D. J. Witter et al. / Open Journal of Stomatology 1 (2011) 69-74 73
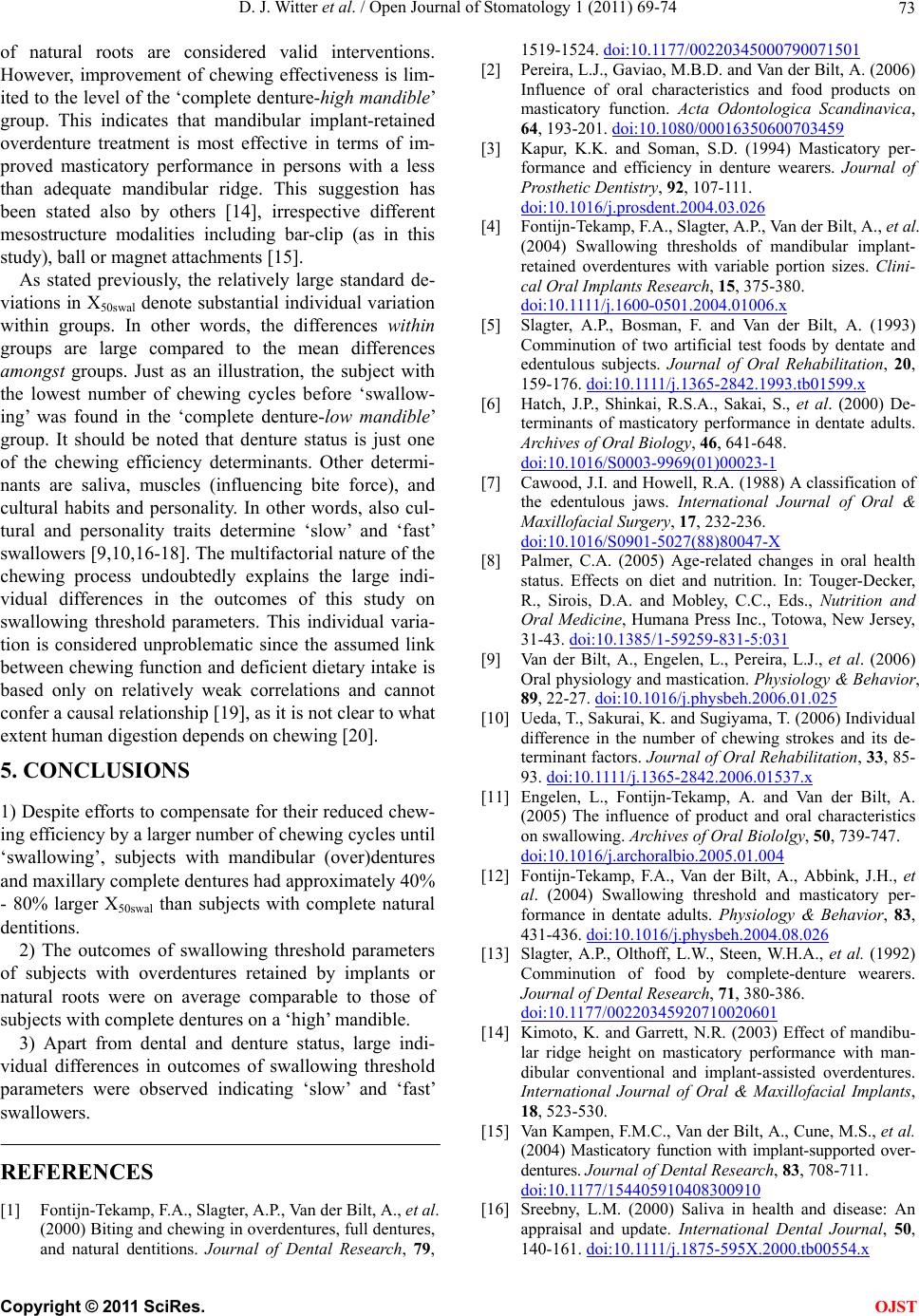
of natural roots are considered valid interventions.
However, improvement of chewing effectiveness is lim-
ited to the level of the ‘complete denture-high mandible’
group. This indicates that mandibular implant-retained
overdenture treatment is most effective in terms of im-
proved masticatory performance in persons with a less
than adequate mandibular ridge. This suggestion has
been stated also by others [14], irrespective different
mesostructure modalities including bar-clip (as in this
study), ball or magnet attachments [15].
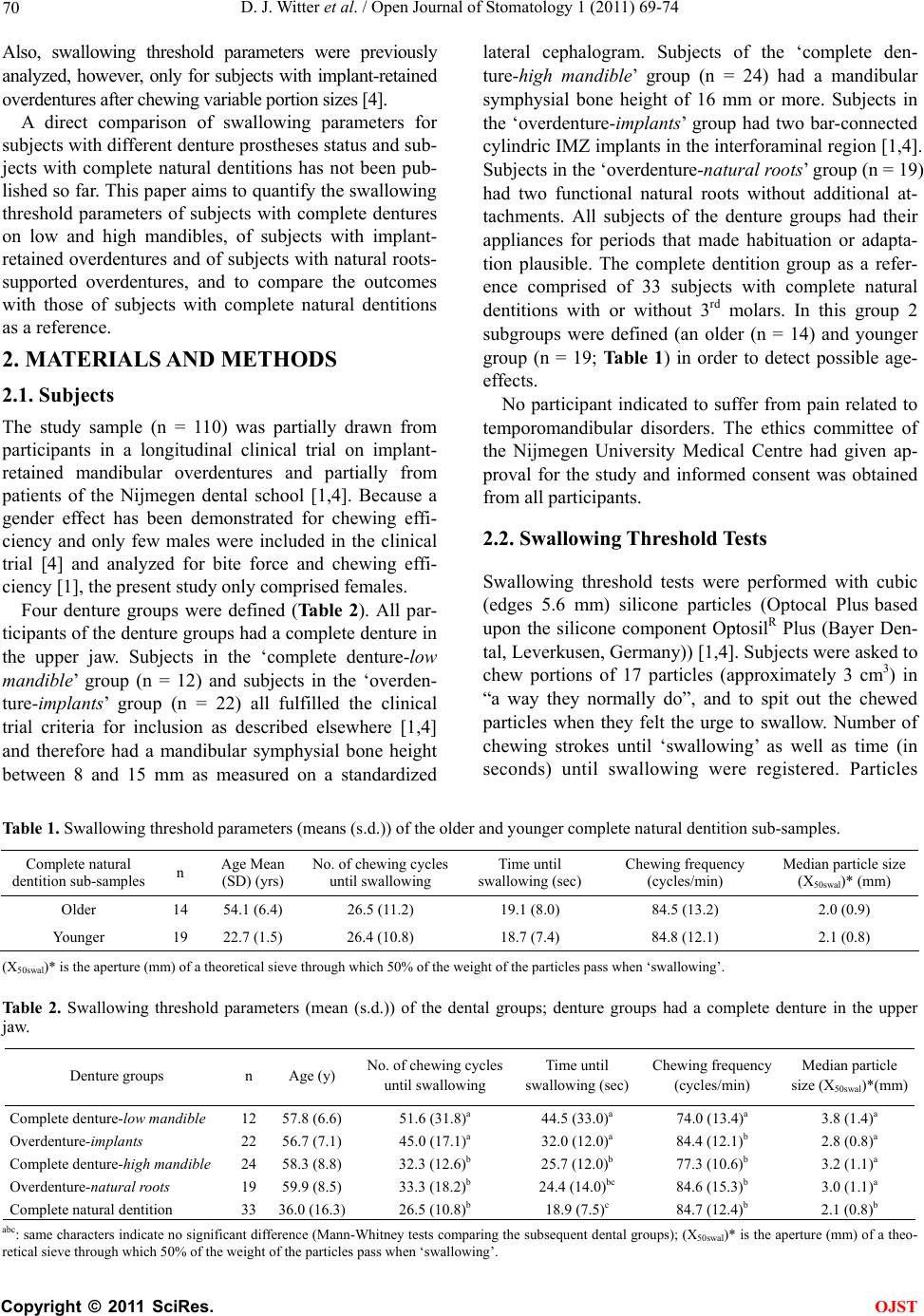
As stated previously, the relatively large standard de-
viations in X50swal denote substantial individual variation
within groups. In other words, the differences within
groups are large compared to the mean differences
amongst groups. Just as an illustration, the subject with
the lowest number of chewing cycles before ‘swallow-
ing’ was found in the ‘complete denture-low mandible’
group. It should be noted that denture status is just one
of the chewing efficiency determinants. Other determi-
nants are saliva, muscles (influencing bite force), and
cultural habits and personality. In other words, also cul-
tural and personality traits determine ‘slow’ and ‘fast’
swallowers [9,10,16-18]. The multifactorial nature of the
chewing process undoubtedly explains the large indi-
vidual differences in the outcomes of this study on
swallowing threshold parameters. This individual varia-
tion is considered unproblematic since the assumed link
between chewing function and deficient dietary intake is
based only on relatively weak correlations and cannot
confer a causal relationship [19], as it is not clear to what
extent human digestion depends on chewing [20].
5. CONCLUSIONS
1) Despite efforts to compensate for their reduced chew-
ing efficiency by a larger number of chewing cycles until
‘swallowing’, subjects with mandibular (over)dentures
and maxillary complete dentures had approximately 40%
- 80% larger X50swal than subjects with complete natural
dentitions.
2) The outcomes of swallowing threshold parameters
of subjects with overdentures retained by implants or
natural roots were on average comparable to those of
subjects with complete dentures on a ‘high’ mandible.
3) Apart from dental and denture status, large indi-
vidual differences in outcomes of swallowing threshold
parameters were observed indicating ‘slow’ and ‘fast’
swallowers.
REFERENCES
[1] Fontijn-Tekamp, F.A., Slagter, A.P., Van der Bilt, A., et a l.
(2000) Biting and chewing in overdentures, full dentures,
and natural dentitions. Journal of Dental Research, 79,
1519-1524. doi:10.1177/00220345000790071501
[2] Pereira, L.J., Gaviao, M.B.D. and Van der Bilt, A. (2006)
Influence of oral characteristics and food products on
masticatory function. Acta Odontologica Scandinavica,
64, 193-201. doi:10.1080/00016350600703459
[3] Kapur, K.K. and Soman, S.D. (1994) Masticatory per-
formance and efficiency in denture wearers. Journal of
Prosthetic Dentistry, 92, 107-111.
doi:10.1016/j.prosdent.2004.03.026
[4] Fontijn-Tekamp, F.A., Slagter, A.P., Van der Bilt, A., et a l.
(2004) Swallowing thresholds of mandibular implant-
retained overdentures with variable portion sizes. Clini-
cal Oral Implants Research, 15, 375-380.
doi:10.1111/j.1600-0501.2004.01006.x
[5] Slagter, A.P., Bosman, F. and Van der Bilt, A. (1993)
Comminution of two artificial test foods by dentate and
edentulous subjects. Journal of Oral Rehabilitation, 20,
159-176. doi:10.1111/j.1365-2842.1993.tb01599.x
[6] Hatch, J.P., Shinkai, R.S.A., Sakai, S., et al. (2000) De-
terminants of masticatory performance in dentate adults.
Archives of Oral Biology, 46, 641-648.
doi:10.1016/S0003-9969(01)00023-1
[7] Cawood, J.I. and Howell, R.A. (1988) A classification of
the edentulous jaws. International Journal of Oral &
Maxillofacial Surgery, 17, 232-236.
doi:10.1016/S0901-5027(88)80047-X
[8] Palmer, C.A. (2005) Age-related changes in oral health
status. Effects on diet and nutrition. In: Touger-Decker,
R., Sirois, D.A. and Mobley, C.C., Eds., Nutrition and
Oral Medicine, Humana Press Inc., Totowa, New Jersey,
31-43. doi:10.1385/1-59259-831-5:031
[9] Van der Bilt, A., Engelen, L., Pereira, L.J., et al. (2006)
Oral physiology and mastication. Physiology & Behavior,
89, 22-27. doi:10.1016/j.physbeh.2006.01.025
[10] Ueda, T., Sakurai, K. and Sugiyama, T. (2006) Individual
difference in the number of chewing strokes and its de-
terminant factors. Journal of Oral Rehabilitation, 33, 85-
93. doi:10.1111/j.1365-2842.2006.01537.x
[11] Engelen, L., Fontijn-Tekamp, A. and Van der Bilt, A.
(2005) The influence of product and oral characteristics
on swallowing. Archives of Oral Biololgy, 50, 739-747.
doi:10.1016/j.archoralbio.2005.01.004
[12] Fontijn-Tekamp, F.A., Van der Bilt, A., Abbink, J.H., et
al. (2004) Swallowing threshold and masticatory per-
formance in dentate adults. Physiology & Behavior, 83,
431-436. doi:10.1016/j.physbeh.2004.08.026
[13] Slagter, A.P., Olthoff, L.W., Steen, W.H.A., et al. (1992)
Comminution of food by complete-denture wearers.
Journal of Dental Research, 71, 380-386.
doi:10.1177/00220345920710020601
[14] Kimoto, K. and Garrett, N.R. (2003) Effect of mandibu-
lar ridge height on masticatory performance with man-
dibular conventional and implant-assisted overdentures.
International Journal of Oral & Maxillofacial Implants,
18, 523-530.
[15] Van Kampen, F.M.C., Van der Bilt, A., Cune, M.S., et al.
(2004) Masticatory function with implant-supported over-
dentures. Journal of Dental Research, 83, 708-711.
doi:10.1177/154405910408300910
[16] Sreebny, L.M. (2000) Saliva in health and disease: An
appraisal and update. International Dental Journal, 50,
140-161. doi:10.1111/j.1875-595X.2000.tb00554.x
C
opyright © 2011 SciRes. OJST