R. L. Heaton et al. / Open Journal of Obstetrics and Genecology 1 (2011) 136-138
Copyright © 2011 Sc iRes. OJOG
Fi gure 3 . Florid glomerulations and Hunner’s ulcers of
the bladder consistent with typical interstitial cystitis.
Extensive lysis of adhesions, biopsying of pigmented
areas and laparoscopic excision of the round ligament
tumor were performed. Hysteroscopically, both cornua
appeared to be normal and open; there was no evidence
of submucosal pigmentations consistent with adenomy-
osis. Pathologic report showed endometriosis and the
round ligament t umor proved to be a leiomyoma. Opera-
tive time was 65 minutes and blood loss was estimated at
100 cc.
3. LAPARO SCOPIC TECHNIQUE
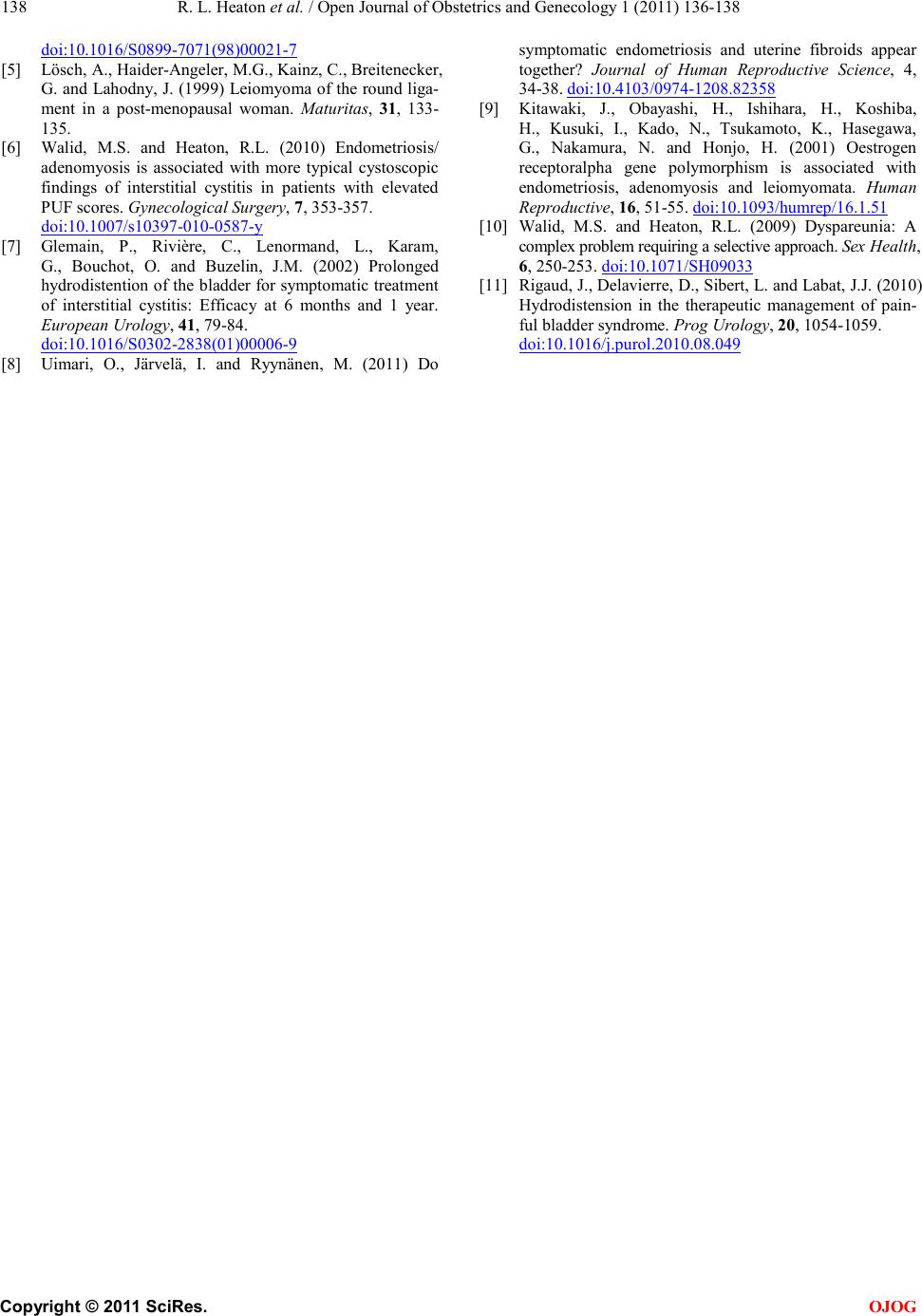
The leiomyomatous tumor was located at the anterio-
lateral left ju nction o f the r ound ligame nt with t he per ito-
neum. Laparoscopic removal of interligementous fib-
roids is accomplished by traction counter traction with
either sharp or harmonic dissection taking care to coagu-
late any bleeding sites as encountered, to maintain a dry
field and optimal visualization to avoid injury to su-
rrounding structures. Removal of a tumor, if small, can
be done with an endopouch, and if large, morcellation is
required.
4. COMMENTARY
Intra-ligamentous fibroids affecting the round ligament
are not common. During a busy gynsurgical career we
have seen intraligamentous fibroids involving the labia
majora, the lower third of the right lateral vaginal wall,
and the broad ligament of the uterus. It is important to
remember that a solid tumor any where in t he pelvi s ma y
be a fibroid. These misplaced tumors usually lead to
exploratory surgery to rule out more sinister lesions.
Since fibroids are hormone-sensitive they tend to grow
until menopause or until they outgrow their blood supply.
Therefore when seen during diagnostic laparoscopy it is
our recommendation to remove them and prevent a sub-
sequent exploratory surgery.
The other interesting aspect of this case is the coe-
xistent endometriosis and interstitial cystitis. We have
previously reported that in our retrospective series there
was a 60% comorbid state with endometriosis or adeno-
myosis when Interstitial cystitis (IC) is present [6]. We
are disturbed by the de-emphasis of the importance of
cystoscopy with hydrodistension in the evaluation of
possible IC. With such a high rate of comorbid disease, if
the patient is already under anesthesia for evaluation of
pelvic pain laparoscopically why would one pass up the
opportunity to diagnose a frequent comorbid disease and
get prognostic information based on anesthetic bladder
capacity? As it appears that prognosis for remission is
good with normal bladder capacity and progressively
worse ns with loss of bladder capacity [7]. Also since the
symptom complex for adenomyosis and endometriosis
overlap and adenomyosis can be confirmed but not ex-
cluded hysteroscopically it seems somewhat negligent
not to hysteroscope these patients. The senior author (Dr.
Heaton) in the past used a resectoscope to biopsy pig-
mented submucosal uterine lesions; the pathology unifor-
mally revealed ademomyosis. Endometriosis, adenomy-
osis and leio myomata develop in wome n of reprod uctive
age and regress after menopause or removal of ovaries,
indicating t hat they grow in an estrogen-dependent man-
ner. These diseases appear to have some co mmo n patho-
genetic pathways [8]. A recent study suggested that the
PVUII polymorphism of the ERalpha gene is associated
with the risk for end ometriosis, ade nomyosis, and leio m-
yomata [9].
We have reported previously on the common multi-
factorial nature of chronic pelvic pain [10]. This patient
is yet another example of this concept. It is our opinion
that if a patient has e no ugh cyclic pelvic pain to indicate
laparoscopy then hysteroscopy is warranted as well to
evaluate for possible adenomyosis. If endometriosis or
adenomyosis or an elevated PUF score is present it is
also our opinion that with the patient already asleep for
laparoscopy failing to take t he opportunity to confirm the
diagnosis of IC and obtain prognostic informatio n seems
to be less than optimal care especially with the patients
having a 50% chance of temporary relieve of IC sym-
ptoms for several mo nths after hydrodistension [7,11 ].
REFERENCES
[1] Mi chel, P. and HViola, DH. (2003) Abdomino-pelvic leiom-
yoma of the round ligament: Contribution of computed
tomography and magnetic resonance imaging. Journal of
Gynecology and Obstetric Bio logy R e p ro ductive, 32, 571-
574.
[2] HVignali, MH., HBertul es si, CH., HSpreafico, CH. and HBusacca, MH.
(2006) A large symptomatic leiomyoma of the round
ligament. Minimally Invasive Gynecology, 13, 375-376.
Hdoi:10.1016/j.jmig.2006.03.008
[3] HGrossman, S.LH. and Cheung, V.Y. (1999) Round liga-
ment fibroid. Journal of Ob st etrics and Gynaecology of
Canadian, 29, 109-110.
[4] Warshauer, D.M. and Mandel, S.R. (1999) Leiomyoma of
the extra-peritoneal round ligament: CT demonstration.
Clinical Imaging, 23, 375-376.