A. Grinshpoon et al. / Open Journal of Psychiatry 1 (2011) 126-131
128
his/her own ideas.
Some nurses, however, cited negative advocacy ex-
periences, for instance, when overzealous advocates
urged a client’s point of view without actually attempt-
ing to mediate as expected by them. By mediation they
meant acting as a go-between two parties i.e. the staff
member and the patient, in a dispute, in which case ad-
vocates should be expected to represent both the profes-
sional and the patient viewpoint. Some nurses also re-
ported that they would be failing their professional duty
if they represented a patient’s view themselves.
2.3. Legal Representation
According to Oladimeji [8] the LR of psychiatric pa-
tients should not only protect patient rights but also
promote patient autonomy and welfare by spelling out
wishes, needs, and interests of the patients being repre-
sented. In this regard, legal advocates should also col-
laborate with professional carers in making decisions
about a patient treatment and then explain the deci-
sion-making process and the decisions made to the pa-
tient. Lawyers representing a patient at a DPB hearing
typically ground their arguments for or against a pa-
tient’s detention in hospital, at least partly, on the reports
on the his current mental state and behavior of nurses,
physicians, and significant others. Healthcare profes-
sionals, including nurses, thus need to be well instructed
and have thorough knowledge on patients civil and hu-
man rights especially of those who must appear at DPB
hearings. But are all nurses sufficiently informed or have
an appropriate professional attitude toward LR of the
human and civil rights of involuntary patients in psychi-
atric hospital setting? Would LR of patients in the hos-
pital setting result in some nurses feeling threatened or
relieved, or fearing for their patients perceived harm or
being optimistic about the well-being of their patients?
These issues are controversial and need to be further
assessed.
3. METHODS
3.1. Study Design
A case-control pilot survey was designed to determine
baseline beliefs and attitudes of hospital mental health
professionals towards the LR of involuntarily hospital-
ized psychiatric patients appearing before a DPB. A lon-
gitudinal study design was used to determine possible
changes in the participants’ attitudes over one year time,
following routine implementation of the practice of LR
of patients appearing before a DPB at the Tirat Carmel
Mental Health Center in Israel. The Institutional Review
Board approved the research protocol and written in-
formed consent was received from all participants. The
study was initially planned as a pilot study, and after
evaluation of the preliminary data a longitudinal study,
involving multiple mental health centers across the
country was planned.
3.2. Participants and Setting
The setting for this study was a state psychiatric hospital
which has a total of 228 beds distributed as follows: 24
adolescents’ beds, 68 chronic and 136 acute patients’
beds, and 14 ambulatory centers. The hospital serves a
catchment area with a mixed lower and middle-income
population of 600,000. During the survey period, the
professional staff of the hospital included 83 psychiatric
registered nurses, 21 certified psychiatrists, 11 psychiat-
ric residents, and 14 social workers. LR was imple-
mented in the hospital since November 1, 2007. Over the
1-year course of the study, 51 DPB sessions have been
conducted, and 50 involuntarily hospitalized patients
received routine LR.
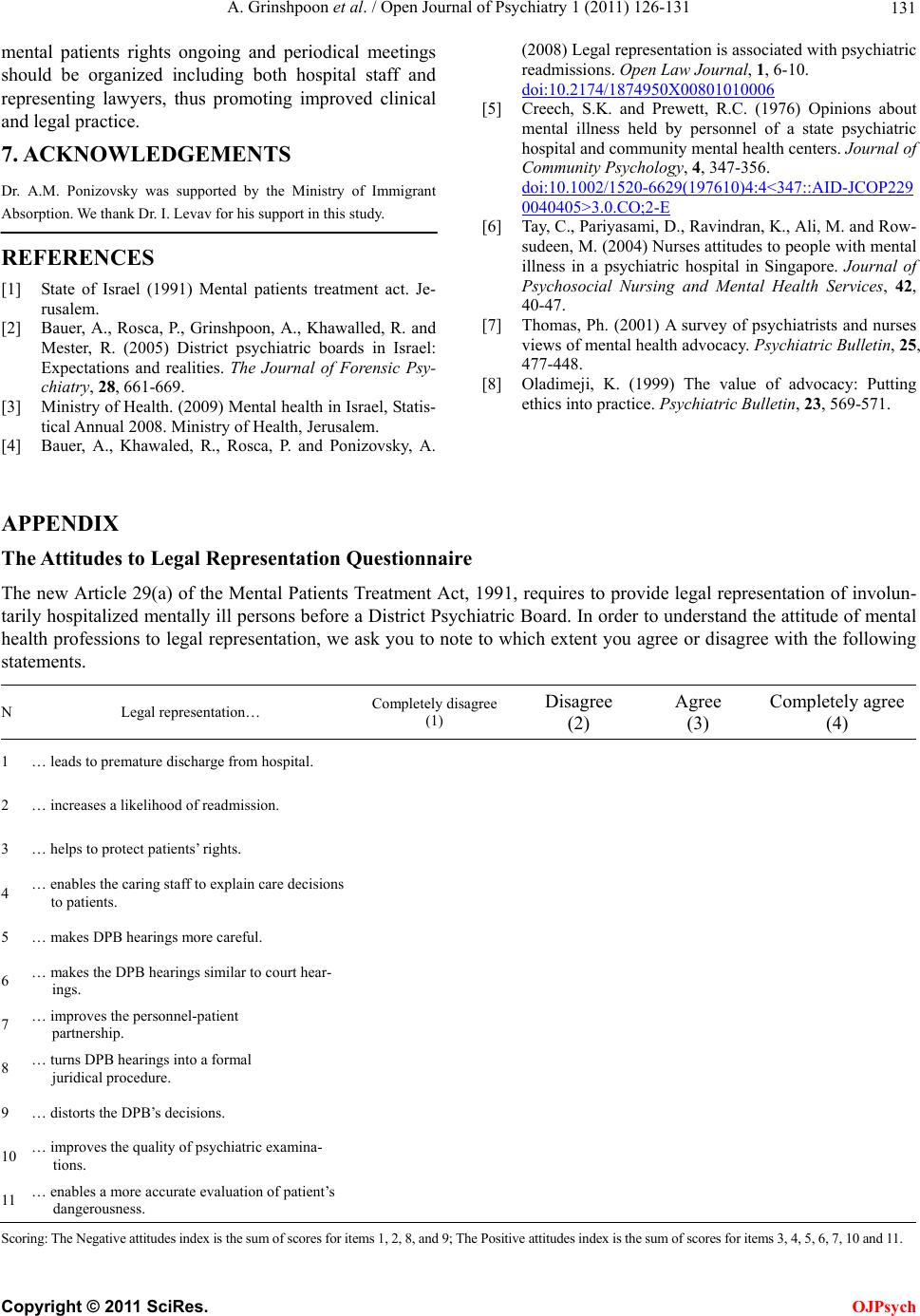
3.3. The Questionnaire
An “Attitudes to Legal Representation Questionnaire”
(ALRQ) was especially developed for the study (see
Appendix). The questionnaire consists of 11 items
grouped into two subscales: the positive and negative
attitudes subscales. The first reflects staff member no-
tions about the various benefits bound to legal represen-
tation of all participants in the process, whereas the sec-
ond subscale defines staff members’ concerns/beliefs
about the potential harm of LR. Correspondingly, the
positive attitudes subscale consists of 7 items: “LR helps
protect patients’ rights”; “LR enables the caring staff to
explain care decisions to patients”; “LR makes DPB
hearings more careful”; “LR makes the DPB similar to
court hearings”; “LR improves the personnel-patient
partnership”; “LR improves the quality of psychiatric
examinations”; and “LR enables a more accurate evalua-
tion of patients’ dangerousness”. The negative subscale
comprises 4 items: “LR leads to premature discharge
from hospital”; “LR increases a likelihood of readmis-
sion”; “LR turns DPB hearings into a formal juridical
procedure”, and “LR distorts the DPBs’ decisions”.
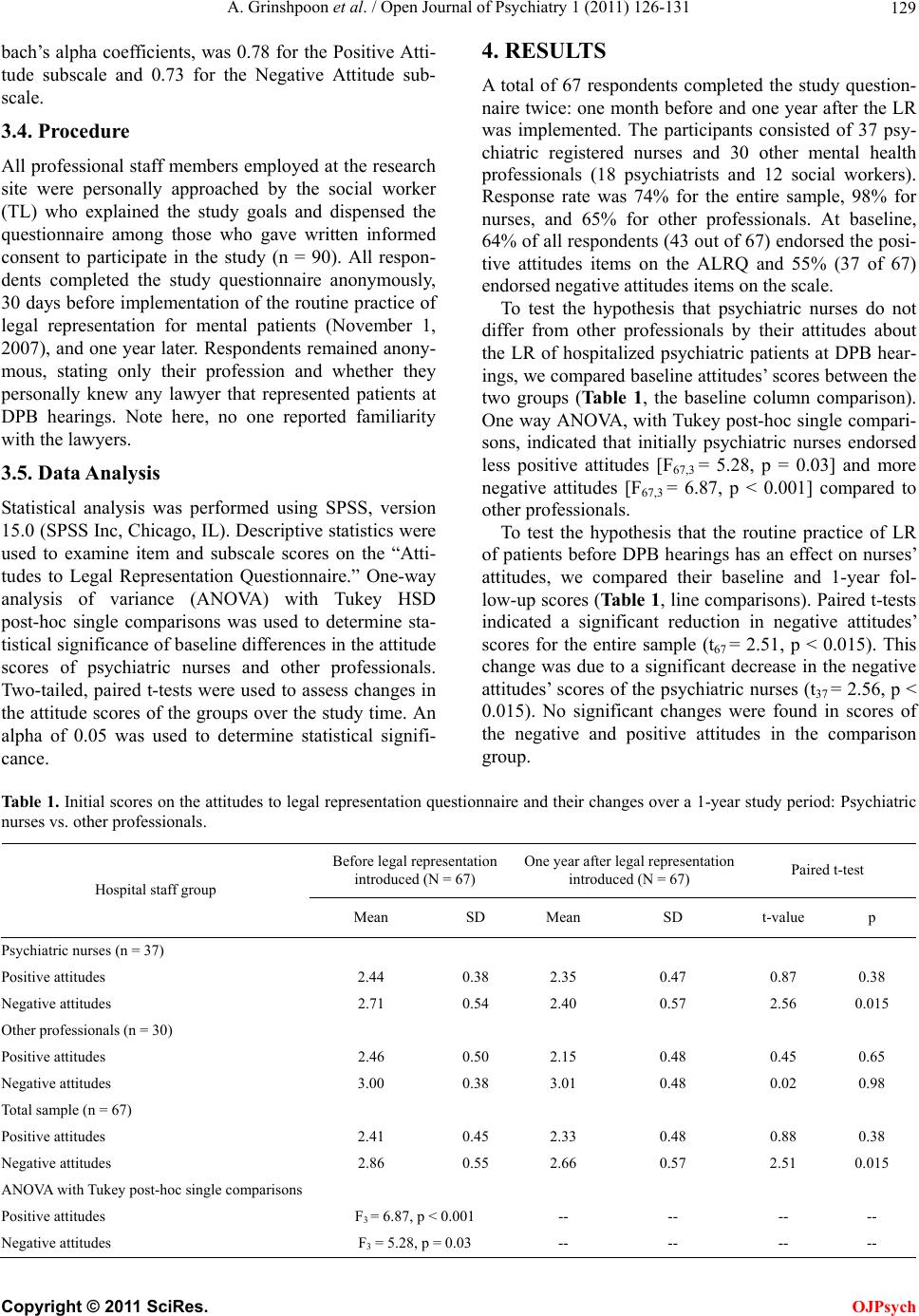
In the questionnaire, a respondent is asked to assess
his/her degree of agreement with each item. The re-
sponses are scored on a 4-point Likert scale: ‘Com-
pletely disagree’ (score 1), ‘Disagree’ (score 2), ‘Agree’
(score 3), and ‘Completely agree’ (score 4). Mean scores
for each subscale are calculated by summing item scores
divided by number of completed items. The cut off point
for the operational definition of positive and negative
attitude subscale score was established as 2.5. Thus, a
mean score lower than 2.5 indicates participant agree-
ment with the subscale items, whereas a mean score of
2.5 and over displays his/her disagreement. The internal
consistency of the ALRQ items, as measured by Cron-
Copyright © 2011 SciRes. OJPsych