Open Jo urnal of Obstetr ics and Gynecology, 2011, 1, 124-127 OJOG
doi:10.4236 /ojog.2011.13022 Published Online Sept e mb er 2011 (http://www.SciRP.org/journ al/ojog/).
Published Online September 2011 in SciRes. http://www.scirp.org/journal/OJOG
An unusual case of ovarian torsi on w ith infarction simulating
malignancy in an adolescent girl
Madhu Jain1*, Kusum Lata1, Shivi Jain2
1Department of Obstetr ics & Gynecology, In s titute o f Medical Sciences, B anaras Hindu University, Varanasi, I ndia;
2Department of Obstetr ics & Gynecology and Radiology, Inst itute of Medical Sciences, Banaras Hindu University, Varanasi, Indi a
E-mai l : *
Hdrmadhujainbhu@gmail.com
Received 11 June 2011; revised 20 August 2011; accepted 27 August 2011.
ABSTRACT
Torsion of the ovary is an uncommon condition. It is
the 5th most common gynaecological emergency. It
most commonly occur in reproductive age group, on
right side, often in presence of congenital abnormali-
ties of adnexa but may occur in their absence too.
Adnexal torsion often poses a diagnostic challenge
because of non specific symptoms of presentation.
Ultrasound with colour Doppler ma y be helpful.
Keywords: Adenexal Torsion; Ovarian Infarction;
Colour Doppler
1. INTRODUCTION
Torsion of uterine adnexa is an uncommon condition.
Torsion of ovary is still uncommon. Despite of being
uncommon this is the 5th most common gynaecological
emergency [1], representing 3% of the emergency gy-
naecological surgeries [2]. Adnexal torsion is a diagno-
stic dilemma largel y because of the non specific clinical,
laboratory, and imaging findi ngs [3].
2. CASE REPORT
A 15 year old unmarried girl Miss M.R., presented in our
out patient department with the complains of dull ac hing
pain in lower abdomen for one year. It was more on right
side, episodic, non radiating, not responding to medica-
tions. The pain was increased in severity for last five to
six days. It was consta nt, radiating to suprap ub ic region,
with some relief on medication not associated with nau-
sea or vomiting. For this ultrasound was done in a pri-
vate hospital and told of having some tumour. She de-
nied o f ha ving an y ga s tr oi nte s t ina l o r genito uri na r y s ym-
ptoms. She achieved menarche one year back. Her
cycles were irregular at 2 - 3 mo nths, o f 8 - 10 days du-
ration with average flow. Her last menstrual period was
seven days back.
On examination she was alert, oriented and in severe
agony due to the pain. Her temperature was normal, re-
spiratory rate was 16 breaths/min, heart rate was 88
beats/min, and blood pressure was 110/70 mm Hg. Her
secondary sexual characters were normally developed.
Her cardiovascular and respiratory examinations were
unremarkable. Abdominal examination revealed a firm
lump in the lower abdomen of approximately 24 weeks
size involving iliac fosae, both lumbar, umbilical and
hypogastric areas. It was immobile, tender, overlying
skin was normal looking, lower ma rgins wer e not re ached.
She had no hepatosplenomegaly and bowel sounds were
normal. In per rectal examination, rectal mucosa was
free and fullness was felt anteriorly.
A pelvic ultrasound with colour Doppler was per-
formed, showing a large heterogeneous well defined
elongated pelvic mass of 17.3 × 11.1 × 9 cm, arising
from right adnexa with multiple cystic areas and right
sided subhepatic extension, suggestive of ovarian mass
(Fi gure 1). T here wa s no signific ant colour Do ppler flow.
Both ovaries were not visualized separately. How- ever
CECT pelvis revealed heterodense solid cystic mass
lesion in pelvis arising from right adnexal region with
mild pelvic ascites and mesenteric fat stranding, en-
larged pelvic lymph node, suggestive of malignant right
ovarian mass (Figure 2(a), 2(b)). MRI also reported a
well de fine d pre domina ntly c ystic ma ss a nd an eccentric
solid component, with an extension and encasement of
right distal commo n iliac, proximal exter nal iliac and in-
filtration of neurovascular bundle, suggestive of Germ
cell tumour with possibility of malignant degeneration
(Figure 3(a), 3(b)). Patient was also evaluated with
tumour markers such as LDH,
β
-HCG, Ca-125 & α-
fetoprotein, out of which only LDH was mildly in-
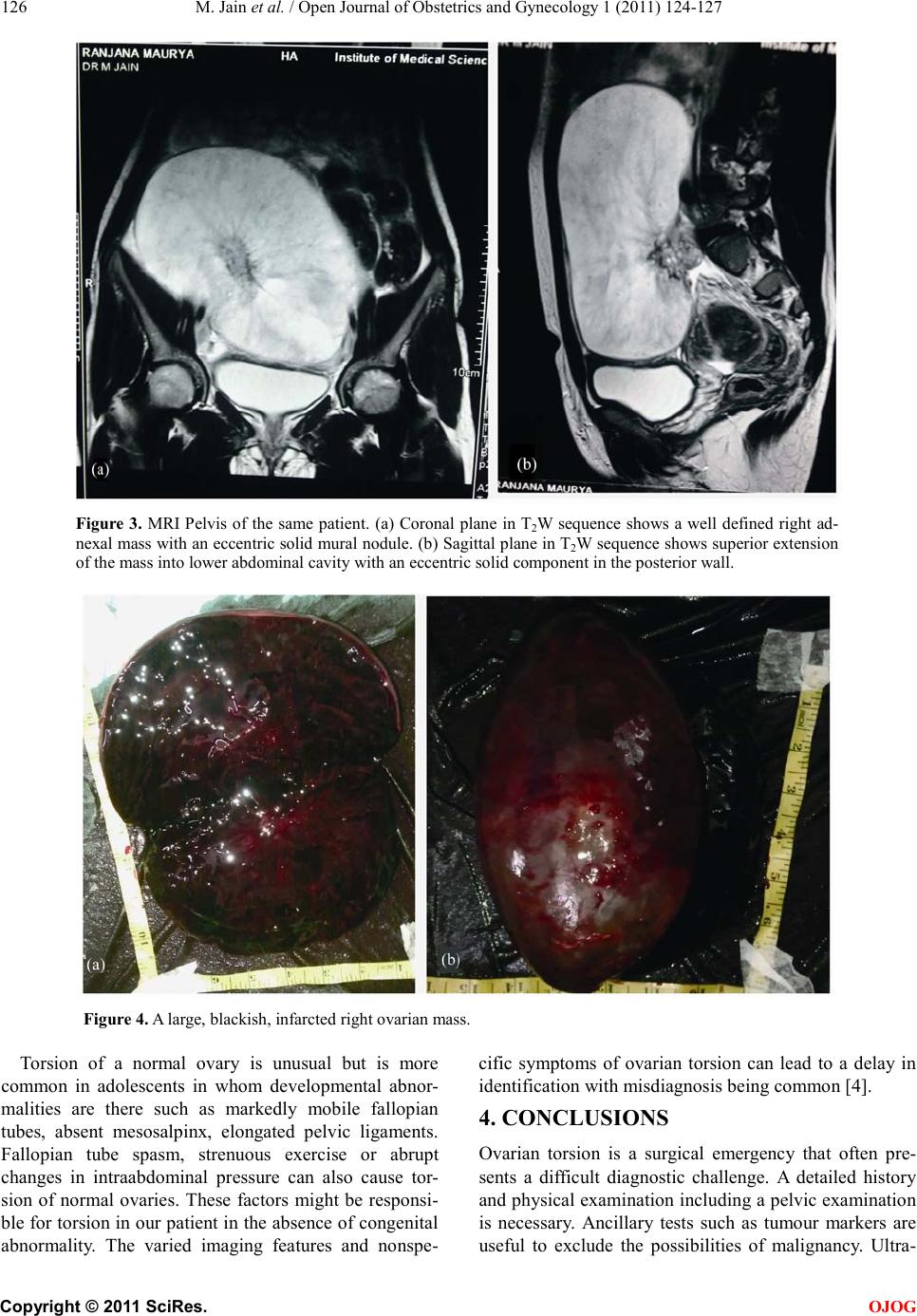
creased. Laparotomy was done after proper evaluation. A
large blackish right ovarian mass of approximately 25 ×
15 cm was present (Fi g u re 4). On delivering the ovary
out, 4 - 5 twist was present around ovarian ligament.
Histo patholo gy turne d out to , the ri ght ovar ian hae morr-
hagic cyst.