Open Journal of Psychiatry
Vol.3 No.4(2013), Article ID:37860,6 pages DOI:10.4236/ojpsych.2013.34042
Taijin-Kyofu-Sho: A subtype of social anxiety
![]()
Department of Psychiatry, Singapore General Hospital, Singapore City, Republic of Singapore
Email: leslie.lim.e.c@sgh.com.sg
Copyright © 2013 Leslie Lim. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received 4 September 2013; revised 2 October 2013; accepted 9 October 2013
Keywords: Taijin-Kyofu-Sho; Social Anxiety Disorder; Cultural Factors; Treatment
ABSTRACT
Taijin-Kyofu-Sho (TKS) has long been considered as a Japanese culture-bound form of social anxiety disorder, although subsequent case-reports from countries outside Japan have dispelled this notion. There are subtle yet distinct differences between TKS and DSM-defined social anxiety disorder (SAD). For instance, the TKS subject fears causing offence to others, whereas the SAD subject is more fearful of causing embarrassment to him/herself. Four sub-categories of TKS have been recognised of which the Jikoshu-kyofu variety resembles the olfactory reference syndrome (ORS) known to Western psychiatrists. There are two TKS subtypes, general (or simple) and offensive (delusional). The general subtype resembles social anxiety disorder, whereas the offensive subtype is characterised by delusions. True community-wide prevalence is unknown, although clinic studies estimate between 7.8% to 45.5% patients have a diagnosis of TKS, with a slight male preponderance. Cultural and societal norms engendering guilt, shame, and embarrassment are likely etiological factors. Treatment may consist of antidepressant and/or antipsychotic medications, while some patients may also benefit from cognitive behavior therapy.
1. INTRODUCTION
Taijin-Kyofu-Sho (TKS) has long been described as a Japanese culture-specific expression of SAD. The term literally means fear (kyofu) of interpersonal relationships (taijin) [1]. It is classified in the DSM-V under social anxiety disorder, and briefly described under culturerelated diagnostic issues [2]. TKS is defined as a persistent and excessive fear of giving offence to others in social circumstances by physical characteristics such as blushing, gaze, or emitting of foul body odor [3,4]. It was first described in Japan by Shoma Morita in the 1920s, and who used Morita Therapy to treat this condition [5].
Following initial descriptions of the condition much interest has been generated over the years as evidenced by a sporadic stream of publications both from East Asian and Western sources. Hence, it might be worthwhile to review the literature and present a succinct summary of the available information on TKS and to clarify similarities and differences between the latter and other related DSM-defined conditions, especially in light of the recently published DSM-V [2].
2. CLINICAL FEATURES
In TKS, the individual fears that his/her own attitudes, behavior, and physical characteristics are cause for offence in social situations. He/she experiences emotional reactions such as shame, embarrassment, anxiety, fear, and is anxious and tense in these situations; and may feel unaccepted, despised, and rejected by others, perceiving that they are trying to avoid him/her [3,6,7].
Owing to fear of rejection, the subject attempts to avoid potentially painful social and interpersonal interactions. Strong anxieties are usually not experienced in the presence of very closely related people, or conversely, complete strangers. Rather, it is in the presence of familiar people that individuals with TKS experience the most anxiety [1,8]. Such settings include places most often frequented by sufferers (e.g. school, work, commuter trains, etc.). Most patients only experience a single circumscribed fear, although the specific focus may change over time. Takahashi has proposed the following diagnostic criteria for TKS [7]. (Please refer to Table 1).
2.1. TKS Subtypes
Researchers have defined TKS as a condition with a wide spectrum of illness severity, from the more prevalent but transient social anxiety to the severe offensive
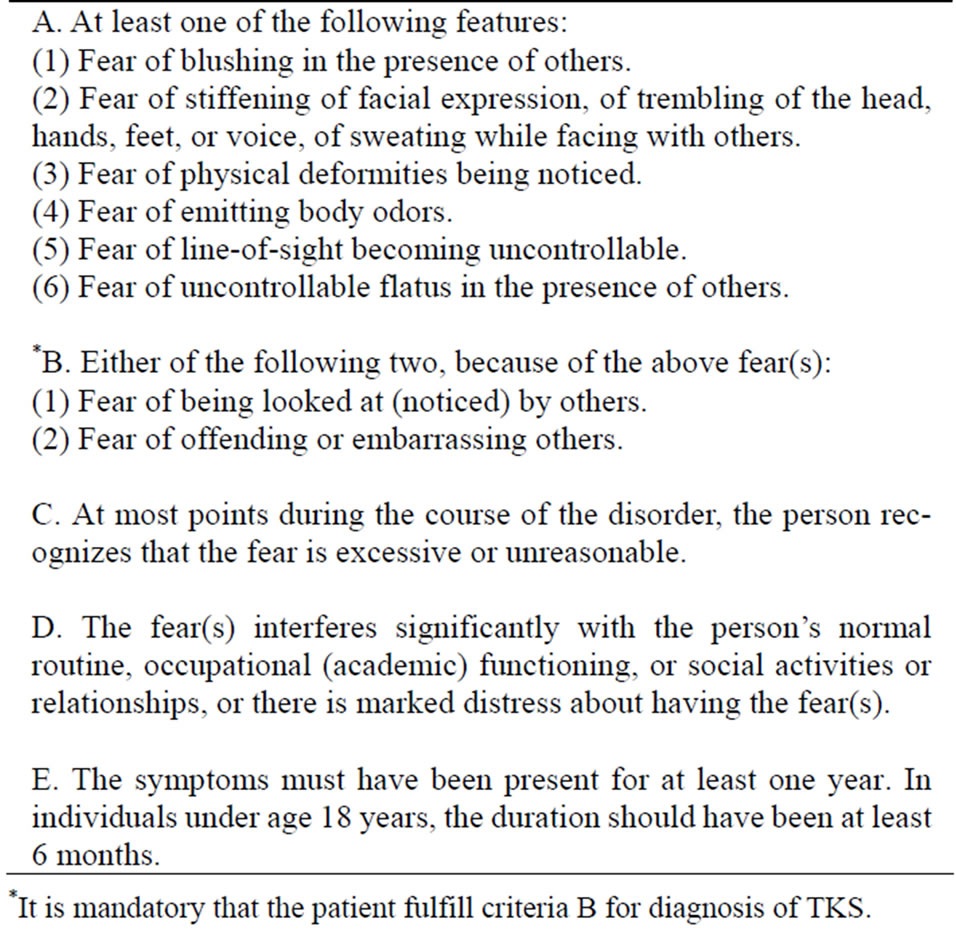
Table 1. Proposed diagnostic criteria for Taijin-Kyofu-Sho (TKS).
*It is mandatory that the patient fulfill criteria B for diagnosis of TKS.
type [8]. Some have suggested that there are two broad subtypes viz. general (or simple) and offensive (delusional).
2.2. General Subtype
It is suggested that the general subtype comprises features that are essentially identical to those of the commonly known social anxiety disorder, including physical symptoms such as blushing and stiff facial expressions, fear of being negatively evaluated by others, and frequent avoidant behaviors in social situations [9]. The DSM-V refers to this as the “sensitive type” with “extreme social sensitivity and anxiety about interpersonal interactions” [2].
2.3. Offensive Subtype
This subtype is well documented and is characterized by delusions including the belief that there is a defect in a particular body part (e.g. eye, face ) or appearance, or the belief that one is emitting body odor [1,9-13]; the belief that one is causing harm to others by his/her physical appearance; or that others are avoiding him/ her [1,11].
In both sensitive and offensive subtypes the recent classification recognises that concerns may include features resembling body dysmorphic disorder (BDD) and delusional disorder [2].
Suzuki has proposed a classification which further divides TKS into four sub-categories [14]:
1) Sekimen-kyofu (the phobia of blushing)
2) Shubo-kyofu (the phobia of a deformed body)
3) Jikoshisen-kyofu (the phobia of eye-to-eye contact)
4) Jikoshu-kyofu (the phobia of one’s own foul body odour)
Of these four subcategories, sekimen-kyofu appears to be most closely associated with the DSM-definition of SAD, whereas shubo-kyofu appears to be most closely associated with BDD [14].
The Western equivalent of Jikoshu-kyofu seems to be that of “Olfactory Reference Syndrome” (ORS) initially described by Pryse-Phillips [15]. ORS sufferers are preoccupied with the fear that their body is emitting a foul odor, thus causing offence to others. These preoccupations lead to “contrite reactions” for example, taking a shower, brushing the teeth, changing the clothes, and using deodorant.
It is uncertain whether ORS is a primary disorder or a component of other psychiatric conditions [16]. As such, ORS is not included in the DSM-IV [17] or DSM-V [2], the rationale being that since there could be overlaps with other established conditions, a new diagnostic category was unnecessary [16].
Whereas Sekimen-kyofu and Shubo-kyofu could be diagnosed as social anxiety disorder and body dysmorphic disorder according to DSM-IV [14,17], Jikoshisenkyofu is a condition with a particular East-Asian bias. This is because Japanese children are taught that making eye contact is rude. Instead, they are taught to fix their gaze at the clavicular level of the people they are speaking to. By contrast, Western culture emphasizes the importance of making eye contact. Conversely, avoidance of eye contact is attributed to shame or insincerity by Westerners [6].
3. DIFFERENTIAL DIAGNOSES
The offensive type could be misdiagnosed with other disorders e.g. body dysmorphic disorder (BDD), paranoid personality, delusional disorder, and even obsessive-compulsive disorder (OCD) [6,18-20]. In the case of BDD, there is a preoccupation in one more perceived defects in one’s physical appearance. These so-called defects do not appear to distress or embarrass the onlooker as much as they do the subject. Conversely, the TKS sufferer is more concerned that his physical characteristics offend others. In the case of OCD, intrusive thoughts, images or impulses compel one to perform a variety of repeated actions (rituals) e.g. checking or washing or cleaning. In view of obsession-like thinking, there are even some who judge ORS to be a variant of obsessive-compulsive disorder [21,22].
ORS has been defined as a psychiatric condition characterized by persistent preoccupation about body odor accompanied by shame, embarrassment, significant distress, avoidance behaviour and social isolation [23]. Defined as a delusional disorder, ORS differs from JKF in that JKF’s broad spectrum stretches from that of social anxiety to delusional disorder (somatic type) [23].
Suzuki et al. compared the features of ORS with those of JKF [23]. They found that the features of both conditions were identical, which suggests that they shared a common clinical entity. This view is also upheld by DSM-V [2]. It has been argued that while the age of onset of ORS (at 25.4 years) was significantly younger than those with schizophrenia and depression, they were older than those with JKF [15]. By contrast, age of onset of JKF was in the teens [23].
Although the preoccupation of most BDD patients is their physical appearance, there is data to indicate that some patients with BDD report obsessional concerns about odor [16]. However, the repetitive behaviors of BDD differ from the obsessions and compulsions of OCD in that BDD subjects are only preoccupied with perceived defects in their appearance [2]. In contrast to OCD, insight appears to be more lacking in BDD [2].
Given the significant overlap between ORS and BDD, Lochner and Stein suggest that ORS could be considered a variant of BDD. In this conceptualization, BDD might share some features of social anxiety disorder, in which symptoms clearly lead to social anxiety and avoidance [16]. But unlike social anxiety disorder the preoccupations of BDD centre on perceived appearance defects [2].
Differences from Social Anxiety Disorder (SAD)
About 10 years ago, it was still uncertain whether TKS and social phobia could be regarded as identical conditions [24]. Although initial reports suggest similarities between the general type and social anxiety disorder, there are subtle yet distinct differences.
The main difference is that the TKS subject fears causing offence to others, whereas the SAD subject fears embarrassing him/herself. This may include showing signs of anxiety, which may result in negative evaluation by others. Therefore, TKS has been described as an allocentric, or other-orientated, disorder and SAD as an egocentric, or self-orientated disorder [18].
The TKS patient is preoccupied about causing offence through appearance, gaze or odor. The SAD patient is fearful of behaving in a manner which would result in embarrassment to him/her while under the scrutiny of others [25]. In TKS, there is a preoccupation with certain body parts but not in the case of social phobia. Specifically, individuals with TKS fear that they may offend others, thereby bringing shame upon their families and friends [1].
It would appear that the TKS definition is more encompassing: not only does the sufferer consider his/her own physical appearance to be offensive to the onlooker, additionally, attitudes and behaviors are also subject to perceived negative appraisal by onlookers. The criteria that one is unaccepted, despised, and avoided by others is a feature of TKS, but not a pre-requisite of SAD [25]. In both conditions there is avoidance of situations where anxieties might arise.
One study comparing social phobia with TKS among a sample of university students in the United States and Japan found an approximate 50% co-occurrence between high scorers on the TKS and social phobia scales. Results suggested that cultural variables mediated the expression of social anxiety disorder and TKS while both disorders could be found in each sample [26].
4. EPIDEMIOLOGY
Community-wide prevalence is still unknown [27]. In Japan, clinic studies have yielded prevalence rates between 7.8% and 45.5% [3]. Individuals who present with clinical symptoms of TKS are predominantly male, although the percentage of female patients in Japan is rising. The male-female ratio is approximately 3:2 [3], whereas in the case of SAD, female preponderance is well established.
Onset of TKS typically occurs during early adulthood [3], or late adolescence, and this may affect the formation of interpersonal relationships, to the detriment of personal growth and development [25].
TKS cases seem to vary on a continuum of severity from the highly prevalent but transient adolescent social concerns to delusions—somatic type, depending on the tenacity and bizarreness of one’s belief that his or her actions or characteristics are offending or damaging to others [3,8,28].
5. IS IT CULTURE-BOUND?
Although TKS was initially judged to be a culture-bound disorder unique to Japan [8,28], evidence is accumulating to suggest that it is not confined to a particular culture or country. For example, similar social avoidant patterns have been reported in Korea [11,29], various European countries [30,31], the United States [15,19, 20,30] and Australia [31], thus dispelling the notion that this is a culture-bound syndrome specific only to Japanese society. More recently, the condition has also been described in Southeast Asia [32,33].
A study by Kleinknecht and colleagues examined differences between SAD and TKS, and their relation to independence and interdependence in US and Japanese university students. Factor analyses yielded three factors, each corresponding to the respective scales defining TKS and SAD. A case analysis indicated an approximate 50% co-occurrence between high scorers on the TKS and SAD scales [26].
A recent study using the TKS questionnaire assessed the allocentric focus of fear in U.S. and Korean patients with DSM-IV diagnosis of social anxiety disorder [12].
The results confirmed that 75% of patients with SAD had at least one of the five offensive TKS symptoms. In both samples, the severity of offensive TKS symptoms was significantly associated with severity of SAD, depressive symptoms, and disability. These results showed that TKS offensive subtype symptoms are not uncommon among U.S. patients with SAD, suggesting that the condition may not be as culturally specific as previously believed.
6. PSYCHOPATHOLOGICAL MECHANISMS
6.1. Embarrassment, Guilt, and Shame
The central feature of SAD (and TKS) is an inordinate fear of violating social norms, resulting in embarrassment to oneself or others. Some researchers have observed that it is easier to embarrass persons from an East Asian culture because there are more rules governing social behaviors there, thus rendering deviations from the norm easier to detect [34]. Others have also suggested that embarrassment is more common in collectivistic societies because it is induced by external sanctions, whereas guilt and self-blame are more common in individualistic cultures because they are induced by internal sanctions [35,36].
6.2. Independence and Interdependence
Markus and Kitayama suggested that individuals from the US and other individualistic societies tend to endorse independence and autonomy from the rest of society [37]. By contrast, people from the East are more likely to embrace interdependence, viewing themselves as being part of a wider social group. To this end, they strive for harmony in interpersonal relationships by being attentive to, and responding to the thoughts, feelings, and behaviors of those whom they are interacting with [37].
Singelis and Sharkey proposed that being interdependent may trigger an acute awareness of the social norms and sensitivity to evaluation by others, while being independent may serve as a protective factor in the face of these evaluations [34].
Similarly, Okazaki suggested that highly interdependent people might be more attuned to social cues and are more likely to experience social anxiety than individuals who score low on this dimension [38]. This hypothesis was confirmed in a study that examined the relationship between self-construals and social anxiety among American and Japanese university students [39].
The concept that shame may play a bigger role in Chinese (as opposed to American) culture was demonstrated in a study examining the cross-cultural differences of the effects of shame and personality on social anxiety [40]. In Japan, shame-prone and self-effacing behavior are highly valued and are actively promoted by society, whereas American culture might tend to prohibit shame-prone behaviors and the expression of one’s vulnerability, while encouraging the visible demonstration of one’s autonomy and capability [40].
Ironically, 12-month rates of DSM-IV social anxiety disorder in the US appear to be the highest in the world at 7.1% [41], almost double that in Europe [42]. In contrast, the 12-month prevalence rate of SAD from East Asian countries has been reported to be much lower, in the range of 0.4% in Taiwan [43], 0.2% - 0.6% in Korea [44], 0.2% in China [45], and 0.8% in Japan [46]. This seems to suggest that while individualism might confer some measure of protection from TKF-type anxieties, they do not necessarily prove advantageous in preventing individuals from developing DSM-defined social anxiety disorder.
7. TREATMENT
TKS appears to respond well to serotonin reuptake inhibitors [13,47,48] and selective serotonin and noradrenaline reuptake inhibitors [49]. It may also respond to psychological treatments, for example, there has been a case report demonstrating efficacy of cognitive behavior therapy in a Jikoshu-kyofu patient whose predominant fear is that of emanating a foul body odor [33].
Morita therapy has been a well established treatment in Japan to treat TKS [1]. Initially formatted as an intensive inpatient treatment, it has since been modified for use in the outpatient setting, in the form of group therapy. There are 2 phases, an intensive phase lasting several months, followed by a working-through phase.
There are elements of behavior therapy such as the use of exposure exercises with the aims of achieving functional improvements, rather than symptom relief. Few controlled trials have been conducted to assess its efficacy.
In the case of the offensive delusional type of disorder, antipsychotic medications are required, although there is a distinct paucity of reports describing the efficacy and tolerability of any particular atypical antipsychotic medication. It has been previously suggested that medications such as pimozide could be effective in some patients with ORS [48]. Some have suggested the use of specific serotonin reuptake inhibitors to treat ORS [22,48] assuming that these symptoms, despite causing distress, have not reached delusional intensity.
8. CONCLUSIONS
Social anxiety is a common symptom/disorder in many countries. While TKS may have been first described in Japan, subsequent research has contradicted earlier assertions that it is a culture-bound phenomenon. Not-withstanding, socio-cultural factors might have facilitated its expression in the East-Asian context. Epidemiological data is still lacking as information is mainly derived from clinical samples.
Perception of societal norms and expectations are likely to play a major role in shaping thinking, emotions and behavior. Shame and collectivism feature prominently in East-Asian societies and are likely predisposing factors. In the West, individualism and autonomy, while seemingly advantageous, may nevertheless not protect one from developing DSM-defined social anxiety disorder. Therefore, a person’s socio-cultural background needs to be carefully taken into consideration when evaluating the origins of their social anxiety. The same social behavior perceived as acceptable in one culture may come across as “unreasonable and excessive” in another.
The expressions of social anxiety are influenced by multiple factors—societal, cultural, gender role, gender role identification, and ideas of shame and embarrassment [50]. While social anxieties in different parts of the world share common features, the expression and experience of anxiety may differ. Fortunately reports of effective pharmacological and psychological treatments are available.
REFERENCES
- Maeda, F. and Nathan, J.H. (1999) Understanding taijin kyofusho through its treatment, Morita Therapy. Journal of Psychosomatic Research, 46, 525-530.
- American Psychiatric Association (2013) Diagnostic and statistical manual of mental disorders, DSM-5. American Psychiatric Publishing, Washington DC.
- Takahashi, T. (1989) Social phobia syndrome in Japan. Comprehensive Psychiatry, 30, 45-52. http://dx.doi.org/10.1016/0010-440X(89)90117-X
- Kleinknecht, R.A., Dinnel, D.L., Tanouye-Wilson, S. and Lonner, W.J. (1994) Cultural variation in social anxiety and phobia: A study of taijin kyofusho. Behaviour Therapist, 17, 175-178.
- Ohara, K., Aizawa, S. and Iwai, H. (1970) Morita therapy. Bunkodo, Tokyo.
- Tanaka-Matsumi, J. (1979) Taijin Kyofusho: Diagnostic and cultural issues in Japanese psychiatry. Culture, Medicine and Psychiatry, 3, 231-245. http://dx.doi.org/10.1007/BF00114612
- Kasahara, Y. (1986) Fear of eye-to-eye confrontation among neurotic patients in Japan. In: Lebra, T.S. and Lebra, W.P., Eds., Japanese Culture and Behavior, University of Hawaii Press, Honolulu, 379-387.
- Kirmayer, L.J. (1991) The place of culture in psychiatric nosology: Taijin Kyofusho and DSM-III-R. Journal of Nervous and Mental Disease, 179, 19-28. http://dx.doi.org/10.1097/00005053-199101000-00005
- Kasahara, Y., Fujinawa, A., Sekiguchi, H. and Matsumoto, M. (1972) Phobias of eye-to-eye confrontation and body odor. Seishi kyofu, taishu kyofu. Igakushoin, Tokyo. (in Japanese)
- Iwase, M., Nakao, K., Takahashi, J., Yorifuji, K., Ikezawa, K. and Takeda, M. (2000) An empirical classification of social anxiety: Performance, interpersonal and offensive. Psychiatry and Clinical Neurosciences, 54, 67-75. http://dx.doi.org/10.1046/j.1440-1819.2000.00639.x
- Lee, S.H. and Oh, K.S. (1999) Offensive type of social phobia: Cross-cultural perspectives. International Medical Journal, 6, 271-279.
- Choy, Y., Schneier, F.R., Heimberg, R.G., Oh, K.S. and Liebowitz, M.R. (2007) Features of the offensive subtype of Taijin-Kyofu-Sho in US and Korean patients with DSM-IV social anxiety disorder. Depression and Anxiety, 25, 230-240. http://dx.doi.org/10.1002/da.20295
- Nagata, T. (2006) An open trial of paroxetine for the “offensive subtype” of Taijin Kyofusho and social anxiety disorder. Depression and Anxiety, 23, 168-174. http://dx.doi.org/10.1002/da.20153
- Suzuki, K., Takie, N., Kawai, M., Minabe, Y. and Mori, N. (2003) Is Taijin Kyofusho a culture-bound syndrome? American Journal of Psychiatry, 160, 1358. http://dx.doi.org/10.1176/appi.ajp.160.7.1358
- Pryse-Phillips, W. (1971) An olfactory reference syndrome. Acta Psychiatrica Scandinavica, 47, 484-509. http://dx.doi.org/10.1111/j.1600-0447.1971.tb03705.x
- Lochner, C. and Stein, D.J. (2003) Olfactory reference syndrome: Diagnostic criteria and differential diagnosis. Journal of Postgraduate Medicine, 49, 328-331.
- American Psychiatric Association (1994) Diagnostic and statistical manual of mental disorders, DSM-IV. American Psychiatric Publishing, Washington DC.
- Chang, S.C. (1997) Social anxiety (phobia) and east Asian culture. Depression and Anxiety, 5, 115-120. http://dx.doi.org/10.1002/(SICI)1520-6394(1997)5:3<115::AID-DA1>3.0.CO;2-D
- Clarvit, S.R., Schneier, F.R. and Liebowitz, M.R. (1996) The offensive subtype of Taijin-Kyofu-Sho in New York City: The phenomenology and treatment of a social anxiety disorder. Journal of Clinical Psychiatry, 57, 523-527. http://dx.doi.org/10.4088/JCP.v57n1104
- McNally, R.J., Cassiday, K.L. and Calamari, J.E. (1990) Taijin-Kyofusho in a black American woman: Behavioral treatment of a “Culturebound” anxiety disorder. Journal of Anxiety Disorder, 4, 83-87. http://dx.doi.org/10.1016/0887-6185(90)90025-5
- Dominguez, R.A. and Puig, A. (1997) Olfactory reference syndrome responds to clomipramine but not fluoxetine: A case report. Journal of Clinical Psychiatry, 58, 497-498. http://dx.doi.org/10.4088/JCP.v58n1106e
- Stein, D.J., Le Roux, L., Bouwer, C. and Van Heerden, B. (1998) Is olfactory reference syndrome an obsessivecompulsive spectrum disorder? Two cases and a discussion. Journal of Neuropsychiatry and Clinical Neurosciences, 10, 96-99.
- Suzuki, K., Takei, N., Iwata, Y., Sekine, Y., Toyoda, T., Nakamura, K., et al. (2004) Do olfactory reference syndrome and Jiko-shu-kyofu (a subtype of Taijin-kyofu) share a common entity? Acta Psychiatrica Scandinavica, 109, 150-155. http://dx.doi.org/10.1046/j.1600-0447.2003.00195.x
- Nakamura, K., Kitanishi, K., Miyake, Y., Hashimoto, K. and Kubota, M. (2002) The neurotic versus delusional subtype of taijin-kyofu-sho: Their DSM diagnoses. Psychiatry and Clinical Neurosciences, 56, 595-601. http://dx.doi.org/10.1046/j.1440-1819.2002.01061.x
- Stein, D.J. (2009) Social anxiety disorder in the West and in the East. Annals of Clinical Psychiatry, 21, 109-117.
- Kleinknecht, R.A., Dinnel, D.L. and Kleinknecht, E.E. (1997) Cultural factors in social anxiety: A comparison of social phobia symptoms and Taijin Kyofusho. Journal of Anxiety Disorders, 11, 157-177. http://dx.doi.org/10.1016/S0887-6185(97)00004-2
- Ono, Y., Yoshimura, K., Yamauchi, K., Asai, M., Young, J., Fujuhara, S. and Kitamura, T. (2001) Taijin Kyofusho in a Japanese community population. Transcultural Psychiatry, 38, 506-514. http://dx.doi.org/10.1177/136346150103800408
- Kasahara, Y. (1988) Social phobia in Japan. Transcultural Psychiatric Research Review, 25, 145-150.
- Lee, S.H. (1987) Social phobia in Korea. Social Phobia in Japan and Korea: Proceedings of the 1st Cultural Psychiatry Symposium between Japan and Korea. The East Asian Academy of Cultural Psychiatry, Seoul.
- Prince, R. and Tcheng-Laroche, F. (1987) Culture-bound syndromes and international disease classifications. Culture, Medicine and Psychiatry, 11, 3-19. http://dx.doi.org/10.1007/BF00055003
- Kim, J., Rapee, R.M. and Gaston, J.E. (2008) Symptoms of offensive type taijin-kyofusho among Australian social phobics. Depression and Anxiety, 25, 601-608. http://dx.doi.org/10.1002/da.20345
- Lim, L. and Divya, A. (2012) A case of Jikoshu-Kyofu treated with cognitive behavioural therapy. Singapore Medical Journal, 53, e139-e141.
- Vriends, N., Pfaltz, M.C., Novianti, P. and Hadiyono, J. (2013) Taijin kyofusho and social anxiety and their clinical relevance in Indonesia and Switzerland. Frontiers in Psychololgy, 4, 3. http://dx.doi.org/10.3389/fpsyg.2013.00003
- Singelis, T.M. and Sharkey, W.F. (1995) Culture, self-construal, and embarrassability. Journal of Cross-Cultural Psychology, 26, 622-626. http://dx.doi.org/10.1177/002202219502600607
- Scherer, K.R., Wallbott, H.G. and Summerfield, A.R. (1986) Experiencing emotion: A cross-cultural study. Cambridge University Press, Cambridge.
- Wallbott, H.G. and Scherer, K.R. (1995) Cultural determinants in experiencing shame and guilt. In: Tangney, J.P. and Fischer, K.W., Eds., Self-Conscious Emotions. The Psychology of Shame, Guilt, Embarrassment, and Pride. Guilford Press, New York, 465-487.
- Markus, H.R. and Kitayama, S. (1991) Culture and the self: Implications for cognition, emotion, and motivation. Psychological Review, 98, 224-253. http://dx.doi.org/10.1037/0033-295X.98.2.224
- Okazaki, S. (1997) Sources of ethnic differences between Asian American and White American college students on measures of depression and social anxiety. Journal of Abnormal Psychology, 106, 52-60. http://dx.doi.org/10.1037/0021-843X.106.1.52
- Dinnel, D.L., Kleinknecht, R.A. and Tanaka-Matsumi, J. (2002) A cross-cultural comparison of social phobia symptoms. Journal of Psychopathology and Behavioral Assessment, 24, 75-84. http://dx.doi.org/10.1023/A:1015316223631
- Zhong, J., Wang, A., Qian, M., Zhang, L., Gao, J., Yang J., Li, B. and Chen, P. (2008) Shame, personality, and social anxiety symptoms in Chinese and American nonclinical samples: A cross-cultural study. Depression and Anxiety, 25, 449-460. http://dx.doi.org/10.1002/da.20358
- Ruscio, A.M., Brown, T.A., Chiu, W.T., Sareen, J., Stein, M.B. and Kessler, R.C. (2008) Social fears and social phobia in the United States: Results from the National Comorbidity Survey Replication. Psychological Medicine, 38, 15-28. http://dx.doi.org/10.1017/S0033291707001699
- Fehm, L., Pelissolo, A., Furmark, T., et al. (2005) Size and burden of social phobia in Europe. European Neuropsychopharmacology, 15, 453-462. http://dx.doi.org/10.1016/j.euroneuro.2005.04.002
- Hwu, H.G., Yeh, E.K. and Chang, L.Y. (1989) Prevalence of psychiatric disorders in Taiwan defined by the Chinese Diagnostic Schedule. Acta Psychiatrica Scandinavica, 79, 136-147. http://dx.doi.org/10.1111/j.1600-0447.1989.tb08581.x
- Cho, M.J., Kim, J.K., Jeon, H.J., Suh, T., et al. (2007) Lifetime and 12-month prevalence of DSM-IV psychiatric disorders among Korean adults. Journal of Nervous and Mental Disease, 195, 203-210. http://dx.doi.org/10.1097/01.nmd.0000243826.40732.45
- Shen, Y.C., Zhang, M.Y., Huang, Y.Q., He, Y.L., Liu, Z.R., Cheng, H., Tsang, A., Lee, S. and Kessler, R.C. (2006) Twelve month prevalence, severity, and unmet need for treatment of mental disorders in metropolitan China. Psychological Medicine, 36, 257-267. http://dx.doi.org/10.1017/S0033291705006367
- Kawakami, N. and Kikkawa, T. (2005) Twelve-month prevalence, severity, and treatment of common mental disorders in communities in Japan: Preliminary findings from the World Mental Health Japan Survey 2002-2003. Psychiatry and Clinical Neurosciences, 59, 441-452. http://dx.doi.org/10.1111/j.1440-1819.2005.01397.x
- Matsunaga, H., Kiriike, N., Matsui, T., et al. (2001) Taijin kyofusho: A form of social anxiety disorder that responds to serotonin reuptake inhibitors? International Journal of Neuropsychopharmacology, 4, 231-237. http://dx.doi.org/10.1017/S1461145701002474
- Kobayashi, N., Kurauchi, S., Sawamura, T., et al. (2003) Case study: The effect of paroxetine on Taijinkyofusho: A report of three cases. Psychiatry, 66, 262-267. http://dx.doi.org/10.1521/psyc.66.3.262.25158
- Nagata, T. (2003) Open trial of milnacipran for Taijin Kyofusho in Japanese patients with social anxiety disorder. International Journal of Psychiatry and Clinical Practice, 7, 107-112. http://dx.doi.org/10.1080/13651500310000690
- Hinton, D.E. and Lewis-Fendandez, R. (2010) Idioms of distress among survivors: Subtypes and clinical utility. Culture, Medicine, and Psychiatry, 34, 209-218. http://dx.doi.org/10.1007/s11013-010-9175-x