K. Shashikala et al. / Open Journal of Stomatology 1 (2011) 55-60 59
our knowledge of the demineralization and remineraliza-
tion process [13]. The administration of fluoride has
been proposed, and used, as a method of reducing
enamel susceptibility to decalcification since the time it
was discovered in the early 20th century by eminent
investigators like McKay and Black [5]. Fluoride affects
the caries process by enabling the formation of high
quality fluorapatite that aids remineralization and inhib-
its glycolysis of plaque microorganisms [6]. The early
attempts to incorporate fluoride into toothpastes which
dates back to the 1960s and it is one of the most com-
mon and effective modes of topical fluoride delivery [7].
Hence, in the present study a non-fluoridated denti-
frice has been used as a control along with two higher
concentrations of fluoride, that is 500 ppm and 1000
ppm for comparison. The study was designed in such a
way that it simulated an oral environment subjected to
acid and remineralization twice a day.
Monitoring demineralization and remineralization of
dental hard tissues is essential for the prevention and
minimally invasive treatment of dental caries and hy-
persensitivity [8]. Light based methods used for the de-
tection of dental caries induced enamel demineralization
are Conventional radiography, micro radiography, Digi-
tal Imaging Fiber Optic Trans illumination Imaging
[DIFOTI], laser induced fluorescence [DIAGNO dent],
and quantitative light-induced fluorescence [QLF]. Con-
ventional microscopy suffers from the problem as light
scattering, namely multiple scattering from objects that
are out of focus within the illuminated region prevents
imaging deep within a sample. Further, if care is not
taken, optical microscopy can lead to the observation of
certain artifacts which in turn leads to incorrect physical
interpretation of the system in question [3 ,9].
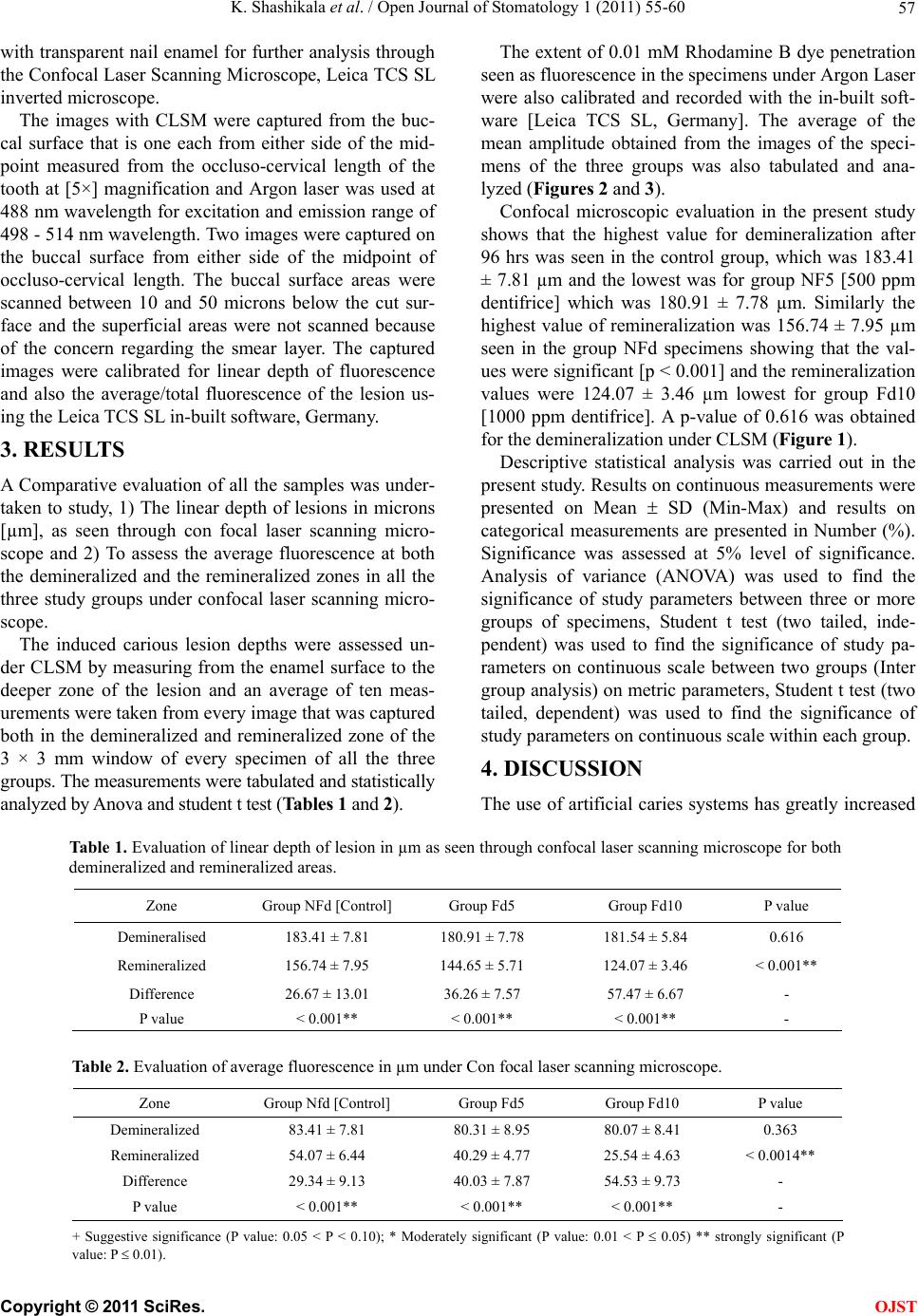
Confocal microscopy and its application in dentistry
have been advocated by Watson [9]. CLSM overcomes
the limitations of conventional wide-field microscopy
through: high resolution fluorescence, high resolution
3-D imaging, non-destructive imaging technique and
in-situ characterization of tissue microstructure images.
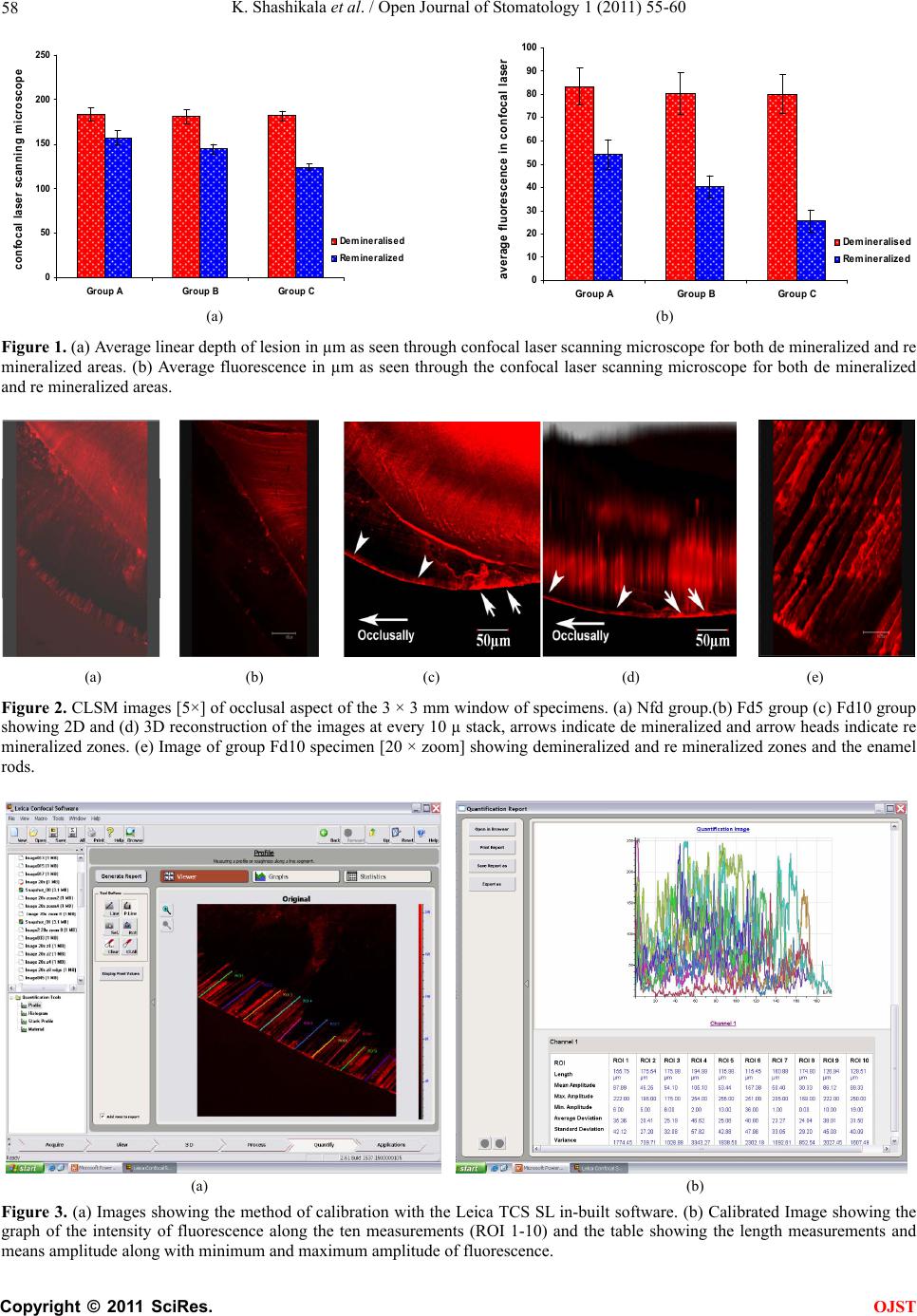
Fontana performed a study to correlate area of lesion,
average fluorescence and total fluorescence obtained by
con focal microscopy to lesion depth and mineral loss
obtained from micro radiography and polarized light
microscopy. The findings show that when a 0.1 mM so-
lution of rhodamine B dye was used, the lesion area cor-
related well with the mineral loss obtained from micro
radiography [10].
However, the average lesion fluorescence best repre-
sented mineral loss, based on their hypothesis that rho-
damine B penetrates the voids and pores created during
enamel demineralization which is a better method of
evaluation over the birefringence through CLSM. Ca-
bezas also conducted a correlation study between micro
radiography and con focal microscopy for measurement
of enamel remineralization. As described by Fontana, 0.1
mM rhodamine B dye was used and lesion area, total
fluorescence and average fluorescence were evaluated.
Lesion area was the confocal parameter that showed the
strongest correlation with microradiography, followed by
total lesion fluorescence [8,10].
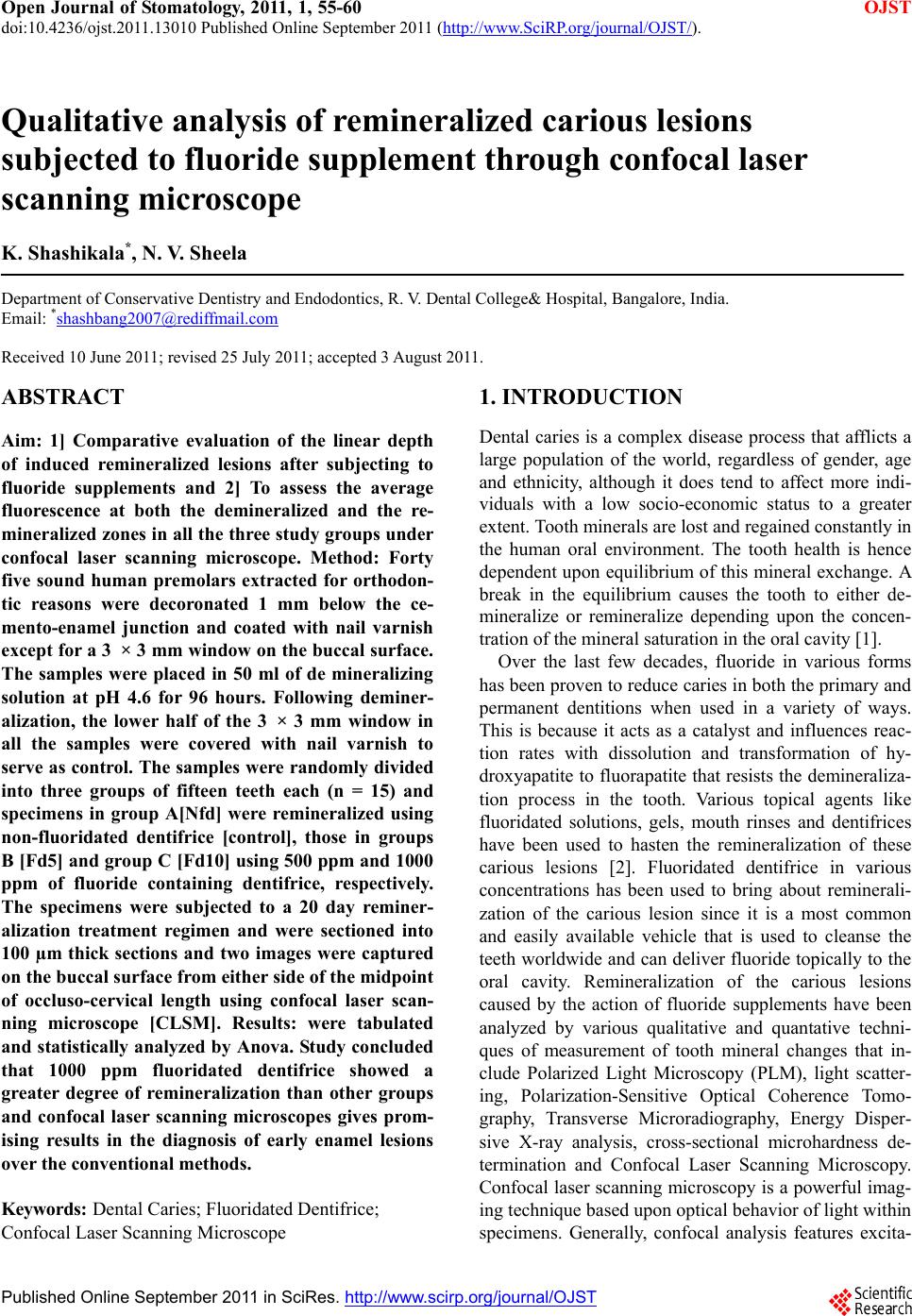
The present study showed a lesser degree of reminer-
alization with the non-fluoridated dentifrices which was
similar to the study by Gonzalez [10], who had used 250
ppm and 1100 ppm dentifrices along with a placebo con-
trol. It was also seen in the study that the linear depth
measurements of the lesion both in the de mineralized
zone and the re mineralized zone varied significantly
under the con focal microscopic. This is on par with the
analysis by the earlier studies [11,12] showing that con
focal microscopy is an advanced tool to diagnose and
measure early enamel lesions both in-vivo and in-vitro
without requiring the tooth to be sectioned.
Fluorides are effective means of remineralization of
carious lesions in higher concentrations (1000 ppm) as
compared to the non-fluoridated control or 500 ppm
concentration [13]. Diagnosis of early enamel carious
lesions still remains a challenge to dentists worldwide.
Various in-vitro studies show promising results with con
focal laser scanning microscope as a diagnostic aid for
early carious lesion detection. This appro ach will enable
the operator to circumvent errors due to variation in the
thickness of enamel at different locations of the crown.
Recent evolution in techniques and technologies have
facilitated a relatively wide spread adoption of this im-
aging diagnostic modality with increased “user friendli-
ness and flexibility”. Study concluded that 1000 ppm
fluoridated dentifrice showed a greater degree of remin-
eralization than other groups and con focal laser scan-
ning microscopes gives promising results in the diagno-
sis of early enamel lesions over the conventional meth-
ods.
REFERENCES
[1] Sturdevant, C.M., Roberson, T.M. and Heymann, H.O.
(2006) The art and science of operative dentistry. 5th
Edition, Mosby Publishers, St. Louis.
[2] Queiroz, C.S. and Hara, A.T. (2008) PH-cycling models
to evaluate the effect of low fluoride dentifrice on enamel
de- and remineralization. Brazilian Dental Journal, 19,
21-27. doi:10.1590/S0103-64402008000100004
[3] Kishen, A., Shrestha, A. and Rafique, A. (2008) Fiber
optic backscatter spectroscopic sensor to monitor enamel
demineralization and remineralization in vitro. Journal of
Conservative Dentistry, 11, 63-70.
doi:10.4103/0972-0707.44053
[4] Ferriera-Zandona, A.G., Analoui, M. and Beiswanger,
C
opyright © 2011 SciRes. OJST