Open Journal of Preventive Medicine
Vol.3 No.3(2013), Article ID:33066,9 pages DOI:10.4236/ojpm.2013.33043
Diet-nutrition-related cancer prevention knowledge and beliefs of Sudanese in Khartoum: A descriptive study
![]()
Tuskegee University, Tuskegee, USA; *Corresponding Author: acbenjamin@mytu.tuskegee.edu
Copyright © 2013 Adelia Bovell-Benjamin, Essam Elmubarak. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received 23 February 2013; revised 1 May 2013; accepted 18 May 2013
Keywords: food and nutrition knowledge; cancer prevention; dietary beliefs; food preferences; food practices and purchasing patterns
ABSTRACT
Cancer appears to pose a major threat to the health of the Sudanese population. It is the third leading cause of death in the Sudan after malaria and pneumonia, accounting for 5% of all deaths. In 2005, approximately 22,000 people in the Sudan died from cancer and 17,000 of these people were less than 70 years old. This study was designed to: 1) assess nutrition knowledge and selected dietary beliefs related to cancer in Sudanese residing in Khartoum; 2) identify perceived barriers to the adoption of eating behaviors consistent with those recommended for cancer prevention; and 3) describe the food preferences and dietary practices in Sudanese residing in Khartoum. An interviewer-administered questionnaire elicited demographic information, cancer-related food and nutrition knowledge, food preferences, selected dietary beliefs, barriers to healthy eating and food practices from 182 participants between the ages of 18 and 35 years. More than 50% of females and males correctly identified the food lowest in fiber from a given list. Respondents were knowledgeable about the fat content of their traditional foods, but unaware of the different types of fat. Only 8.8% of the respondents thought that consumption of fruits and vegetables reduced cancer risk. Resondents perceived nutritionists as the most reliable source of information about nutrition and cancer, and the media as the best source of information on nutrition and healthy cooking. “Samin”, feta cheese, a variety of stews, “Zalabia”, lean meat, brown bread, sesame oil, dried okra, fried fish, and chicken were described as preferred food items by respondents. Daily salt/ sodium intake was described by 44% and 39% of the male and female respondents, respectively, as “high” (>2400 mg/day). The findings of this study have clear implications for aggressive nutrition education intervention programs with emphasis on the traditional foods of the Sudan.
1. INTRODUCTION
According to the World Health Organization (WHO), chronic diseases, including cancer are the major causes of death and disability worldwide. Cancer is the third leading cause of death in the Sudan after malaria and pneumonia, accounting for 5% of all deaths [1]. It is worth noting that this apparently low figure is reflective of scantiness in cancer diagnosis and data [2,3]. In 2005, approximately 22,000 people in the Sudan died from cancer, and 17,000 of these people were less than 70 years old. Although it is argued that accurate data regarding the incidence of cancer in the Sudan are scarce, reports from El Hassan et al. [4] and the World Health Organization (WHO) have indicated that breast, mouth and oropharynx cancers are the leading causes of cancer mortality in the Sudan. Ahmed et al. and Elgaili et al. [5,6] determined that breast cancer mortality in the Sudan is high. Cancer of the breast was responsible for 20% and 30% of cancer in Sudanese women between 1999 and 2004, and 2006, respectively [2,5]. Therefore, cancer appears to pose a major threat to the health of the Sudanese population.
Overweight and obesity are important risk factors for cancer. According to the WHO, in 2005, 23% and 37% of men and women, respectively, in the Sudan were overweight. The prevalence of overweight and obesity in males and females in the Sudan is expected to increase further over the next five years. By 2015, 29% and 44% of Sudanese men and women, respectively, will be overeight [7]. Dietary factors are estimated to account for approximately 20% of cancers in developing countries [8]. It is known that circa 40% of cancers could be prevented through healthy diet and sustained regular physical activity.
In the United States (US), individuals described as “African Americans or Blacks” have many subcultures based on linguistics, dietary habits, nutrition knowledge and cancer-related beliefs. African Americans or Blacks in the US cannot be characterized as a homogeneous group because they come from a myriad of socioeconomic, educational and cultural circumstances. In the US, it has been demonstrated that the various subcultures within the African American population have different nutritional knowledge and dietary practices. For example, BovellBenjamin et al. [9] have described the dietary practices of a subculture of African Americans or Blacks in the rural South very differently from Elmubarak et al. [10] who articulated the cancer-related nutrition knowledge and dietary practices of a Sudanese-American subculture in the same environment.
Nutrition knowledge, beliefs, food preferences, food purchasing, consumption and preparation practices are usually shaped by indigenous cultural background, which influence eating behaviors through generations [11]. Although Sudanese-Americans have changed continents and countries, they have brought with them their cultural heritage. Laverentz et al. [12] reported that women of the Nuer culture of the Sudan residing in Iowa faced cultural issues and barriers regarding diet and nutrition. Elmubarak et al. [10] raised concerns about the SudaneseAmericans’ knowledge regarding the role of diet, nutrition and lifestyle choices in cancer prevention.
This study was one phase of a larger study, which aims to better understand the dietary habits and barriers that prevent “African Americans or Blacks” from adopting eating habits consistent with the National Cancer Institute’s (NCI) dietary guidelines. We hypothesized that if the Sudanese-American subculture is to receive effective culturally relevant dietary interventions to reduce cancer risk, it is important to thoroughly understand their dietary habits from the Sudanese and US context. Additionally, Ahmed et al. [5] contended that Sudan is undergoing a cancer epidemic, which warrants aggressive prevention measures. Also, from their study of prognostic characteristics of breast cancer in women in Khartoum, Awadelkarim et al. [3] suggested relevant implications for breast cancer prevention and treatment. Altogether, the above findings, Elmubarak et al.’s [10], and the fact that cultural background influences eating behaviors provide the evidence for urgent diet-cancer-prevention-related research in the Sudan. An additional benefit of this research is that the findings will enable us to better understand the Sudanese-American dietary practices. It was against this backdrop that the study was designed to: 1) assess nutrition knowledge and selected dietary beliefs related to cancer in Sudanese residing in Khartoum; 2) identify perceived barriers to the adoption of the eating behaviors consistent with those recommended for cancer prevention; and 3) describe the food preferences and dietary practices in Sudanese residing in Khartoum.
2. MATERIALS AND METHODS
2.1. Research Setting
The Sudan is located in Northern Africa, bordering the Red Sea, between Egypt and Eritrea. It is the largest country in Africa and the tenth largest in the world. It has a total area of 2,505,810 km2 (967,499 mi2) and is slightly >25% the size of the US. The population is 4,100,887 with 44% under 15 years of age. Khartoum is the capital of the Sudan. It is a tripartite metropolis consisting of Khartoum proper, and linked by bridges to Khartoum North and Omdurman to the west. According to the GeoNames geographical database, the population of Khartoum as estimated in 2010 was 1,947,647. The study was confined to Khartoum. The recruitment and data collection period was prior to South Sudan becoming an independent country in 2011.
2.2. Participants
Participants were recruited through advertisements in local newspapers, flyers, through personal contact, and with some assistance from the local radio stations. Inclusion criteria were:
• Willingness to participate in the study;
• Age 18 years and older;
• Ability to conduct an oral interview;
• Ability to give verbal consent.
2.3. Study Design
A cross-sectional survey was conducted in Khartoum using in-person (face-to-face), in-depth structured interviews to elicit the required information. In-depth interviews have long been recognized as one of the most penetrating methods available for assessing a person’s knowledge and/or attitudes [13]. The sample (N = 182) was self-selected, that is, volunteers who responded were enrolled once they met the criteria.
2.4. Ethical Considerations and Informed Consent
Approval to conduct the study was received from the Human Participants Review Committee at Tuskegee University and the Health Department, Khartoum. Agreement to be interviewed was obtained from all potential participants. The purpose of the study was explained and confidentiality of the information collected assured. Potential participants were informed that participation in the study was voluntary, and they were then required to give verbal consent.
2.5. Questionnaire Development
A preliminary questionnaire was generated through consideration of the study objectives; a review of the relevant literature; the assistance of the Northern Sudanese graduate student involved in the project; and the responses from focus groups conducted with SudaneseAmericans [10]. Questions were ordered and arranged based on recommendations by Smith and Morrow [14]. The questions were refined to address some predisposing factors of the PRECEDE model for health promotion planning. PRECEDE, which is the acronym for Predisposing, Reinforcing, Enabling, Constructs is described elsewhere [15].
The questionnaire contained a mixture of closed and open-ended questions with closed questions predominating. Most questionnaire items were pre-coded, and coding manuals were developed for the open-ended questions. Once the questionnaire (survey instrument) was developed, it was reviewed for clarity, ease of completion, length, format, cultural appropriateness, and its overall presentation. The questionnaire was then translated into Arabic. The survey instrument was pilot-tested on a convenience sample of adults in Khartoum to help identify sensitive, ambiguous and/or poorly understood questions.
2.6. Questionnaire Content
The questionnaire was divided into six distinct sections. The demographics section elicited information regarding education level, gender, age and income. The knowledge section contained questions regarding cancerrelated food and nutrition information. Food preferences (liking or the affective response to the sensory properties of food) is an important determinant of eating behavior, therefore, food preference questions, based on Wardle’s [16] approach were included. Questions to elicit selected dietary beliefs, barriers to eat healthy and food practices were also included.
2.7. Questionnaire Administration
The questionnaires were interviewer-administered to ensure completion of all questions, enhance response rate, facilitate cooperation and clarify misunderstandings [17]. Furthermore, interviews allow the facilitator to repeat; permit standardization and control of the environment and the question order; and observation of nonverbal behavior and recording of spontaneous responses [18]. In an effort to minimize interviewer bias, and increase the survey’s cultural sensitivity, a Sudanese graduate student from Khartoum was trained to administer the survey [19, 20]. At the end of the study, each participant was given a copy of the correct answers to the knowledge questions, and appropriate nutrition education material as necessary.
2.8. Statistical Analyses
Most questionnaire items were pre-coded, and code books were developed for the open-ended questions. Descriptive statistics were used to summarize the data.
3. RESULTS
3.1. Respondents’ Characteristics
A total of 182 adults from Khartoum, Northern Sudan participated in the study. In Table 1, the main characteristics of the respondents show that 59 (32.4%) and 123 (67.6%) were males and females, respectively. Fortyfour percent of the respondents were between the ages of 18 and 24 years (Table 1). More than half (53.6%) of the respondents indicated that they completed university,
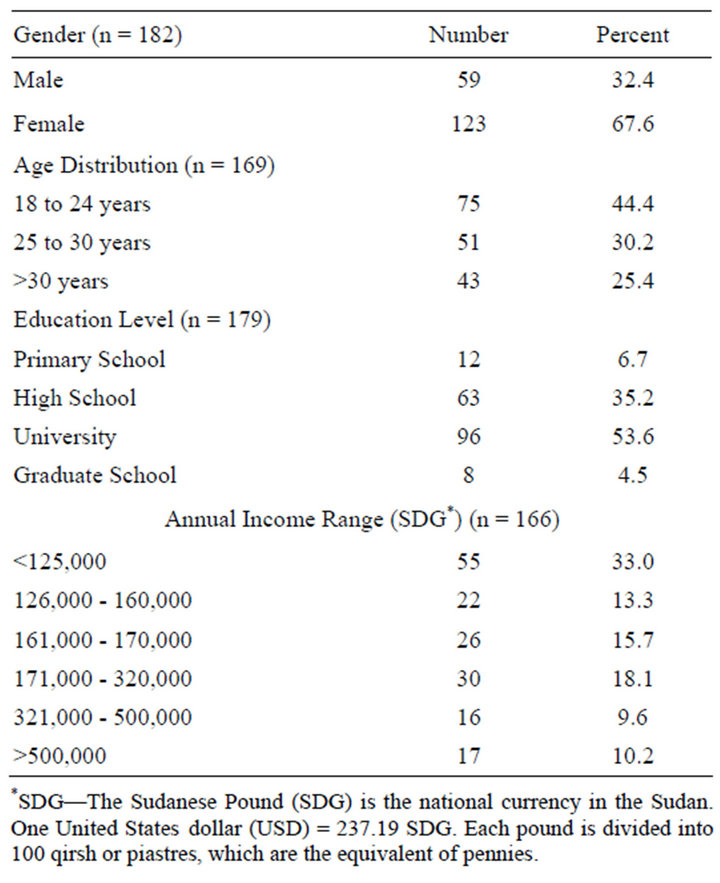
Table 1. Demographic characteristics of the respondents (n = 182).
3.2. Cancer-Related Food and Nutrition Knowledge
More than half (52%) the female respondents answered correctly when asked to select from a list, the food item(s) with the lowest fiber content. Roughly 32% and 20% of the females chose white bread and white rice, respectively. However, 19% of the females incorrectly indicated wheat bread, and 16% did not know which food was lowest in fiber. For the males, 31% incorrectly identified wheat bread as lowest in fiber, while 53% correctly identified the food lowest in fiber.
The respondents were given a list of foods (feta cheese, kissra, samin and rob) to select the one lowest in fat; the majority (86%) correctly selected kissra as the food lowest in fat. The Sudanese food items are described in Table 2. When asked consumption of which foods lowered their chances of getting cancer, 59% and 65% of the males and females, respectively, said foods high in fat. Males (22%) and females (20%) mentioned that consumption of foods high in fiber reduced one’s chances of getting cancer. Only 16 respondents (8.8%) thought that consumption of fruits and vegetables reduced cancer risk.
When asked to relate increased risk of some types of cancer to certain foods, 73% of the male respondents associated it with high intakes of fat; 8% and 3% related it to high intakes of vegetables and fruits, respectively. A slightly higher percentage of female (76.4%) than male respondents (73%) associated higher cancer risk with high intakes of fats. Likewise, more than three quarters of all the respondents agreed with the statement that consumption of high fat foods is associated with cancer. As in the case of the males, six percent of the female respondents associated higher cancer risk to high intakes of vegetables; and 3% of the females indicated that high intakes of fruits were related to higher cancer risk.
Both male (54%) and female (56%) respondents believed that the highest incidence of cancer in the Sudan occurred among women; while 31% and 12% of females and males, respectively, indicated that they did not know. None of the females, and 3% of the males believed that the highest incidence of cancer was among Sudanese children. Roughly 19% of the males and 12% of the females believed that the highest incidence of cancer in the Sudan was among men.
The respondents were asked whether nutrition counseling and specific instructions about how to make dietary changes to prevent cancer would help them modify their eating behaviors. Most male respondents (76.4%) and 84% of the females agreed that this would. When asked whether saturated fats associated with cancers are found in red meats, 34% and 20% of the males indicated true and false, respectively. Twenty nine percent of the males said that they did not know. More than and less than half the female (58%) and male (46%) respondents, respectively, knew that saturated fats associated with cancers are found in samin. Forty-one percent of the male respondents did not answer whether saturated fats associated with cancer are found in cow, sheep or camel milk. Fifty six, 54%, 22% and 10% of the males indicated that they heard cancer is related to how much fat, saturated fat, fiber and fruits/vegetables, respectively, one consumes.
For the females, 52%, 74%, and 27% indicated that they heard some types of cancers are related to how much fat, saturated fat, fiber and fruits/vegetables, respectively, one consumes.
3.3. Selected Dietary Beliefs
In terms of beliefs, the majority of males (88.0%) and females (87.0%) believed that there is a relationship between what people consume and some types of cancer. On the other hand, 51% of the males and 41% of females believed that some types of cancer were related to what people drink. A high percentage of male (59.3%) and female (41.0%) respondents primarily believed that tobacco/marijuana/snuf and eating fatty foods can increase one’s chances of getting cancer. Snuff is a product made from ground or pulverised tobacco leaves; it is the local type of smokeless tobacco. Other things perceived to increase one’s chances for some types of cancer included: poor nutrition habits, pollution/environment, chemicals/ pesticides and atomic rays/microwaves.
Respondents were asked to name specific foods, which they believed increased the risk of some types of cancer. For the males, the main three foods given were fatty foods (47%), lean meat (27%) and starchy foods (24%). The females believed that fatty foods (70%), foods with chemicals/artificial flavors/canned (21%) and fiber (13%) increased one’s cancer risk. The majority of respondents (roughly 98%) believed that nothing would happen if they reduced their present intake of feta cheese, samin, sesame oil or Zalabia (Table 2). However, when asked about reducing fat in the diet, 81% and 76% of the males and females, respectively, believed it would be good for their health. Male and female respondents believed that increased vegetable intake would result in good health. Almost all the respondents (97%) believed that it is important to learn about nutrition and cancer. The nutritionist was perceived to be the most reliable source of information about nutrition and cancer, while the media was perceived as the best source of information on nutrition and healthy cooking (Table 3). Less than half of the males (49%) and females (39%) disagreed with the statement, “there is nothing one can do to prevent cancer”.
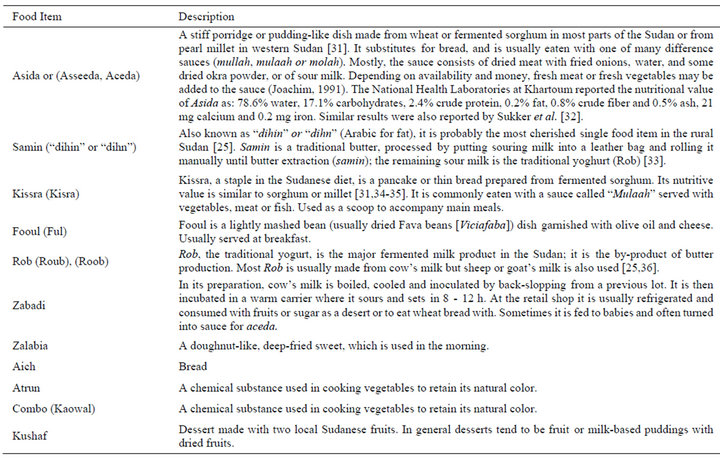
Table 2. Description of Sudanese food items.
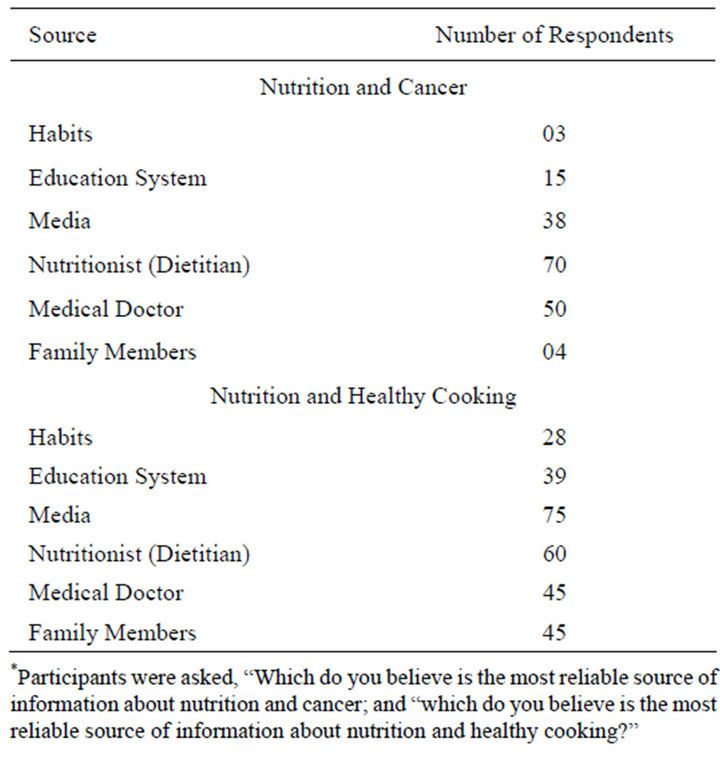
Table 3. Sources of information about nutrition, cancer and healthy cooking* (n = 182).
3.4. Barriers
Cost was the most frequently mentioned barrier to including fruits and vegetables in their daily diets (Table 4). Other frequently reported barriers included health issues, taste preferences, and family habits, which affected respondents’ decision as to which foods to eat. Respondents were asked about the problems related to purchasing, preparing and consuming healthy foods. Again, the respondents cited income, availability, lack of time, quality of foods, lack of support from family members and convenience as the problems. More than 50% and 46% of the males and females, respectively, indicated that it was not difficult to get reliable information about nutrition and cancer from a nutritionist or dietitian. However, when asked if they ever tried to get information from a nutritionist or dietitian, fewer males (54%) than females (66%) said yes.
3.5. Food Preferences
Male respondents (39%) expressed a preference for stews while females (38%) preferred grilled foods. Male respondents (37%) also expressed preference for grilled foods. Of the male respondents, 48% and 39% revealed that they consumed “fooul” once and twice per day, respectively (Table 2). Females (49%) indicated that they ate “fooul” twice per day. The responses revealed that 46% of the males and 41% of females consumed “Rob” weekly, while 36% and 26% males and females, respectively, consumed it daily. Monthly consumption of
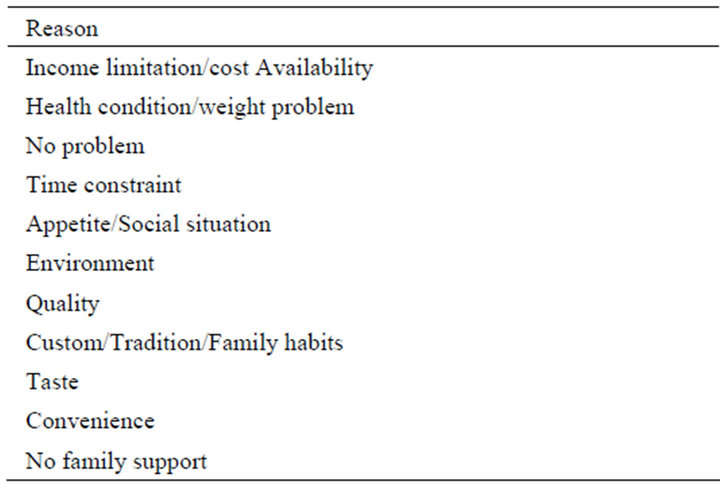
Table 4. Perceived barriers for not eating the way they would like to.
“samin” was 41% for males and 44% for females. Feta cheese, a variety of stews, “Zalabia”, lean meat, brown bread, sesame oil, dried okra, fried fish, and chicken were also commonly favored food items.
3.6. Food Practices and Purchasing Patterns
Many respondents (64%) said they preferred their vegetables cooked without fat most of the time. When asked, “when you eat chicken, do you eat the skin?” Forty six, 26.9%, 13.2%, and 13.2% of the respondents replied, never, rarely, always and most times, respectively. More than half the respondents indicated that they always got rid of fat off meat before cooking. Roughly 76% of the respondents said they consumed dark, green vegetables daily, while 28% said weekly. Fewer respondents (57%) stated that they consumed vegetables that are yellow and orange daily and 38% said weekly. According to the respondents (79%), red vegetables were consumed daily. A low 39% of the respondents indicated daily fruit consumption and 20% said once per week. Females (41%), and 39% of males stated that they consumed fried food most frequently.
When asked where they got drinking water from, most respondents (80%) stated that it was pipe-borne, and 76% said they never boiled it before drinking. “Atrun” was never used when cooking vegetables by 37% of respondents, while an equal percentage of respondents (25%) said they rarely or sometimes used it. Similarly, 72% of the respondents indicated that “combo” was never used when cooking vegetables. Slightly more females (37%) than males (31%) said that white bread would be typically found on their plates when eating a meal at home. Typical desserts reported by the respondents were fruit-based (“Kushaf”) and custard pudding, 62% and 14%, respectively. Table 5 shows a typical breakfast as reported by the respondents.
Respondents were asked about their fast food practices;
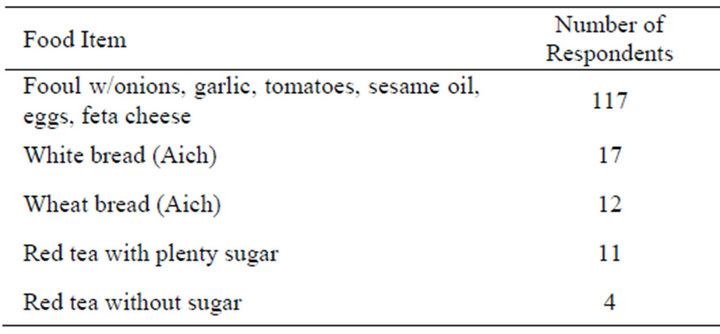
Table 5. Typical Sudanese breakfast items as described by the respondents.
more than half the males (51%) and fewer females (49%) said they consumed fast food once per day. Sixty female respondents (49%) reported spending 500 to 400,000 Sudanese Pounds (SDG) daily on fast food, while 30 males (51%) said they spent between 200 to 10,000 SDG. One SDG is equivalent to US $0.23. When asked to describe their daily sugar intake, 46% of the respondents said “neither high nor low”; 14.3% said “very high”; 21% said “high”; 15.4% said “low”; and 3.3% said “very low”.
Daily salt intake was described by male (44%) and female (39%) respondents as “high”. Male and female respondents consumed <3 cups tea and coffee daily.
4. DISCUSSION
This study elicited descriptive information about nutrition/diet-cancer-related knowledge, dietary beliefs; perceived barriers to the adoption of eating behaviors consistent with those recommended for cancer prevention; and described food preferences and dietary practices in Sudanese residing in Khartoum. When Hamad [1] discussed the cancer initiatives taken in the Sudan to prevent, detect and treat cancer, none of these included diet, nutrition or physical activity, which have important roles in cancer prevention and treatment. Therefore, our study also identified potential gaps, which need to be filled for future diet-cancer related studies in the Sudan and US.
Dietary fiber was always a significant part of the human diet, but its intake has decreased over the past two centuries, partly due to consumption of increasing quantities of processed foods [21]. According to Musaiger [22], the traditional diet of the Sudan was characterized by high-fiber content and low fat, cholesterol and sodium, but has been replaced with one high in fat, cholesterol, sodium, sugar and low in fiber. Currently, the importance of the preventive and management effects of dietary fiber in cancer, and other chronic disease prevention is receiving renewed interest [23]. According to WCRF/AICR [24], foods containing dietary fiber in all probability protect against colorectal cancer.
In the current study, from the food list given, more respondents than expected were incapable of identifying foods low in dietary fiber. These respondents’ choices clearly indicated limited knowledge about dietary fiber; they could not differentiate between high-fiber and highly processed or refined foods such as white rice. Too many respondents were unaware that high intakes of fiber-rich foods reduced one’s chances for some types of cancer. The public health goals of WCRF/AICR [24] indicate that relatively unprocessed cereals (grains) and/or pulses (legumes), and other foods that are a natural source of dietary fiber, should contribute to a population average intake of at least 25 g non-starch polysaccharide daily. Further, very few respondents knew that regular daily consumption of fruits and vegetables reduced cancer risk. Fruits, vegetables, unprocessed grains and cereals are usually rich sources of dietary fiber. The WCRF/AICR [24] has recommended eating at least five portions/servings (at least 400 g) of a variety of non-starchy vegetables and of fruits daily. A high percentage of males were unaware of the relationships among saturated fats, red meats, different types of milk (cow, sheep, camel) “samin” and cancer, although milk is integral to the life of the Sudanese [25].
Harnack et al. [26] examined the relationship of cancer prevention-related nutrition knowledge, beliefs, and attitudes to cancer prevention dietary behavior; and concluded that those who believe that it is difficult to eat a more healthful diet are less likely to do so. The current study queried the prevalence of the belief that there is a relationship between what one consumes and cancer, an issue of tremendous importance for cancer education. Optimistically, most respondents believed that there is a relationship between what people consume and cancer; and it is important to learn about nutrition and cancer. This is gratifying, given concern that nutrition is not considered in cancer prevention, detection and treatment initiatives. However, it should be noted that although respondents agreed to this, their responses to other questions suggested a range of beliefs about nutrition and cancer causation also exist.
Our findings indicated that the most frequently reported reliable source of information on nutrition and healthy cooking was the media. According to Charlton et al. [27], such findings have both positive and negative connotations. In terms of negativity, there is the possibility that the information could be unscientific and presented in a misleading manner. On the positive side, this provides a wide reaching opportunity for qualified nutritionists and dietitians to use the media to disseminate messages on nutrition and healthy cooking. In this study, a high percentage of the respondents indicated frequent consumption of fried foods. Stott-Miller et al. [28] concluded that regular consumption of select deep-fried foods such as French fries, fried chicken, and doughnuts is associated with an increased risk of prostate cancer.
Unaffordable food prices usually impact negatively on healthy choices. On average, Sudanese spend 61% of their income on food [29]. Cost was the most frequently mentioned barrier to healthy eating in this study. It has been reported that in the Sudan, vegetables cost too much, for example, one kilogram of tomatoes cost 20 SDG [30]. Traditional foods such as “Ful”, partly imported from Egypt; and sorghum, one of the staple foods of the Sudan have experienced increased prices. Sudanese are forced to choose less healthy alternatives, for example, eating two meals per day instead of three; and using less vegetables and meat because they are so expensive. Interventions to educate the Sudanese about healthy food choices on limited food budgets are needed. Programs regarding policy changes to address rising food prices and the other barriers mentioned are also needed.
Sudanese in Khartoum were asked to describe their daily sugar intake including honey and zalabia. Recommended daily intakes of sugar for women and men are five teaspoons or 20 - 25 g and nine teaspoons or 36 - 38 g, respectively; that is, if there is no health condition, which requires lower intakes. In the US, the recommended daily sodium intake for adults without health restriction is 2400 mg. Responses were recorded on a five-point intake level, which ranged from “very high” through “neither high nor low” to “very low” (Table 6). When compared with recommended daily sodium intake, a large number of the respondents reported exceeding the requirements daily. It can be speculated, however, that intakes for people in the Sudan may be higher than the recommendation for people in the US because of the hot and humid climate in the country. It has been reported by Abdelgadir et al. [25] that in the Sudan “samin”, other milk products, animal fat, honey and sugar are highly cherished and integral to life. This is apparent in the reported consumption practices, sugar and sodium intakes, even though it is highly likely that there was under-
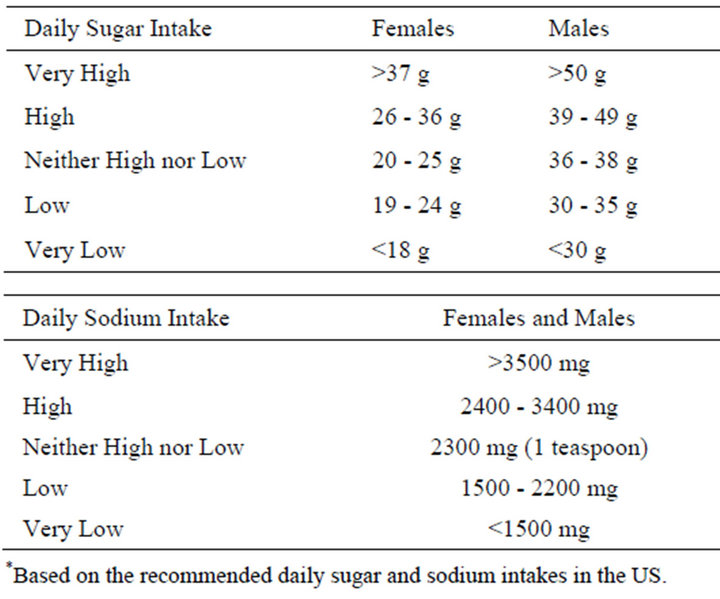
Table 6. Intake levels used to describe daily sugar and sodium intake in Sudanese in Khartoum, Sudan.*
reporting.
Elmubarak et al. [10] conducted focus groups with Sudanese-Americans to generate background information for a pre-conceptualized diet, nutrition and cancer-related survey instrument to be administered to Sudanese-Americans. This instrument (with some modifications) was tested on Sudanese in Khartoum. Although our sample in Khartoum was predominantly younger Sudanese, their responses indicated preference for their indigenous foods, such as “fooul”, “rob”, “samin”, and “Zalabia”. Similar preferences were expressed by the Sudanese-Americans. The typical breakfast (Table 5) described by the Sudanese in Khartoum was similar to that described by Sudanese-Americans residing for several years in Alabama, United States [10]. Similarly, cost was also perceived as the most common barrier to healthy eating by the Sudanese-Americans and Sudanese in Khartoum [10].
Study Limitations and Strengths
A limitation of this type of study is that the findings cannot be generalized across the broader Sudanese population because the sample size was small, restricted to the Khartoum area; was cross-sectional, and most respondents had high levels of education. However, our focus was on versatility of the findings, rather than generalizations. Like any self-reported description of nutrition knowledge, dietary patterns and preferences, responses in this study could have been influenced by social desirability; there is always the possibility that participants reported their diets, preferences and dietary preparation methods as healthier than they were in reality. However, the findings in this study could be generalized to other chronic diseases such as diabetes. Overall, this study adds to the existing literature in that relatively few qualitative studies have focused on nutrition knowledge and dietary practices of Sudanese in relation to cancer prevention. The findings provide information that could be useful in the designs of interventions for Sudanese-Americans regarding the role of diet and nutrition choices in cancer prevention.
5. CONCLUSION
The evidence is clear that the Sudan is undergoing a cancer epidemic, which calls for compelling prevention policies and programs. The findings of this study have clear implications for aggressive nutrition education intervention programs with emphasis on the traditional foods of the Sudan. Furthermore, interventions should aim at the following: 1) educating the Sudanese population about healthy food preparation methods, healthy food choices on limited food budgets, acceptable levels of sodium, fat and sugar consumption, general increase in the consumption of high fiber foods, fruits and vegetables; 2) addressing rising food prices and other barriers, which prevent healthy eating; and 3) qualified nutritionists and dietitians in the Sudan should utilize the media to disseminate messages on diet, nutrition, healthy cooking and cancer prevention.
REFERENCES
- Hamad, H.M. (2006) Cancer initiatives in Sudan. Annals of Oncology, 17, 32-36. doi:10.1093/annonc/mdl985
- Awadelkarim, K.D, Aceto G., Veschi, S., Elhaj, A., Morgano, A., Mohamedani, A.A., Eltayeb, E.A., Abuidris, D., Di Gioacchino, M., Battista, P., Verginelli, F., Cama, A., Elwali, N.E. and Mariani-Costantini, R. (2007) BRAC1 and BRAC2 status in a Central Sudanese series of breast cancer patients: Interactions with genetic, ethnic and reproductive factors. Breast Cancer Research Treatment, 102, 189-199. doi:10.1007/s10549-006-9303-z
- Awadelkarim, K.D., Arizzi, C., Elamin, E., DeBlasio, P., Hamad, H.M.A., Mekki, S.O., Osman, I., Biunno, I., Elwali, N.E., Mariani-Costantini, R. and Barberis, M.C. (2008) Pathological, clinical and prognostic characteristics of breast cancer in Central Sudan versus Northern Italy; implications for breast cancer in Africa. Histopathology, 52, 445-456. doi:10.1111/j.1365-2559.2008.02966.x
- El Hassan, A., El Hassan, L., Mudawi, H., Gasim, B., Own, A., Elamin, E., Ouf, M.I., El Mekki, M. and Fedail, S. (2008) Malignant gastric tumors in Sudan: A report from a single pathology center. Hematology Oncology and Stem Cell Therapy, 1, 130-132.
- Ahmed, H.G., Ali, A.S. and Almobarak, A.O. (2010) Frequency of breast cancer among Sudanese patients with breast palpable lumps. Indian Journal of Cancer, 47, 23- 26. doi:10.4103/0019-509X.58854
- Elgaili, E.M., Abuidris, D.O., Rahman, M., Michalek, A.M. and Mohammed, S.I. (2010) Breast cancer burden in central Sudan. International Journal Women’s Health, 2, 77-82.
- WHO Global Infobase: Data for Saving Lives. https://apps.who.int/infobase
- Willet, M.C. (1995) Diet, nutrition and avoidable cancer. Environmental Health Perspectives, 103, S165-S170.
- Bovell-Benjamin, A, Dawkins, N., Pace, R. and Shikany, J.M. (2010) Dietary consumption practices and cancer risk in African Americans in the rural South. Journal of Health Care for the Poor and Underserved, 21, 57-75. doi:10.1353/hpu.0.0361
- Elmubarak, E., Bromfield, E. and Bovell-Benjamin, A.C. (2005) Focused interviews with Sudanese Americans: Perceptions about diet, nutrition, and cancer. Preventive Medicine, 40, 502-509. doi:10.1016/j.ypmed.2004.09.021
- Bronner, Y.L., Ebede, T.L., Hossain, M.B., Nowverl, A. and Harris, E. (2001) Historical assessment of nutrition studies using only African American study subjects: Gender, socioeconomic status, and geographic location. Ethnicity & Disease, 11, 134-143.
- Laverentz, M.L., Cox, C.C. and Jordan, M. (1999) The Nuer nutrition education program; breaking down cultural barriers. Health Care for Women International, 20, 593- 601.
- Novak, J.D. and Gowin, D.B. (1984) Learning how to learn. Cambridge University Press, Cambridge. doi:10.1017/CBO9781139173469
- Smith, P.G. and Morrow, R.H., Eds. (1993) Methods for field trials of interventions against tropical diseases: A tool box. Oxford University Press, Inc., New York, 176- 196.
- Green, L. and Kreuter, M. (1991) Health promotion planning. Mayfield Publishing Co., Mountain View, 2-20.
- Wardle, J. (1993) Food choices and health evaluation. Psychology and Health, 8, 65-75. doi:10.1080/08870449308403167
- Margetts, B.M. (1991) Basic issues in designing and interpreting epidemiological research. In: Margetts, M. and Nelson, M., Eds., Design Concepts in Nutritional Epidemiology. Oxford University Press, New York, 22-51.
- Perkin, J. (1992) Design and use of questionnaires in research. In: Monsen, E.R., Ed., Research: Successful Approaches. American Dietetic Association, Chicago.
- Fowler, F.J. and Mangione, T.W. (1990) Standardized survey interviewing. Sage Publications Inc., Applied Social Research Method Series, Newbury Park.
- Schinke, S.P., Singer, B., Cole, K. and Contento, I.R. (1996) Reducing cancer risk among Native American adolescents. Preventive Medicine, 25, 146-155. doi:10.1006/pmed.1996.0040
- Burkitt, D.P. and Trowell, H.C. (1975) Refined carbohydrate and disease. Academic Press, New York.
- Musaiger, A.O. (2002) Diet and prevention of coronary heart disease in the Arab Middle East countries. Medical Principles and Practice, 11, 9-16. doi:10.1159/000066415
- Kendall, C.W.C., Esfahani, A. and Jenkins, D.J.A. (2010) The link between dietary fibre and human health. Food Hydrocolloids, 24, 42-48. doi:10.1016/j.foodhyd.2009.08.002
- WCRF/AICR (World Cancer Research Fund/American Institute for Cancer Research) (2007) Food, nutrition, physical activity, and the prevention of cancer: A global perspective. AICR, Washington DC.
- Abdelgadir, W.S., Ahmed, T.K. and Dirar, H.A. (1998) The traditional fermented milk products of the Sudan. International Journal of Food Microbiology, 44, 1-13.
- Harnack, L., Block, G., Subar, A., Lane, S. and Brand, R. (1997) Association of cancer prevention-related nutrition knowledge, beliefs, and attitudes to cancer prevention dietary behavior. Journal of the Academy of Nutrition and Dietetics, 97, 957-965.
- Charlton, K.E., Brewitt, P. and Bourne, L.T. (2004) Sources and credibility of nutrition information among black urban South African women, with a focus on messages related to obesity. Public Health Nutrition, 761, 801-811.
- Stott-Miller, M., Neuhouser, M.L. and Stanford, J.L. (2013) Consumption of deep-fried foods and risk of prostate cancer. The Prostate, 73, 960-969. doi:10.1002/pros.22643
- FAO-SIFSIA (2010) Soaring food prices and its policy implications in north Sudan: A policy brief Sudan institutional capacity programme: Food security information for action (sifsia) brief soaring food prices. http://www.fao.org/fileadmin/user_upload/sifsia/docs/Policy
- Laessing, U. (2013) Sudanese boycott meat to fight food inflation. AL ARABIYA. www.alarabiya.net
- Ibnouf, F.O. (2012) The value of women’s indigenous knowledge in food processing and preservation for achieving household food security in rural Sudan. Journal of Food Research, 1, 238-253. doi:10.5539/jfr.v1n1p238
- Sukkar, M.Y., Boutros, J.Z. and Yousif, M.K. (1975) The composition of common Sudanese foods. Sudan Medical Journal, 13, 51.
- Ibnouf, F.O. (2009) The role of women in providing and improving household food security in Sudan: Implications for reducing hunger and malnutrition. Journal of International Women’s Studies, 10, 144-167.
- Sulieman, A.E., Ali, A.O. and Elkhalifa, E.A. (2003) Some characteristics of the Sudanese bread (Kissra) supplemented with fenugreek (Trigonellafoenum-graecum L.). Gezira Journal of Agricultural Science, 1, 15-25.
- Abdualrahman, M.A.Y. and Ali, A.O. (2012) Supplementation of Sudanese sorghum bread (Kissra) with Bambara groundnut flour (Vignasubterranea (L.) Verdc.). International Journal of Agricultural Research, 7, 215-222.
- Dirar, H.A. (1993) The indigenous fermented foods of the Sudan. C.A.B. International, Wallingford.