J. CONTESSA ET AL.
399
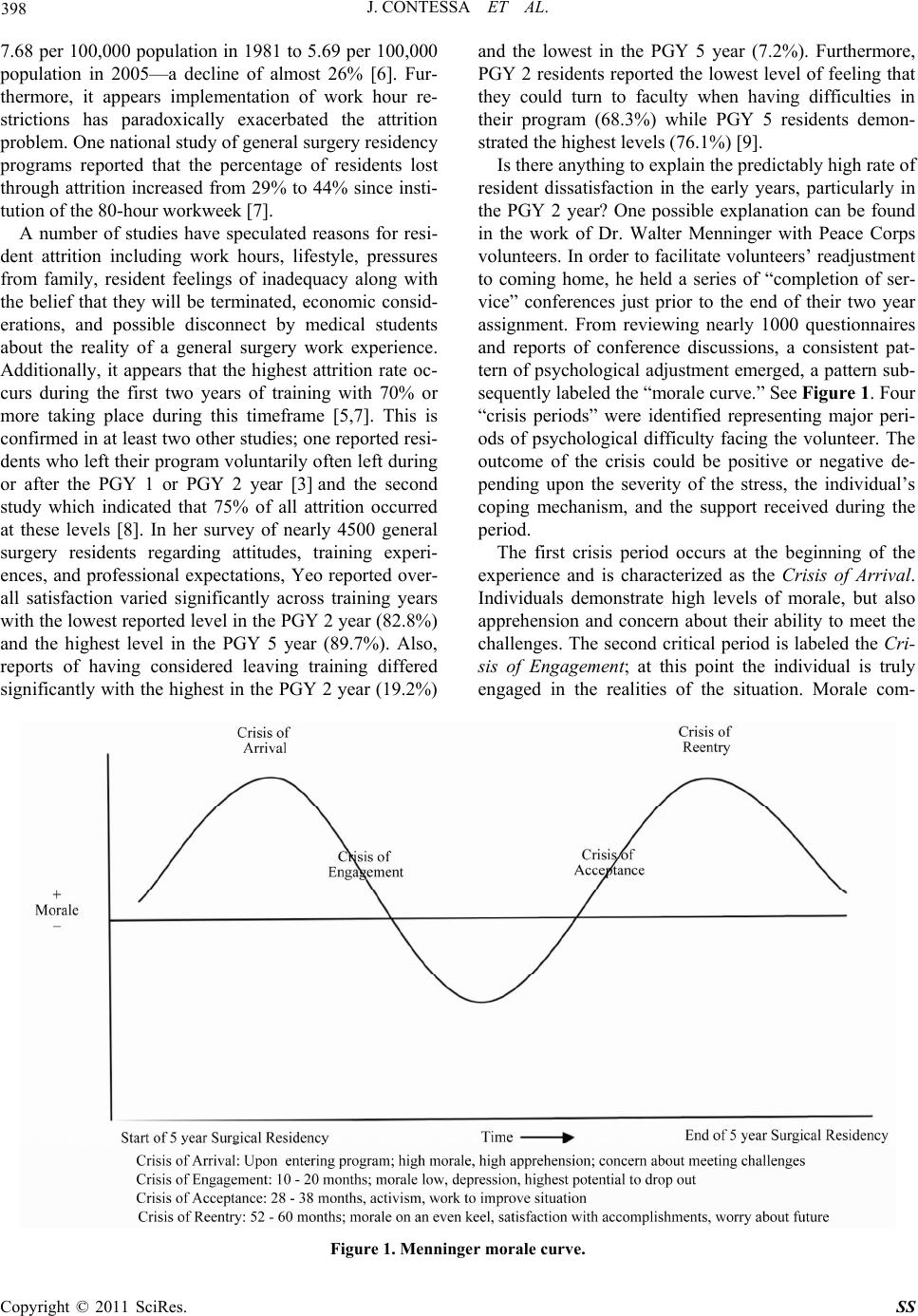
monly is low at this point due to frustrations and limited
support in the new situation. The central feature of this
stage is marked by depression. Individuals take stock of
what they left behind, of unrealized expectations of ac-
complishment, of freedom to express their frustrations.
In the Peace Corps study dropouts peaked during this
stage. The third phase wa s noted approximately half-w ay
through the experience and identified as the Crisis of
Acceptance. This stage is described as one where morale
has been restored as a result of increased knowledge and
mastery of the situation. However, emotionally the tone
is frequently one of anger and activism. Individuals
spoke out more freely and pursued changes to improve
the situation. The final crisis is labeled the Crisis of Re-
entry; morale was generally on an even keel, some satis-
faction associated with what they accomplished and with
completing their commitment, but so me depression asso-
ciated with giving up their identity and ending relation-
ships, and apprehension about an uncertain future.
Menninger indicated that the morale curve is not
unique to the Peace Corps experience, but represents a
process that all individuals undergo as they enter new life
situations. Morale follows a predictable cycle; how an
individual responds is determined by one’s position
within that cycle. He provides support that shows the
model is both universal and scalable (e.g., Stafford-
Clark’s description of the changes in the morale of flight
crew during their 30-sortie tours in World War II) [10].
To date, there has been no research investigating level
of morale of general surgery residents. This study sought
to assess level of resident morale in a general surgery
residency program at the four crisis points to determine if
a cycle similar to the Menninger morale curve is dis-
played and what the implications might be for resident
attrition.
2. Design, Methodology, and
Instrumentation
The instrument used to measure resident morale was the
Morale Assessment in General Practice Index (MAGPI).
This is a 14 question self-scoring instrument designed to
help physicians think about the sources of stress in their
lives and to give them an idea of how they compare with
their colleagues. Respondents are asked to select one of
three statements that “best reflect how you feel about
yourself.” The instrument is scored on the basis of three
points for the most stressed answer, two for intermediate,
and one for least.
MAGPI developers compared their instrument to the
General Health Questionnaire 28 (GHQ 28), which is a
well-validated measure of distress. Both instruments
were sent to 875 physicians in southeast Scotland. Total
scores for the MAGPI were well correlated with total
GHQ 28 scores (r2 = 0.68 p < 0.001). In addition, high
and intermediate scores in all MAGPI parameters (with
one exception) were significantly correlated with GHQ
28 “caseness”—a term used to describe those at risk of
psychological stress. Performing a principal component
analysis revealed four factors comprising the MAGPI:
factor 1—components of control, health, happiness, and
support from friends and worries about family; factor
2—components of being up-to-date, perceptions of value
of patients and colleagues, and career satisfaction; factor
3—components of getting along with colleagues; factor
4—concern over alcohol use. When these factors were
correlated with GHQ 28, all four factors were correlated
highly or moderately, but all demonstrated a p value of
<0.01. In summary, the MAGPI seems to stand up par-
ticularly well when validated against GHQ 28. Also, the
MAGPI was given to 50 General Practitioner trainers.
They found it easy to complete and score, felt the ques-
tions were relevant, and believed that no important pa-
rameters had been missed indicating the MAGPI also has
strong face validity and high acceptability [11].
In this study, the MAGPI was administered to a total
of 21 residents in their PGY 1, 2, 3, and 5 years. Resi-
dents completed th e instru ment in a timeframe during th e
5 year residency cycle congruent with the four crises
identified in the Menninger morale curve—PGY 1 resi-
dents in August, PGY 2 residents in October, PGY 3
residents in March and PGY 5 residents in May.
Setting
The Hospital of Saint Raphael, General Surgery Resi-
dency Program, New Haven, Connecticut. Testing dates
were announced approximately one week prior and resi-
dents reported to a conference room to complete the in-
strument.
Participants
Surgical residents of the Hospital of Saint Raphael
General Surgery Residency Program at the PGY 1, 2, 3,
and 5 levels.
3. Results and Statistical Procedures
Non-parametric methods (Kruskal-Wallis comparisons)
were carried out to assess if there were differences in
MAGPI responses among the four PGY groups. Even
though difference in the MAGPI total means scores did
not achieve statistical significance (p = 0.3229), the
scores for PGY 1 (16.7) and PGY 5 (17.8) residents were
trending lower than PGY 2 (18.0) and PGY 3 (19.5)
scores, indicating an overall higher level of morale for
the PGY 1 and PGY 5 groups (See Table 1). These
findings describe a curve that is similar in shape to the
Copyright © 2011 SciRes. SS