E. N. TEITELBAUM ET AL.
Copyright © 2011 SciRes. SS
429
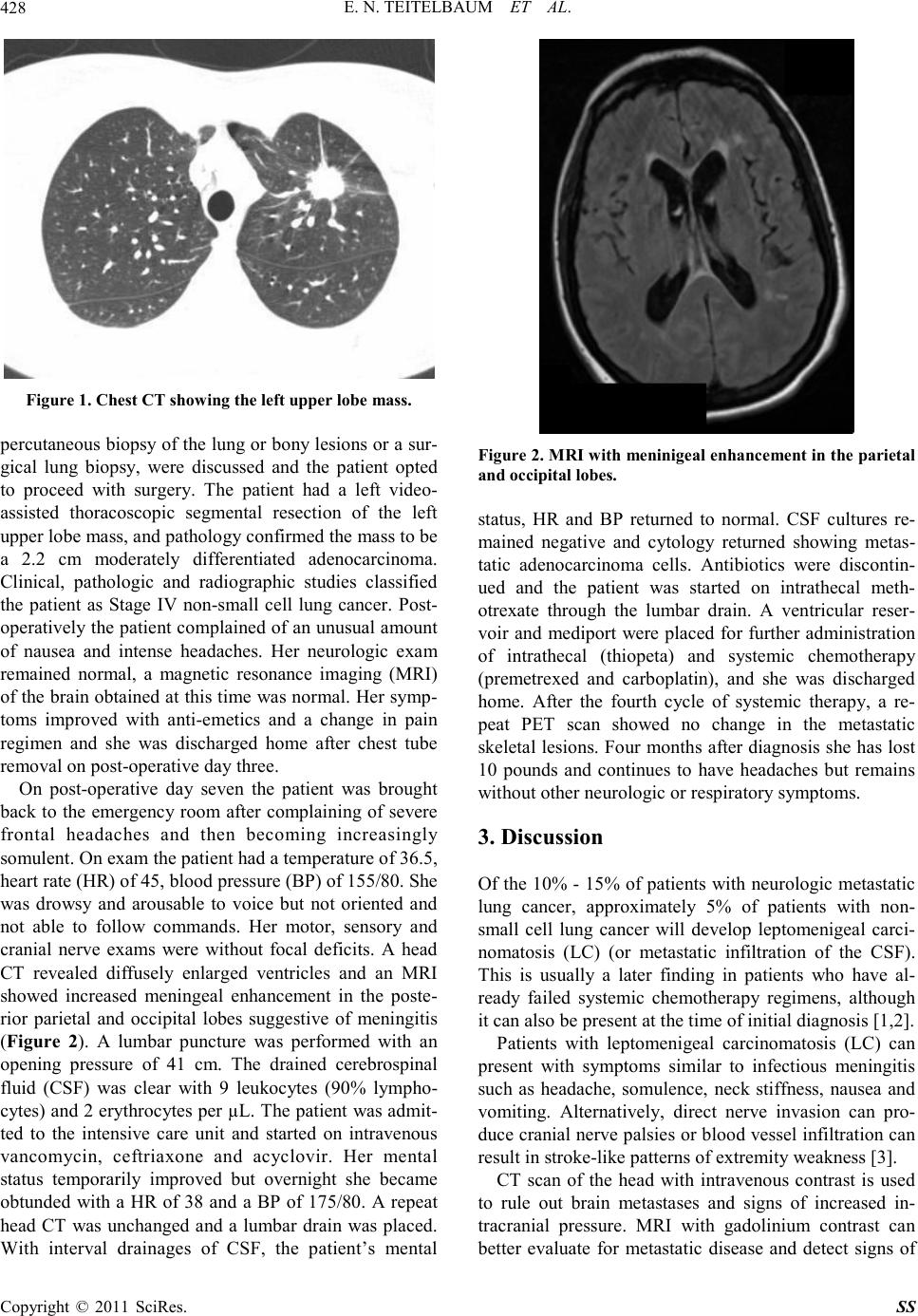
LC such as meningeal enhancement [3,4]. While imaging
can serve as a useful guide, CSF histology remains the
gold standard for diagnosis of LC. CSF cytology is posi-
tive for malignant cells in 50% - 70% of cases, although
this yield can be increased to 90% with second and third
lumbar punctures. Increased opening pressures, high
protein and low glucose levels are also common findings
on CSF examination [5].
LC remains a bleak diagnosis with median survivals of
one to five months in treated patients and four to six
weeks if left untreated [2,6,7]. Wasserstrom reviewed 90
patients with LC from various primary tumors treated
with intrathecal methotrexate. The 23 patients with all
type lung cancer primaries had a 50% response rate and a
median survival of 4 months [6]. Chamberlain studied a
selective population of patients with LC from non-small
cell lung cancer primaries. These 32 patients were treated
with intrathecal methotrexate and some received in-
trathecal cytarabine and thiotepa as second and third-line
therapies respectively. Twelve of the patients received
concurrent systemic chemotherapy. Complete cytologica l
and partial clinical responses were seen in 43% of pa-
tients treated with methotrexate, 50% of those treated
with cytarabine and 33% of those treated with thiotepa.
Median survival was five months and no difference was
seen in the patients who also received systemic chemo-
therapy [2]. Other therapies used in LC have included
gemcitabine and ara-C, as well as radiotherapy and sur-
gery to palliate compressive brain or spinal cord metas-
tases [8].
4. Conclusions
LC is a rare complication of non-small cell lung cancer
that imparts a dismal prognosis. Diagnosis is made by
imaging and CSF evaluation with cytology. Treatment
with intrathecal chemotherapy results in a small im-
provement in life expectancy. As such, palliation of
symptoms and discussions with patients and their family
members regarding realistic expectations for prognosis
are important aspects of care.
5. References
[1] T. W. Shields, J. Locicero, C. E. Reed and R. H. Feins,
“General Thoracic Surgery,” 7th Edition, Williams &
Wilkins, Malvern, 2009.
[2] M. C. Chamberlain and P. Kormanik, “Carcinoma Men-
ingitis Secondary to Non-small Cell Lung Cancer: Com-
bined Modality Therapy,” Archives of Neurology, Vol. 55,
No. 4, 1998, pp. 506-512. doi:10.1001/archneur.55.4.506
[3] N. Pavlidis, “The Diagnostic and Therapeutic Manage-
ment of Leptomeningeal Carcinomatosis,” Annals of On-
cology, Vol. 15, Supplement 4, 2004, pp. iv285-iv291.
doi:10.1093/annonc/mdh941
[4] M. B. Fukui, C. C. Meltzer, E. Kanal and J. G. Smirnio-
topoulos, “MR Imaging of the Meninges,” Radiology,
Vol. 201, No. 3, 1996, pp. 60 5-612.
[5] E. T. Wong and J. T. Joseph, “Meningeal Carcinomatosis
in Lung Cancer,” Journal of Clinical Oncology, Vol. 18,
No. 15, 2000, pp. 2926-2927.
[6] W. Wasserstrom, J. Glass and J. Posner, “Diagnosis and
Treatment of Leptomeningeal Metastases from Solid
Tumors: Experience with 90 Patients,” Cancer, Vol. 49,
No. 4, 1982, pp. 759-772.
doi:10.1002/1097-0142(19820215)49:4<759::AID-CNC
R2820490427>3.0.CO;2-7
[7] M. Balm and J. Hammack, “Leptomeningeal Carcinoma-
tosis,” Archives of Neurology, Vol. 53, No. 7, 1996, pp.
626-632.
[8] M. Westphal, O. Heese and M. de Wit, “In tracranial Me-
tastases: Therapeutic Options,” Annals of Oncology, Vol.
14, Supple ment 3, 2003, pp. iii4- 10.
doi:10.1093/annonc/mdg741