J. Carter et al. / Open Journal of Obstetrics and Gynecology 1 (2011) 139-143 141
performed. Median and mean operating time was 2.5 and
2.3 hours respectively (Range: 1 - 5 hours). Sixteen (24%)
patients were classified as normal BMI and 50 (76%) as
overweight and obese (25 overweight and 25 obese).
Median and mean BMI were 28 kg/m2 and 30 kg/m2 re-
spectively (Range: 18 - 47).
Forty two patients (64%) had a “0” Performance
Status (PS), 20 (30%) had PS 1 and 4 (6%) had a PS of 2.
In total, 24 (36%) had “non-zero” performance status.
Median preoperative Hb was 129, dropping to 119
postoperatively.
Mean intraoperative EBL was 227 ml (95% CI: 189 -
266) with a median EBL of 188ml (Range: 10 ml - 900
ml). There were no intra or postoperative blood transfu-
sions.
Median and mean LOS was 3.0 and 3.7 days respec-
tively (Range: 2 - 16 days) with 10 (15%) patients dis-
charged on or before post operative day 2 and an addi-
tional 7 (2%) patients were deemed suitable for discharge
on day 2 but for social reasons were unable to be dis-
charged. Thirty eight (58%) patients were discharged on
day 3. T hree pa t i en t s (5%) had LOS greater than 7 days.
COX 2 inhibitors were prescribed to 58 (88%) and 62
(94%) were able to successfully complete EOF and FTS
protocol.
There were 3 (5%) intraoperative complications/ad-
verse events. Two were episodes of bradycardia related
to parietal peritoneum stimulation both settling and al-
lowing surgery to proceed. There was 1 intraoperative
bladder injury in a patient who underwent an exentera-
tive procedure, being a Jehovah’s Witness, having pre-
viously undergone an abdomino-perineal resection and
pelvic irradiation for colon cancer, presenting with se-
rous corpus cancer and her uterus fixed to the sacrum.
The bladder was morbidly fixed to the uterus as a con-
sequence of her previous irradiation and the bladder in-
advertently entered during dissection and repaired in 2
layers without sequelae. There was no intraoperative
ureteric, bowel or vascular injuries.
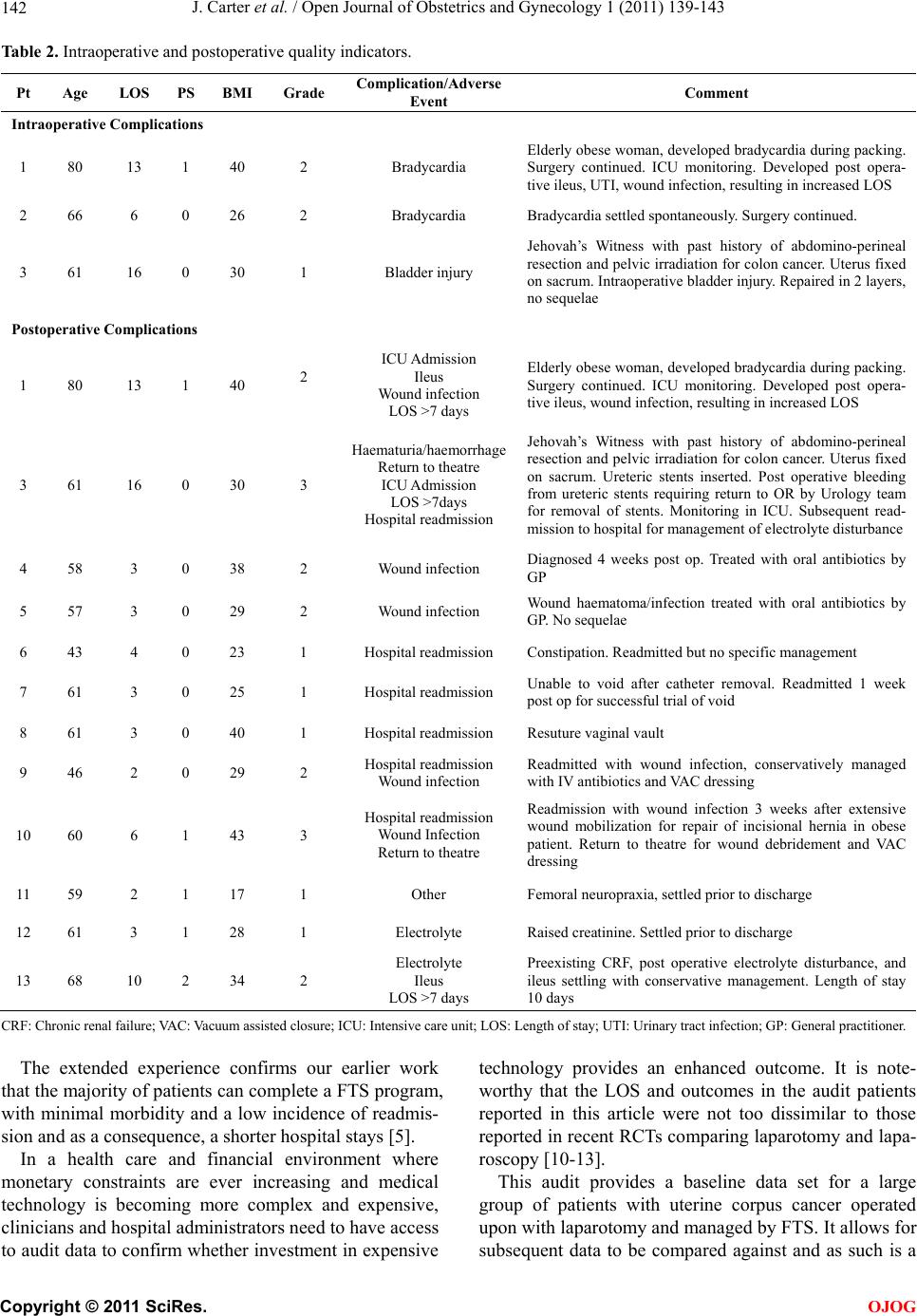
Postoperatively, 13 patents (20%) experienced a total
of 24 complications/adverse events based upon our KPI’s.
There were 6 (9%) hospital readmissions, 5 (8%) wou nd
infections, 3 patients (5%) whose LOS was greater than
7 days, 2 patients (3%) had an unplanned ICU admission,
2 developed an ileus (3%), 2 patients (3%) unplanned
return to theatres, 2 patients (3%) with electrolyte dis-
turbance and 1 each of the following were reported:
haemorrhage from ureteric stents and femoral neuro-
praxia as outlined in Table 2.
One patient (Patient 3) accounted for 5 of 23 (22%)
complications. Only 2 patients (patient 3 and patient 10)
experienced complications greater than grade 2. Patient 3
was a 61 year old, obese Jehovah’s Witness described
above with a past history of abdo mino-perineal r esection
and pelvic irradiation for colon cancer. She was diag-
nosed with a serous corpus cancer and her uterus was
fixed onto the sacrum as a consequence of previous treat-
ments. Intraoperativ ely ureteric stents were inserted. Post
operative bleeding from ureteric stents required her re-
turn to the operating room by the Urology team for re-
moval of ureteric stents, and monitoring in ICU an d sub-
sequent readmission to hospital for management of an
electrolyte disturbance. Patient 10 was a 60 year old
morbidly obese woman who underwent repair of an inci-
sional hernia by general surgical colleagues at the same
time as her uterine cancer surgery. She underwent exten-
sive soft tissue mobilisation an d was readmitted 3 weeks
after surgery with a wound infection that required de-
bridement in the operating room and VAC dressing
placement.
4. DISCUSSION
Patients commonly ask their surgeon “have you done this
before?” and “am I going to be OK?” The answer to
these questions are not derived from published RCTs,
rather they are derived from clinical audit of personal
experience.
Clinical audit is one of the fundamental principles of
clinical governance, the process by which clinicians im-
prove the quality of the care they provide. The process
involves regularly collecting and measuring activity and
outcomes, and analysing and comparing these outcomes
with current or “recognised standards”, together with a
rigorous peer review process. It makes clinicians ac-
countable to the public, by constantly monitoring and
maintaining high standards, being transparent and ac-
countable for those standards, identifying problems and
addressing them and to constantly improve on those
standards to improve overall quality of care. It is what
the public expect [7]. The key feature of audit is that it
involves reviewing actual and all surgical performance
outcomes. In lay terms, the purpose of audit is to confirm
that your outcomes are, what you say or think they are
[8]. It has been shown quite clearly from cardiac surgery
that structured data collection, analysis, and feedback to
clinicians improves the qu ality of outcomes [9].
Our study provides the first real base-line or “recog-
nised standard” on laparotomy patients managed by FTS
for the surgical management of uterine cancer.
In this audit, all patients with a diagnosis of uterine
corpus malignancy and managed by a FTS program were
included. During the study period there were no patients
who underwent laparo scopy and as such this audit repre-
sents extensive experience of fast track surgical care in
patients with uterine malignancy managed by laparotomy
and thus serves as a “recognised standard”.
C
opyright © 2011 SciRes. OJOG