This descriptive correlational study was designed to explore the correlation between staffing and resource adequacy and the incidence of adverse events. The study was participated 395 staff nurses (94.3% response rate) from three university hospitals in Malaysia over two months, from January to February 2011, which means, the highest response rate could be generalized the results in the study population. The approval to conduct the study was obtained from the Institute Review Board, Chiang Mai University and the Medical Research and Ethics Committee of UKMMC, HUSM and UMMC (Project Code No. FF-017-2011).
Stratified random sampling method was used and consisting of staff nurses from eight departments: 1) critical nursing, 2) pediatric nursing, 3) psychiatric nursing, 4) emergency/orthopedic nursing, 5) operating room/oncology, 6) surgical/ophthalmology/ENT, 7) obstetrics and gynecology, and 8) medical nursing department in each university hospital. Confidentiality was maintained throughhout the study.
Data was collected using a self-rated 42 items questionnaire and subjects were given two days to complete the questionnaire. The questionnaire consisted of five domains comprising 1) nurse participation in hospital affairs; 2) nursing foundation for quality of care; 3) nurse manager ability, leadership & support of nurses; 4) staffing and resources adequacy; and 5) collegial nurse-physician relationship. The Practice Environment Scale of the Nursing Work Index (PES-NWI), from NPE’s model [11] was used to explore the staffing and resources adequacy in NPE and the association with POs (adverse events). Patient outcomes measured based on nursingsensitive indicators to assess outcomes sensitive to nursing care that used patient falls, medication errors, nosocomial infections and patient complaints as indicators to measure adverse events in this study [23]. The interpretation for each domain in the NPE model indicated that if the mean score was >2.50, it would mean favorable and high agreement and satisfaction. However, if the mean score was <2.50 it would mean unfavorable, and low agreement and satisfaction.
The researcher translated the PES-NWI into the Malaysian language and requested help from bilingual experts (two Malaysian nursing experts who are able to read and write in Malay and English) to translate the translated instrument (Malay version) back into the English version using back translation technique. Validity and reliability of the instruments were tested. The Cronbach Coefficient alpha of the instruments was 0.89 and 0.81 for POs. The data were entered and analyzed using descriptive statistics and Spearman’s rank-order Correlation through the Statistical Package for Social Science (SPSS) software version 12.0.
3. RESULTS
Table 1 showed the frequency, mean scores and standard deviation on domains of NPE which regards to exploring nursing environment as perceived by nurses. The highest score staff nurses’ rated that was unfavorable ( < 2.50) was “staffing and resources adequacy”, which means 344 (87.1%) staff nurses were the lowest agreement and satisfactory on “adequate staffing and resources” in NPE. Whereas, most staff nurses, 348 (87.8%) were reported “nursing foundations for quality of care” that was favorable (
< 2.50) was “staffing and resources adequacy”, which means 344 (87.1%) staff nurses were the lowest agreement and satisfactory on “adequate staffing and resources” in NPE. Whereas, most staff nurses, 348 (87.8%) were reported “nursing foundations for quality of care” that was favorable ( > 2.50), which means staff nurses were high agreement and satisfactory on “nursing foundations for quality of care”.
> 2.50), which means staff nurses were high agreement and satisfactory on “nursing foundations for quality of care”.
Table 2 shows the frequency on each characteristic explaining staffing and resource adequacy in NPE as staff nurses were reported about their nursing environment. A majority, 300 (76.0%) staff nurses’ rated that were the lowest agreement and satisfactory regarding adequate staffing and resources. The highest agreement and satisfaction perceived by staff nurses, 110 (27.9%) were on statement “adequate support services allow me to spend time with my patients”. The lowest agreement and satisfaction perceived by staff nurses, 297 (75.2%) were on statement “enough staff nurses to provide quality
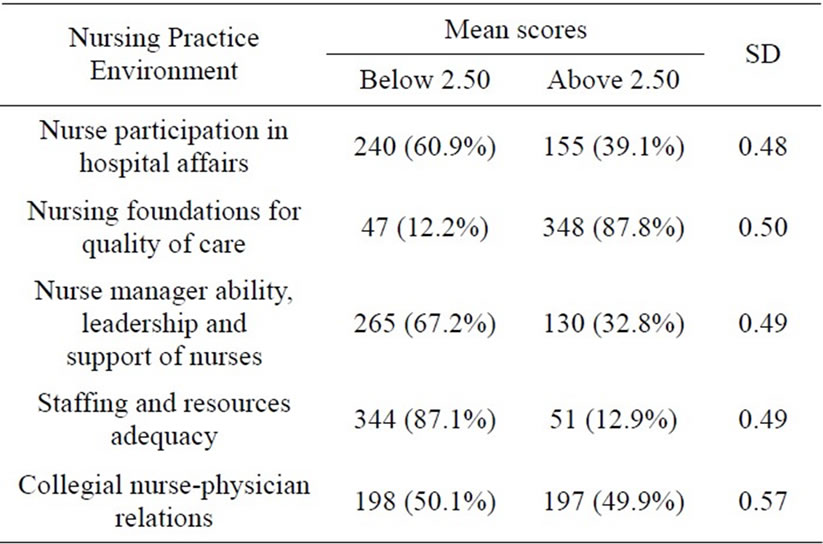
Table 1. Nurses’ score on nursing practice environment (n = 395).
patient care”. The other “staffing and resources adequacy” that staff nurses perceived disagreement and dissatisfaction were on statement “enough time and opportunity to discuss patient care problems with other staff nurses” and “enough staff to get the work done”.
Table 3 shows the correlation between each item in “staffing and resources adequacy” and the incidence of adverse events in the three university hospitals. The findings revealed a weak level of significant negative association between “enough time and opportunity to discuss patient care problems with other staff nurses” and “patient falls” (p = 0.017, r = −0.120), and medication errors (p = 0.027, r = −0.111), and patient complaints (p = 0.021, r = −0.116) which means, more time and the highest opportunity to discuss patient care problems with other staff nurses (having adequate staffing) could decrease patient falls, medication errors and patient complaints. The findings also indicated a weak level of significant negative association between hospital and “patient falls” (p = 0.037, r = −0.105), and “patient complaints” (p = 0.034, r = −0.106) as well as a negative association between ward of work and patient falls (p = 0.000, r = −0.216) and patient complaints (p = 0.005, r = −0.196). This was meant that the best planning and the best standard manage the structure of care by organizational human resource in the university hospitals and in the ward of work at the university hospitals could minimize patient falls and patient complaints.
Table 4 shows the frequency of patient outcomes as perceived by staff nurses in the three university hospitals. The highest adverse event as reported by staff nurses was patient complaints that were 54 (44.26%) cases. The lowest adverse event as reported by staff nurses was patient falls and medication errors that were 18 (14.75%) cases.
4. DISCUSSION
The four main findings from this study are: 1) the highest

Table 2. Frequency on staffing and resource adequacy as perceived by staff nurses (n = 395).
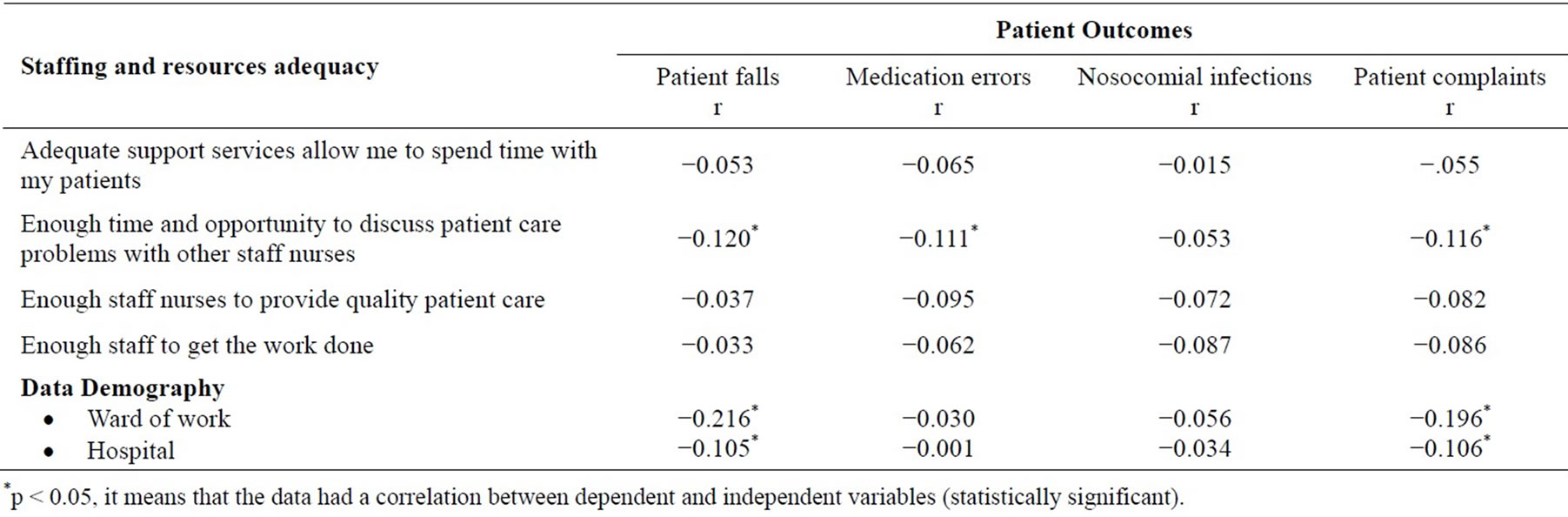
Table 3. Spearman rank correlation coefficient between each item in staffing and resource adequacy and patient outcomes.
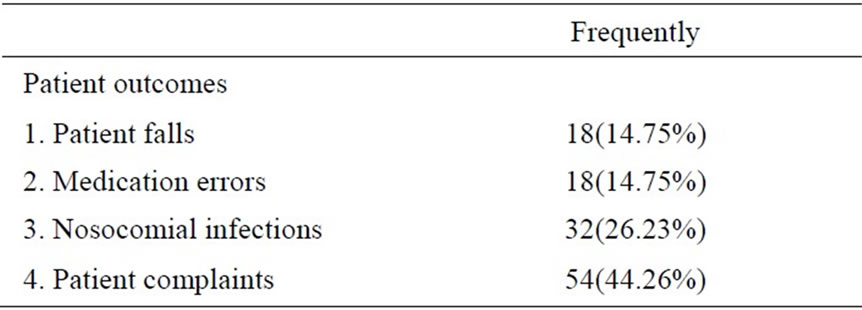
Table 4. Staff nurses’ report on patient outcomes (n = 395).
score was unfavorable on staffing and resources adequacy; 2) the highest disagreement and dissatisfaction among staff nurses were “enough staff nurses to provide quality patient care”; 3) “enough time and opportunity to discuss patient care problems with other staff nurses” had significantly associated with “patient falls, medication errors and patient complaints” for staff nurses working in the university hospitals; and 4) patient complaints were the highest adverse event as reported by staff nurses. The possible explanations for the above results are discussed.
Despite various characteristics of NPE, inadequate staffing and resources remained the main issue in the nurses’ practice environment. This finding was similar with Chiang and Lin’s (2008) [17] study revealed that nurses reported least agreement that their nursing practice environment had enough number of staffing and resources ( = 2.35). Consistently, a study by Friese et al. (2008) [18] showed that nurses rated their hospital as unfavorable NPE due to the wards having an inadequate number of staffing and resources which represent 12 hospitals in Pennsylvania. Besides, a study that uses multiple regression tests also revealed that nurses reported staffing and resource adequacy were important predictors of job satisfaction [19].
= 2.35). Consistently, a study by Friese et al. (2008) [18] showed that nurses rated their hospital as unfavorable NPE due to the wards having an inadequate number of staffing and resources which represent 12 hospitals in Pennsylvania. Besides, a study that uses multiple regression tests also revealed that nurses reported staffing and resource adequacy were important predictors of job satisfaction [19].
The similarities of the above results with previous study may be explained as staff nurses working in university hospitals actually having a lot of work that should be done on time (within a working shift). University hospitals refer to educational institutions that conduct education and training to the Malaysian population and provide tertiary level services for the three functions: human resources development, research, and healthcare services with the motto of integrating education and research for society. Staff nurses as the largest health professional groups in the healthcare system are not taking part in a vital role in the delivery of health care services or promote the patient health and wellbeing only, but they also involved in research and participated as a part of role in organizational management for example, involved in quality activities such as accreditation, quality assurance (QA) project, International Standardization Organization (ISO) certificate programs, quality control (QC) project and work innovation group (KIK) project. Staff nurses always involved with those activities that the activities may contribute to a lot of paperwork and documentation needs to be complete.
In addition, skill mix nursing-staffing at university hospitals is high that is 1: 1 or 2 patients in ICU, 1: 8 - 10 patients in general wards, and 1: 1 - 4 patients at the High Dependency Unit (HDU) and this situation is contrasted with there commendation of skill mix nursing staffing by WHO, which is 1: 4 to 5 patients in medical-surgical unit, rehabilitation unit and general wards, 1: 1 patient in the operating room, and 1: 1 patient in the critical nursing department [22]. As a result, this condition may contribute to sometimes staff nurses need to work extra time/double shift and float at other wards, staff nurses are unable to manage their work properly because of inadequate staff to complete paperwork as well as documentation needed and subsequence with delivering care to patients. The conditions are worse especially when there are many emergency cases or when someone (clerk, staff nurses or attendant) is on sick leave, emergency leave, wedding leave or confinement leave and this may also contribute to nurses experiencing long working hours, staff nurses working more than 7 hours [24]. According to Rogers et al. (2004) [25], hospitals occurred adverse events are more likely when hospital registered nurses work that either twelve or more hours at a stretch.
We should concern with those issues and as evidence, this study shows that staff nurses perceived was unfavorable of staffing and resource adequacy in the three university hospitals, that 344 (87.1%) where the highest disagreement and dissatisfaction with “staffing and resources adequacy” in their nursing environment. In achieving cost-effective [1], high quality nursing care [1], high job satisfaction [2] and positive patient outcomes [3,4], each hospital should require carefully plan and manage the structure of care by following skill mix nursing-staffing as WHO recommendation [22] and practice use of care maps to minimize adverse events [16]. Besides, adequate staffing and resources remains as the important predictors of job satisfaction [19] and thus, inadequate nurse staffing levels as showed in this study, this would interfere nurses’ capability to properly manage patient care requires and these are a source of nurse frustration, heavier workloads and job dissatisfaction [7,12,14].
The findings also indicated that “enough time and opportunity to discuss patient care problems with other staff nurses” had significantly associated with “patient falls (p = 0.017, r = −0.120), medication errors (p = 0.027, r = −0.111) and patient complaints” (p = 0.021, r = −0.116) for staff nurses working in the university hospitals. It was similar to findings from a study by Tourangeau et al. (2007) [16] showed that lower 30-day mortality rates were associated with hospitals that had a higher percentage of registered nurses in acute medical care (p = 0.02) and higher nurses’ perceived having “enough time and opportunity to discuss patient care problems with other staff nurses” (p = 0.04). This means that having adequate staffing would give more time and the highest opportunity for staff nurses to discuss patient care problems with other staff nurses that could decrease patient falls, medication errors and patient complaints in the same time. Therefore, the highest level of nursing management such as Nurse Directors, Nurse Managers or Head Nurses should have good strategic planning in skill mix nursing-staffing and adequate resources to get work done completely. Besides, hospital and unit leadership should also monitor the nursing work environment and job demands aspects through staff surveys may provide enough job resources to predict the feelings of burnout, may provide a feasible of identifying chances of sustaining or improving and ensure both its quality and safety of patient care. This is because the supportive management could increase awareness about safe practice among staff nurses in their environment. In addition, we worry that patient safety issues definitely require more attention, immediate action and responsibility from various levels of healthcare team [9] which included staff nurses as the biggest role in providing care to patients.
Moreover, this finding also revealed the quality of patient care is low as a result of the lowest satisfaction of “staffing and resources adequacy” as reported by staff nurses in the university hospitals. According to Hannan et al. (2001) [2], the quality of care is strongly associated with the well-being and job-satisfaction among health care team [2]. Meanwhile job satisfaction emerges among other stuffs from the perception of resources allocated for caring and the care quality within the division [8]. Therefore, improving working conditions in each hospital is important to maintain adequate staffing, the highest care quality, nurses’ job satisfaction and consequently their retention. A similar study by Hinno, Partanen, & Julkunen (2012) [26] showed that favorable of the adequacy of staffing and resources along with management supports were positively correlated with nurse assessed care quality and job-related positive feelings and negatively associated with intentions to leave a unit, organization or the entire profession.
5. CONCLUSION
The findings clearly indicate that staff nurses perceived that their practice environment in the three university hospitals was unfavorable, which identify negative patient or nurse outcomes and challenging features of everyday practice with inadequate staffing and resources that have emerged appearing to be common to university hospitals. Thus, adequate staffing and resources remain as an important aspect in working condition. The results of this study recommended that management would be well advised to address this aspect of creation of healthy work environments with a good staffing planning; workload planning and management process are able to contribute to desirable outcomes for patients, staff nurses, and/or the system as well as to adapt to the complexities of modern nursing.
6. ACKNOWLEDGEMENT
We would like to thank Universiti Kebangsaan Malaysia for providing the research grant FF-017-2011.
REFERENCES
- Meleis, A.I. (2005) Shortage of nurses means shortage of nurse scientists. Journal of Advanced Nursing, 49, 111.
- Hannan, S., Norman, I.J. and Redfem, S.J. (2001) Care work and quality of care for older people, a review of the research literature. Reviews in Clinical Gerontology, 11, 189-203. http://dx.doi.org/10.1017/S0959259801112104
- Needleman, J., Buerhaus, P., Mattke, S., Stewart, M. and Zelevinsky, K. (2001) Nurse-staffing levels and patient outcomes in hospitals. Harvard School of Public Health, Boston.
- Smith, L.W. and Giuliano, K.K. (2010) Rapid response teams: Improve patient safety and patient outcomes. Journal of Advanced Critical Care, 21, 126-129. http://dx.doi.org/10.1097/NCI.0b013e3181d24676
- Tourangeau, A.E. (2005) A theoretical model of the determinants of mortality. Advances in Nursing Science, 28, 58-69. http://dx.doi.org/10.1097/00012272-200501000-00007
- Aiken, L.H., Clarke, S.P., Sloane, D.M., Lake, E.T. and Cheney, T. (2008) Effects of hospital care environment on patient mortality and nurse outcomes. Journal Nursing Administration, 38, 223-229. http://dx.doi.org/10.1097/01.NNA.0000312773.42352.d7
- Duffield, C., Diers, D., O’Berien-Pallas, L., Aisbett, C., Roche, M., King, M. and Aisbett, K. (2011) Nursing staffing, nursing workload, the work environment and patient outcomes. Applied Nursing Research, 24, 244-255. http://dx.doi.org/10.1016/j.apnr.2009.12.004
- Cohen-Mansfield, J. (1995) Stress in nursing home staff, a review and a theoretical model. The Journal of Applied Gerontology, 14, 444-466. http://dx.doi.org/10.1177/073346489501400406
- (2010) Warning on patient safety. New Straits Times, 23.
- Sandars, J. and Cook, G. (2007) ABC of patient safety. Blackwell Publishing, Australia.
- Lake, E.T. (2002) Development of the practice environment scale of the nursing work index. Research in Nursing & Health, 25, 176-188. http://dx.doi.org/10.1002/nur.10032
- Aiken, L.H., Clarke, S.P., Sloane, D., Sochalski, J. and Silber, J.H. (2002) Hospital nurse staffing and patient mortality, nurse burnout, and job satisfaction. JAMA, 288, 1987-1993. http://dx.doi.org/10.1001/jama.288.16.1987
- Bowles, C. and Candela, L. (2005) First job experiences of recent RN graduates. Journal of Nursing Administration, 35, 130-137. http://dx.doi.org/10.1097/00005110-200503000-00006
- Scott, E., Engelke, M. and Swanson, M. (2008) New graduate nurse transitioning: Necessary or nice? Applied Nursing Research, 21, 75-83. http://dx.doi.org/10.1016/j.apnr.2006.12.002
- Unruh, L.Y. and Zhang, N.J. (2012) Nursing staffing and patient safety in hospitals: New variables and longitudinal approaches. Nursing Research, 61, 3-12. http://dx.doi.org/10.1097/NNR.0b013e3182358968
- Tourangeau, A.E., Doran, D.M., Hall, L.M., Pallas, L.O., Pringle, D., Tu, J.V. and Cranley, L.A. (2007) Impact of hospital nursing care on 30-day mortality for acute medical patients. Journal of Advanced Nursing, 57, 32-44. http://dx.doi.org/10.1111/j.1365-2648.2006.04084.x
- Chiang, H.-Y. and Lin, S.-Y. (2008) Psychometric testing of the Chinese version of nursing practice environment scale. Journal of Clinical Nursing, 18, 919-929.
- Friese, C. R., Lake, E. T., Aiken, L. H., Jeffrey H. Silber, J. H. and Sochalski, J. (2008) Hospital nurse practice environments on outcomes of surgical oncology patients. Health Services Research, 43, 1145-1163. http://dx.doi.org/10.1111/j.1475-6773.2007.00825.x
- Stam, L.M.P., Laschinger, H.K.S., Regan, S. and Wong, C.A. (2013) The influence of personal and workplace resources on new graduate nurses’ job satisfaction. Nursing Management. http://dx.doi.org/10.1111/jonm.12113
- Laschinger, H.K.S., Finegan, J., Shamian, J. and Casier, S. (2000) Organizational trust and empowerment in restructured healthcare settings: Effects on staff nurse commitment. Journal of Nursing Administration, 30, 413-425. http://dx.doi.org/10.1097/00005110-200009000-00008
- Department of Nursing Service UKMMC (2010) UKMMC and annual report. UKMMC, Cheras.
- World Health Organization (WHO) (2009) The world health report 2009-health system: Improving performance. World Health Organization, Geneva.
- Laschinger, H.K.S. and Leiter, M.P. (2006) The impact of nursing work environments on patient safety outcomes: The mediating role of burnout/ engagement. Journal of Nursing Administration, 36, 259-267. http://dx.doi.org/10.1097/00005110-200605000-00019
- Nursing Management Department UKMMC of Malaysia (2010) UKMMC and annual report. UKMMC, Cheras.
- Rogers, A.E., Hwang, W., Scott, L.D., Aiken, L.H. and Dinges, D.F. (2004) The working hours of hospital staff nurses and patient safety. Health Affairs, 23, 202-212. http://dx.doi.org/10.1377/hlthaff.23.4.202
- Hinno, S., Partanen, P. and Julkunen, K.V. (2012) The professional nursing practice environment and nurse-reported job outcomes in two European countries: A survey of nurses in Finland and the Netherlands. Scandinavian Journal of Caring Science, 26, 133-143. http://dx.doi.org/10.1111/j.1471-6712.2011.00920.x
NOTES
*Corresponding author.