Paper Menu >>
Journal Menu >>
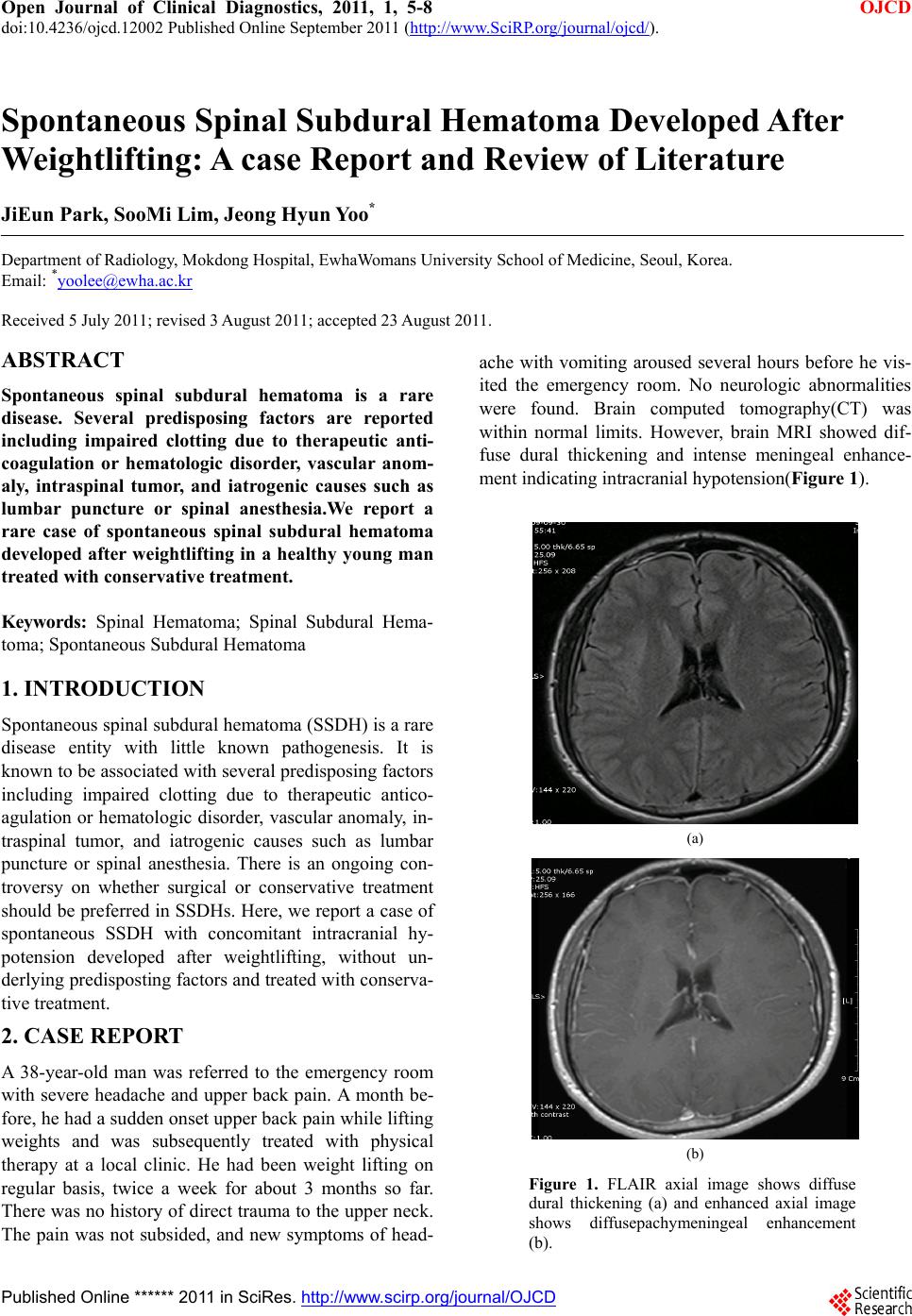 Open Journal of Clinical Diagnostics, 2011, 1, 5-8 OJCD doi:10.4236/ojcd.12002 Published Online September 2011 (http://www.SciRP.org/journal/ojcd/). Published Online ****** 2011 in SciRes. http://www.scirp.org/journal/OJCD Spontaneous Spinal Subdural Hematoma Developed After Weightlifting: A case Report and Review of Literature JiEun Park, SooMi Lim, Jeong Hyun Yoo* Department of Radiology, Mokdong Hospital, EwhaWomans University School of Medicine, Seoul, Korea. Email: *yoolee@ewha.ac.kr Received 5 July 2011; revised 3 August 2011; accepted 23 August 2011. ABSTRACT Spontaneous spinal subdural hematoma is a rare disease. Several predisposing factors are reported including impaired clotting due to therapeutic anti- coagulation or hematologic disorder, vascular anom- aly, intraspinal tumor, and iatrogenic causes such as lumbar puncture or spinal anesthesia.We report a rare case of spontaneous spinal subdural hematoma developed after weightlifting in a healthy young man treated with conservative treatment. Keywords: Spinal Hematoma; Spinal Subdural Hema- toma; Spontaneous Subdural Hematoma 1. INTRODUCTION Spontaneous spinal subdural hematoma (SSDH) is a rare disease entity with little known pathogenesis. It is known to be associated with several predispo sing factor s including impaired clotting due to therapeutic antico- agulation or hematologic disorder, vascular anomaly, in- traspinal tumor, and iatrogenic causes such as lumbar puncture or spinal anesthesia. There is an ongoing con- troversy on whether surgical or conservative treatment should be preferred in SSDHs. Here, we report a case of spontaneous SSDH with concomitant intracranial hy- potension developed after weightlifting, without un- derlying predisposting factors and treated with conserva- tive treatment. 2. CASE REPORT A 38-year-old man was referred to the emergency room with severe headache and upper back pain. A month be- fore, he had a sudden onset upper back pain while lifting weights and was subsequently treated with physical therapy at a local clinic. He had been weight lifting on regular basis, twice a week for about 3 months so far. There was no history of direct trauma to the upper neck. The pain was not subsided, and new symptoms of head- ache with vomiting aroused several hours before he vis- ited the emergency room. No neurologic abnormalities were found. Brain computed tomography(CT) was within normal limits. However, brain MRI showed dif- fuse dural thickening and intense meningeal enhance- ment indicating intracranial hypotension(Figure 1). (a) (b) Figure 1. FLAIR axial image shows diffuse dural thickening (a) and enhanced axial image shows diffusepachymeningeal enhancement (b). 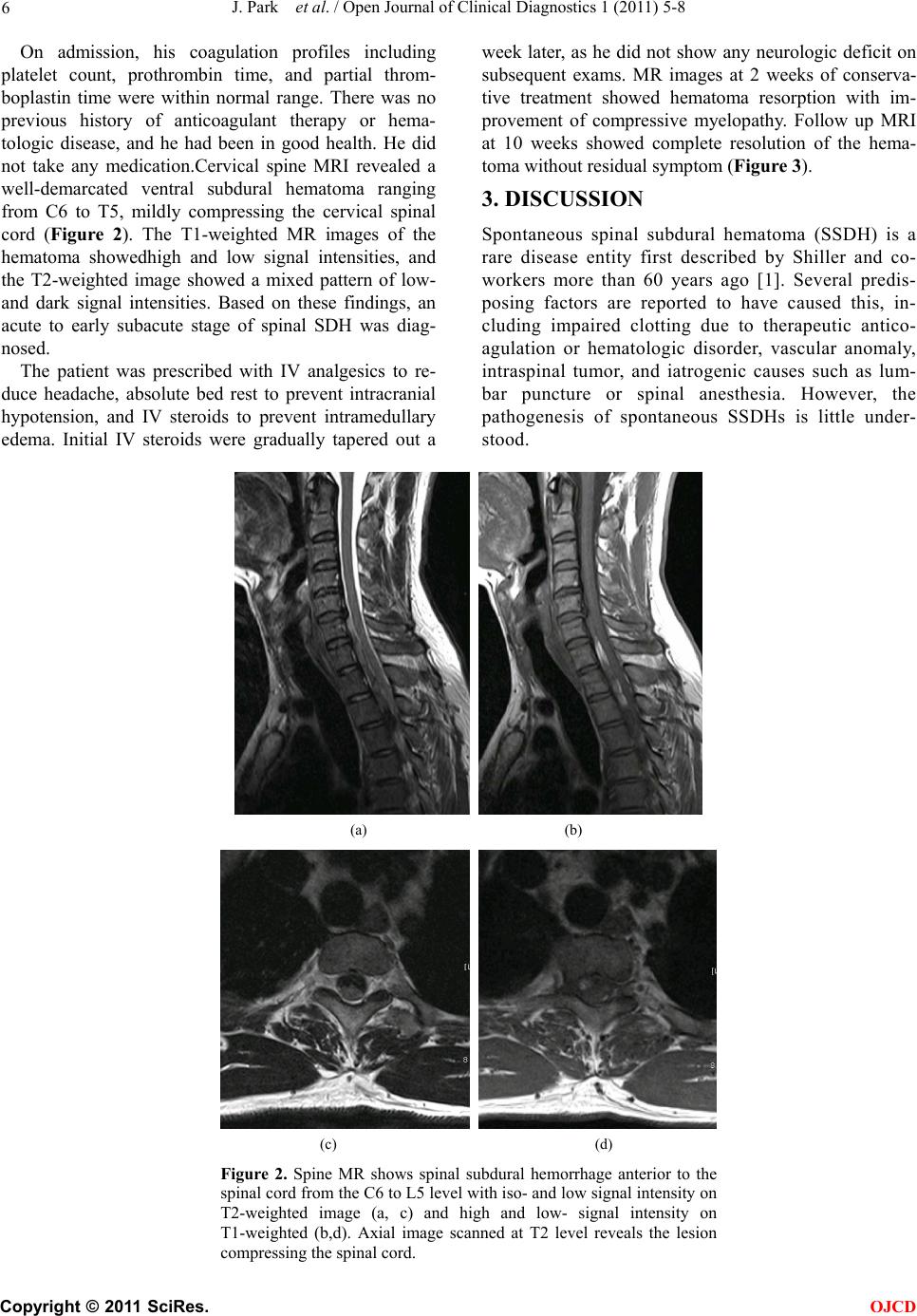 J. Park et al. / Open Journal of Clinical Diagnostics 1 (2011) 5-8 Copyright © 2011 SciRes. OJCD 6 On admission, his coagulation profiles including platelet count, prothrombin time, and partial throm- boplastin time were within normal range. There was no previous history of anticoagulant therapy or hema- tologic disease, and he had been in good health. He did not take any medication.Cervical spine MRI revealed a well-demarcated ventral subdural hematoma ranging from C6 to T5, mildly compressing the cervical spinal cord (Figure 2). The T1-weighted MR images of the hematoma showedhigh and low signal intensities, and the T2-weighted image showed a mixed pattern of low- and dark signal intensities. Based on these findings, an acute to early subacute stage of spinal SDH was diag- nosed. The patient was prescribed with IV analgesics to re- duce headache, absolute bed rest to prevent intracranial hypotension, and IV steroids to prevent intramedullary edema. Initial IV steroids were gradually tapered out a week later, as he did not show any neurologic deficit on subsequent exams. MR images at 2 weeks of conserva- tive treatment showed hematoma resorption with im- provement of compressive myelopathy. Follow up MRI at 10 weeks showed complete resolution of the hema- toma without residual symptom (Figure 3). 3. DISCUSSION Spontaneous spinal subdural hematoma (SSDH) is a rare disease entity first described by Shiller and co- workers more than 60 years ago [1]. Several predis- posing factors are reported to have caused this, in- cluding impaired clotting due to therapeutic antico- agulation or hematologic disorder, vascular anomaly, intraspinal tumor, and iatrogenic causes such as lum- bar puncture or spinal anesthesia. However, the pathogenesis of spontaneous SSDHs is little under- stood. (a) (b) (c) (d) Figure 2. Spine MR shows spinal subdural hemorrhage anterior to the spinal cord from the C6 to L5 level with iso- and low signal intensity on T2-weighted image (a, c) and high and low- signal intensity on T1-weighted (b,d). Axial image scanned at T2 level reveals the lesion compressing the s p i nal c ord . 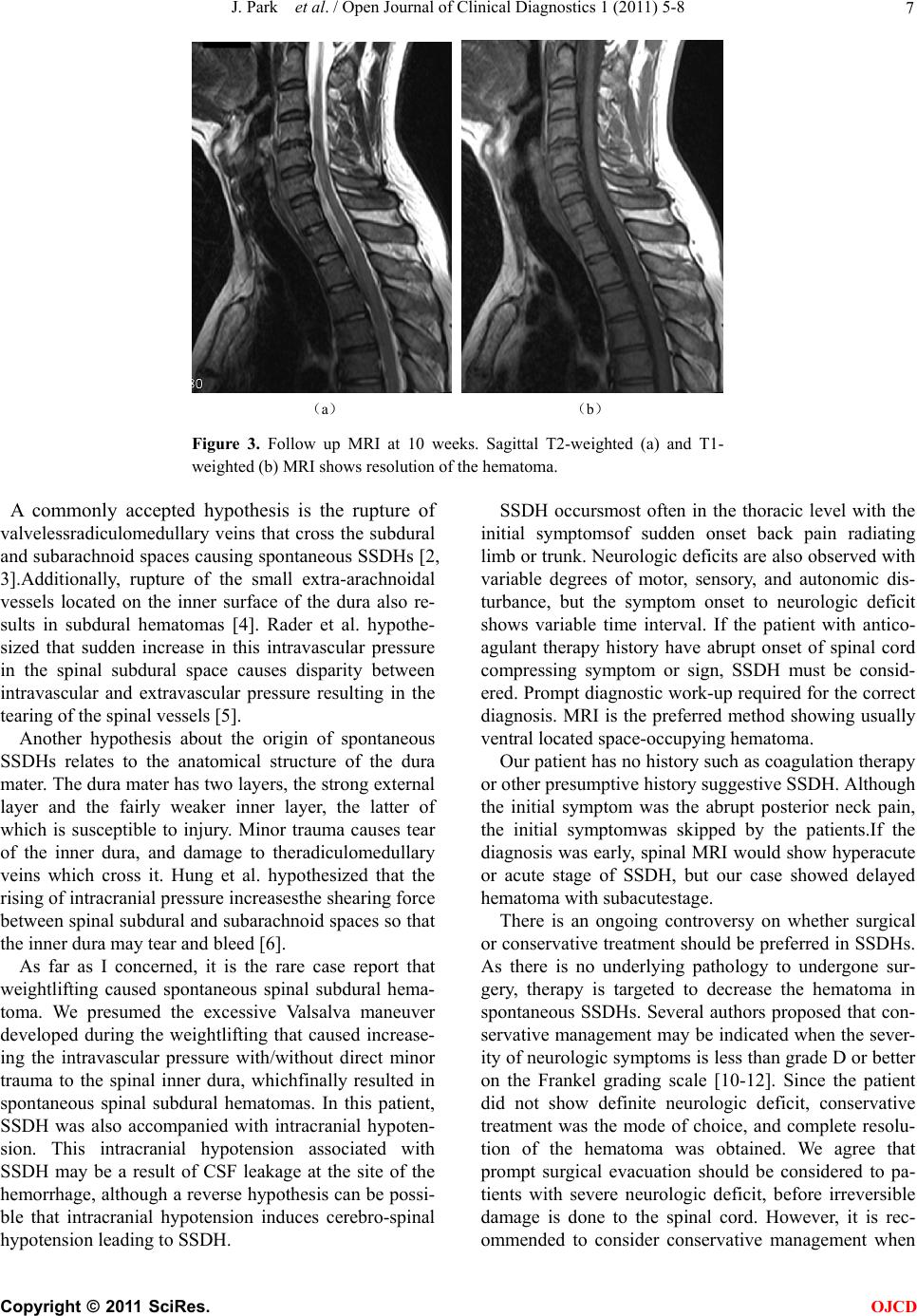 J. Park et al. / Open Journal of Clinical Diagnostics 1 (2011) 5-8 Copyright © 2011 SciRes. OJCD 7 (a) (b) Figure 3. Follow up MRI at 10 weeks. Sagittal T2-weighted (a) and T1- weighted (b) MRI shows resolution of the hematoma. A commonly accepted hypothesis is the rupture of valvelessradiculomedullary veins that cross the subdural and subarachnoid spaces causing spontaneous SSDHs [2, 3].Additionally, rupture of the small extra-arachnoidal vessels located on the inner surface of the dura also re- sults in subdural hematomas [4]. Rader et al. hypothe- sized that sudden increase in this intravascular pressure in the spinal subdural space causes disparity between intravascular and extravascular pressure resulting in the tearing of the spinal vessels [5]. Another hypothesis about the origin of spontaneous SSDHs relates to the anatomical structure of the dura mater. The dura mater has two layers, the strong external layer and the fairly weaker inner layer, the latter of which is susceptible to injury. Minor trauma causes tear of the inner dura, and damage to theradiculomedullary veins which cross it. Hung et al. hypothesized that the rising of intracranial pressure increasesthe shearing force between spinal subdural and subarachnoid spaces so that the inner dura may tear and bleed [6]. As far as I concerned, it is the rare case report that weightlifting caused spontaneous spinal subdural hema- toma. We presumed the excessive Valsalva maneuver developed during the weightlifting that caused increase- ing the intravascular pressure with/without direct minor trauma to the spinal inner dura, whichfinally resulted in spontaneous spinal subdural hematomas. In this patient, SSDH was also accompanied with intracranial hypoten- sion. This intracranial hypotension associated with SSDH may be a result of CSF leakage at the site of the hemorrhage, although a reverse hypothesis can be possi- ble that intracranial hypotension induces cerebro-spinal hypotension leading to SSDH. SSDH occursmost often in the thoracic level with the initial symptomsof sudden onset back pain radiating limb or trunk. Neurologic deficits are also observed with variable degrees of motor, sensory, and autonomic dis- turbance, but the symptom onset to neurologic deficit shows variable time interval. If the patient with antico- agulant therapy history have abrupt onset of spinal cord compressing symptom or sign, SSDH must be consid- ered. Prompt diagnostic work-up required for the correct diagnosis. MRI is the preferred method showing usually ventral located space-occupying hematoma. Our patient has no history such as coagulation therapy or other presumptive history suggestive SSDH. Although the initial symptom was the abrupt posterior neck pain, the initial symptomwas skipped by the patients.If the diagnosis was early, spinal MRI would show hyperacute or acute stage of SSDH, but our case showed delayed hematoma with subacutestage. There is an ongoing controversy on whether surgical or conservative treatment should be preferred in SSDHs. As there is no underlying pathology to undergone sur- gery, therapy is targeted to decrease the hematoma in spontaneous SSDHs. Several authors proposed that con- servative management may be indicated when the sever- ity of neurologic symptoms is less than grade D or better on the Frankel grading scale [10-12]. Since the patient did not show definite neurologic deficit, conservative treatment was the mode of choice, and complete resolu- tion of the hematoma was obtained. We agree that prompt surgical evacuation should be considered to pa- tients with severe neurologic deficit, before irreversible damage is done to the spinal cord. However, it is rec- ommended to consider conservative management when  J. Park et al. / Open Journal of Clinical Diagnostics 1 (2011) 5-8 Copyright © 2011 SciRes. OJCD 8 neurologic symptoms are mild or the symptoms improve quickly to the treatment of spinal edema. 4. CONCLUSIONS Several predisposing factors are reported to have caused this spontaneous spinal subdural hematoma (SSDH). The weightlifting practical exercise can be a one of cause of developing the spontaneous SSDH which can associate with intracranial hypotension. REFERENCES [1] Dickerman, R.D., McConathy, W.J., Smith, G.H., East, J.W. and Rudder, L. (2000) Middle cerebral artery blood flow velocity in elite power athletes during maximal weight-lifting. Resarch on Neurology, 22, 337-340. [2] Dickerman, R.D. and Morgan, J. (2005) Pathogenesis of subdural hematoma in healthy athletes: Postexertional intracranial hypotension? Acta Neurochirurgica (Wien), 147, 349-350. doi:10.1007/s00701-004-0476-0 [3] Hung, K.S., Lui, C.C., Wang, C.H., Wang, C.J. and Howng, S.L. (2002) Traumatic spinal subdural hematoma with spontaneous resolution. Spine (PhilaPa 1976), 27, E534-E538. [4] Kakitsubata, Y., Theodorou, S.J., Theodorou, D.J., Mi- yata, Y., Ito, Y., Yuki, Y., Honbu, K. and Maehara, T. (2010) Spontaneous spinal subarachnoid hemorrhage as- sociated with subdural hematoma at different spinal lev- els. Emergency Radiology , 17, 69-72. doi:10.1007/s10140-008-0792-4 [5] Kirsch, E.C., Khangure, M.S., Holthouse, D. and McAuliffe, W. (2000) Acute spontaneous spinal subdural haematoma: MRI features. Neuroradiology, 42, 586-590. doi:10.1007/s002340000331 [6] Kyriakides, A.E., Lalam, R.K. and El Masry, W.S. (2007) Acute spontaneous spinal subdural hematoma presenting as paraplegia: A rare case. Spine (PhilaPa 1976), 32, E619-E622. [7] Maeda, M., Mochida, J., Toh, E., Nishimura and K., Nomura, T. (2001) Nonsurgical treatment of an upper thoracic spinal subdural hemorrhage. Spinal Cord, 39, 657-661. doi:10.1038/sj.sc.3101219 [8] Ozdemir, O., Calisaneller, T., Yildirim, E., Caner, H. and Altinors, N. (2008) Acute spontaneous spinal subdural hematoma in a patient with bilateral incarcerated inguinal hernia. Joint Bone Spine, 75, 345-347. doi:10.1016/j.jbspin.2007.05.019 [9] Payer, M. and Agosti, R. (2010) Spontaneous acute spi- nal subdural hematoma: spontaneous recovery from se- vere paraparesis-case report and review. Acta Neurochi- rurgica (Wien), 152, 1981-1984. doi:10.1007/s00701-010-0758-7 [10] RADER, J.P. (1955) Chronic subdural hematoma of the spinal cord: Report of a case. The New England Journal of Medici ne, 253, 374-376. doi:10.1007/s00701-010-0758-7 [11] Schiller, F., Neligan, G. and Budtz-Olsen, O. (1948) Sur- gery in haemophilia; a case of spinal subdural haema- toma producing paraplegia. Lancet, 2, 842-845. doi:10.1016/S0140-6736(48)91427-5 [12] Zeidan, A., Farhat, O., Maaliki H and Baraka A. (2010) Does postdural puncture headache left untreated lead to subdural hematoma? Case report and review of the lit- erature. Middle East Journal of Anesthesiology, 20, 483-492. |