Vol.3, No.10, 623-625 (2011)
doi:10.4236/health.2011.310105
C
opyright © 2011 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/
Health
Comparison of postoperative sore throat following
laryngoscopy conducted by Miller and Macintosh
laryngoscope blades
Khosro Barkhordari, F arhad Ete zadi, R eza Shariat Mo harari , Mohammad Re za Khaj avi*
Tehran University of Medical Sciences, Sina Hospital, Tehran, Iran; *Corresponding author: khajavim@tums.ac.ir
Received 6 January 2011; revised 1 June 2011; accepted 15 June 2011.
ABSTRACT
BACKGROUN D: Post operative sore throat (PST)
is one of the most common complaints after
tracheal intubation. In this study we compared
the effects of curved and straight laryngoscope
blades on severity and incidence of PST. METH-
OD: In this prospective randomized clinical trial
we evaluated incidence and severity of PST in
147 ASA physical status I–II, aged 18 – 62 y
(group Miller, n = 71), (group Macintosh, n = 76)
following intubation with Miller and Macintosh
laryngoscope blades by using Visual Analog
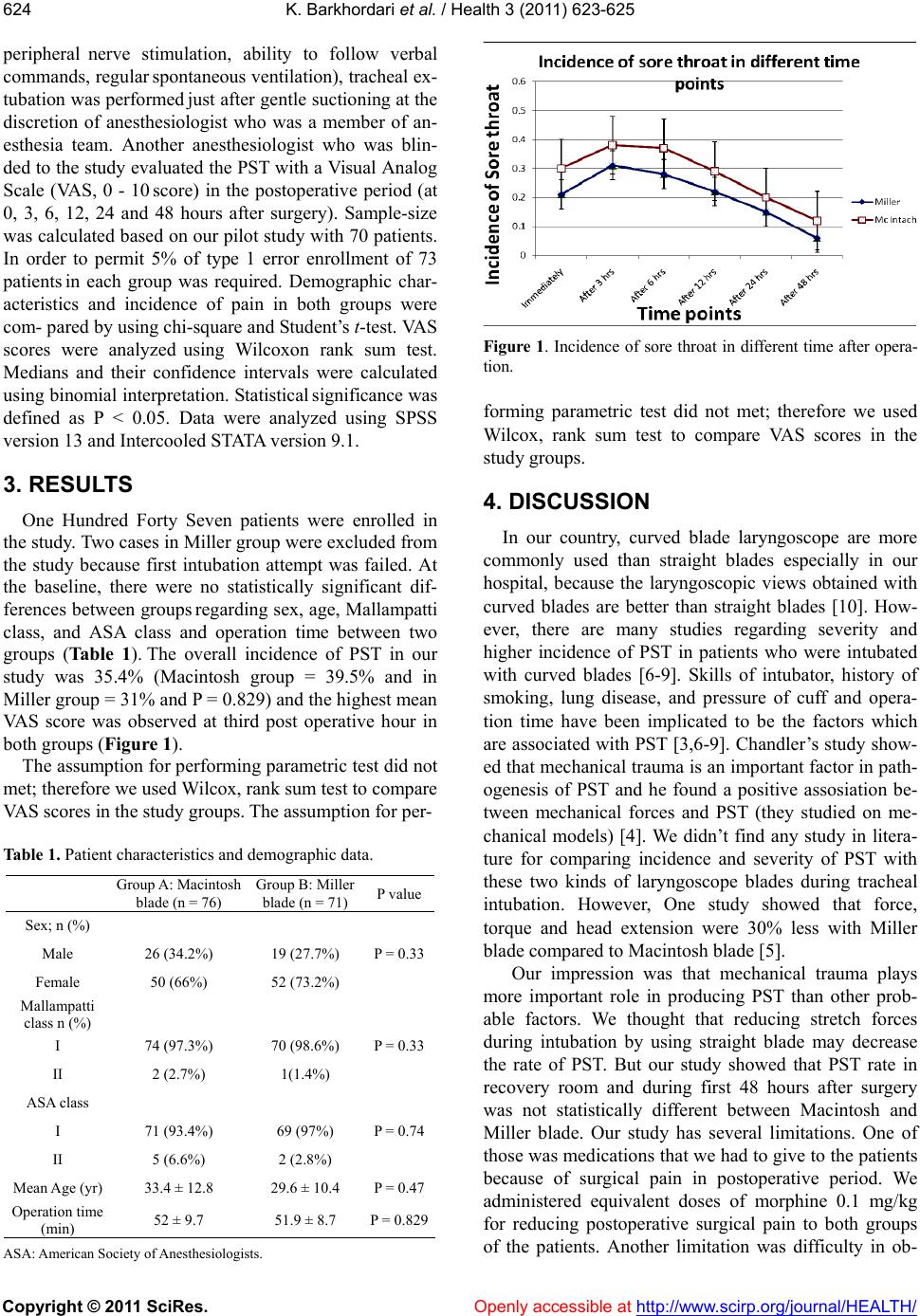
Scale (VAS). RESULTS: The overall incidence of
PST in our study was 35.4% (Macintosh group =
39.5% and in Miller group = 31% and P = 0.829).
The incidence of PST was not statistically differ-
ent between two kinds of laryngoscope blades
and the mean rank of pain score was not statisti-
cally different in recovery room and up to 48
hours after surgery. CONCLUSIONS: Our study
showed these types of laryngoscope blade had
not association with incidence and severity of
PST.
Keywords: Post Operative Sore Throat;
Tracheal Incubation; Laryngoscope Blades
1. INTRODUCTION
Post operative sore throat (PST) is one of the most
frequent complaints after tracheal intubation and its in-
cidence varies between 14% - 50% [1-4]. Mucosal injury,
stretch of ligaments and muscles of throat, prolonged
surgery, changing position of patients during surgery
have been implicated in the pathogenesis of PST [4].
Chandler’s study showed that pressure trauma is very
important to induce PST and he found an association
between mechanical forces and PST [4].
Our hypothesis was that straight blade (Miller) gener-
ates less pressure on pharyngeal wall, muscles and liga-
ments of pharynx than curved blade (Macintosh). Hast-
ings et al showed that the use of Miller laryngoscope
blade required less force and head extension than Mac-
intosh one [5]. We didn’t find any study comparing se-
verity of pain produced by these two common blades
used for laryngoscopy.
The aim of our study was to compare the incidence
and severity of PST with Macintosh and Miller laryngo-
scope blades during normal intubating attempts.
2. METHODS
After Institutional Ethics Committee app roval, written
informed consent was obtained for all patients. We pro-
spectively studied 147 consecutive adult patients (18 -
64 years old) with ASA physical status I–II receiving
general anesthesia with tracheal intu bation. Using a com-
puter generated sequence of numbers, patients were
randomly allocated to be in tubated using either a straight
blade laryngoscope (n = 71) or a curved blade, (n = 76).
Failure to tracheal intubation in the first attempt, posi-
tive history of sore throat, use of NSAIDS, head and
neck surgery, smoking, Mallampati class greater than 2
were our exclusions criteria. After establishing IV access
and use of standard monitoring, midazolam 0.05 mg/kg,
fentanyl 2 µg/kg injected as premedication, thiopental
Na 5 mg/kg, and atracurium 0.4 mg/kg were used for
induction of anesthesia. An anesthesiologist with three
years of continuous practice performed all endotracheal
intubation gently. Size of tracheal tubes were adjusted
for age and body size of patients, and miller no 2 and
Macintosh no 3 blades were used. Endotracheal tubes
(ETT) were lubricated with sterile water. ETT cuffs were
inflated at the safe occlusive volume so initial Cuff
pressure was fixed at 20 cm H2O (Mallinckrodt, Seel-
scherf 1, Germany). Anesthesia was maintained by: air/
N2O (50%/50%), isoflurane (1% to 1.2%) a nd inter mittent
injection of fentanyl as was necessary.
When tracheal extubation criteria were met (return of
neuromuscular function confirmed using train-of-four