W. THANAPONGSATHORN
391
3) Two or three 5 mm port into single incision. One
port for 5mm telescope, others port for 5 mm hand in-
struments. (SI-MPA: Single Incision-Multiple Ports Ac-
cess).
All three approaches are single incision that will give
better cosmetic results than multiple incision procedure.
However, specialized trocars are very expensive, require
more special hand instruments and demand higher skills
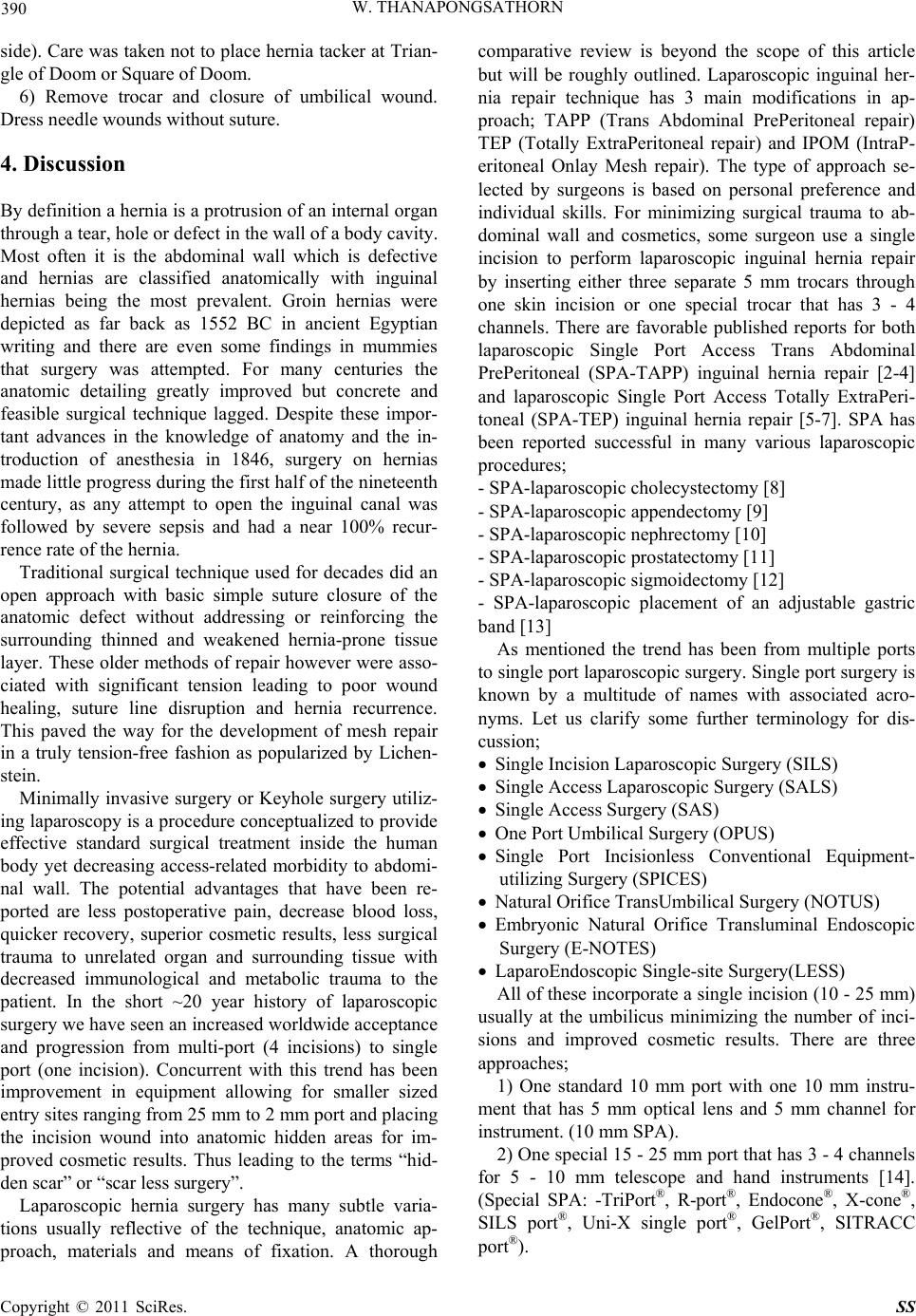
and trainings to perform the operation. Our technique of
10 mm SPA-IPOM using a standard trocar and gyneco-
logical instruments which are present in most operating
rooms can be performed by those surgeons who possess
standard laparoscopic surgical skills.
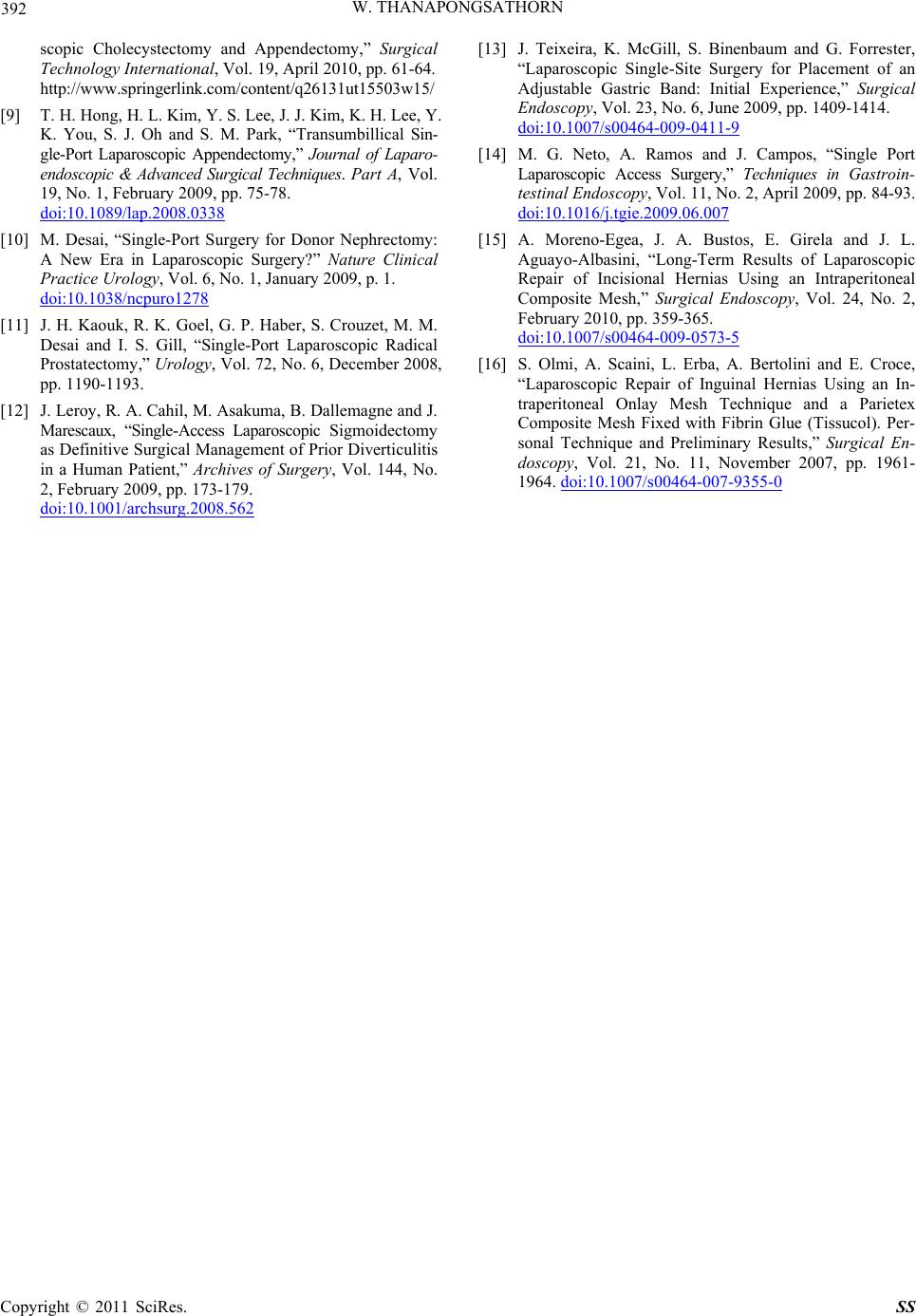
There are many reports using bioresorbable composite
mesh for standard incisional hernia repair [15]. Pa-
rietex™ Composite Mesh was introduced in 1999 with a
resorbable collagen barrier on one side to limit visceral
adhesion and a three-dimensional polyester knit structure
on the other to promote tissue in growth.
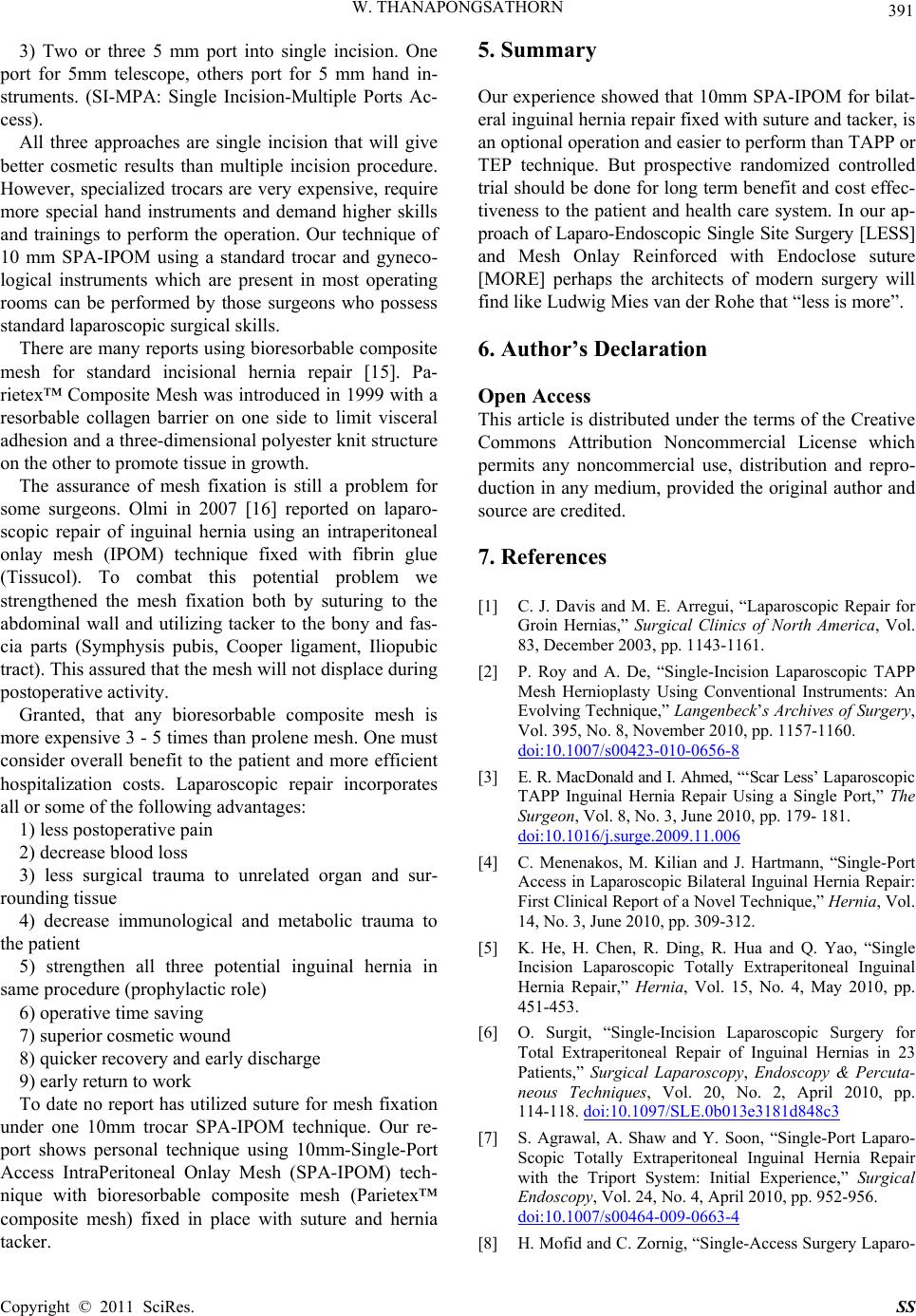
The assurance of mesh fixation is still a problem for
some surgeons. Olmi in 2007 [16] reported on laparo-
scopic repair of inguinal hernia using an intraperitoneal
onlay mesh (IPOM) technique fixed with fibrin glue
(Tissucol). To combat this potential problem we
strengthened the mesh fixation both by suturing to the
abdominal wall and utilizing tacker to the bony and fas-
cia parts (Symphysis pubis, Cooper ligament, Iliopubic
tract). This assured that the mesh will not displace during
postoperative activity.
Granted, that any bioresorbable composite mesh is
more expensive 3 - 5 times than prolene mesh. One must
consider overall benefit to the patient and more efficient
hospitalization costs. Laparoscopic repair incorporates
all or some of the following advantages:
1) less postope rat i ve pai n
2) decrease blood loss
3) less surgical trauma to unrelated organ and sur-
rounding tissue
4) decrease immunological and metabolic trauma to
the patient
5) strengthen all three potential inguinal hernia in
same procedure (prophylactic ro le)
6) operative time saving
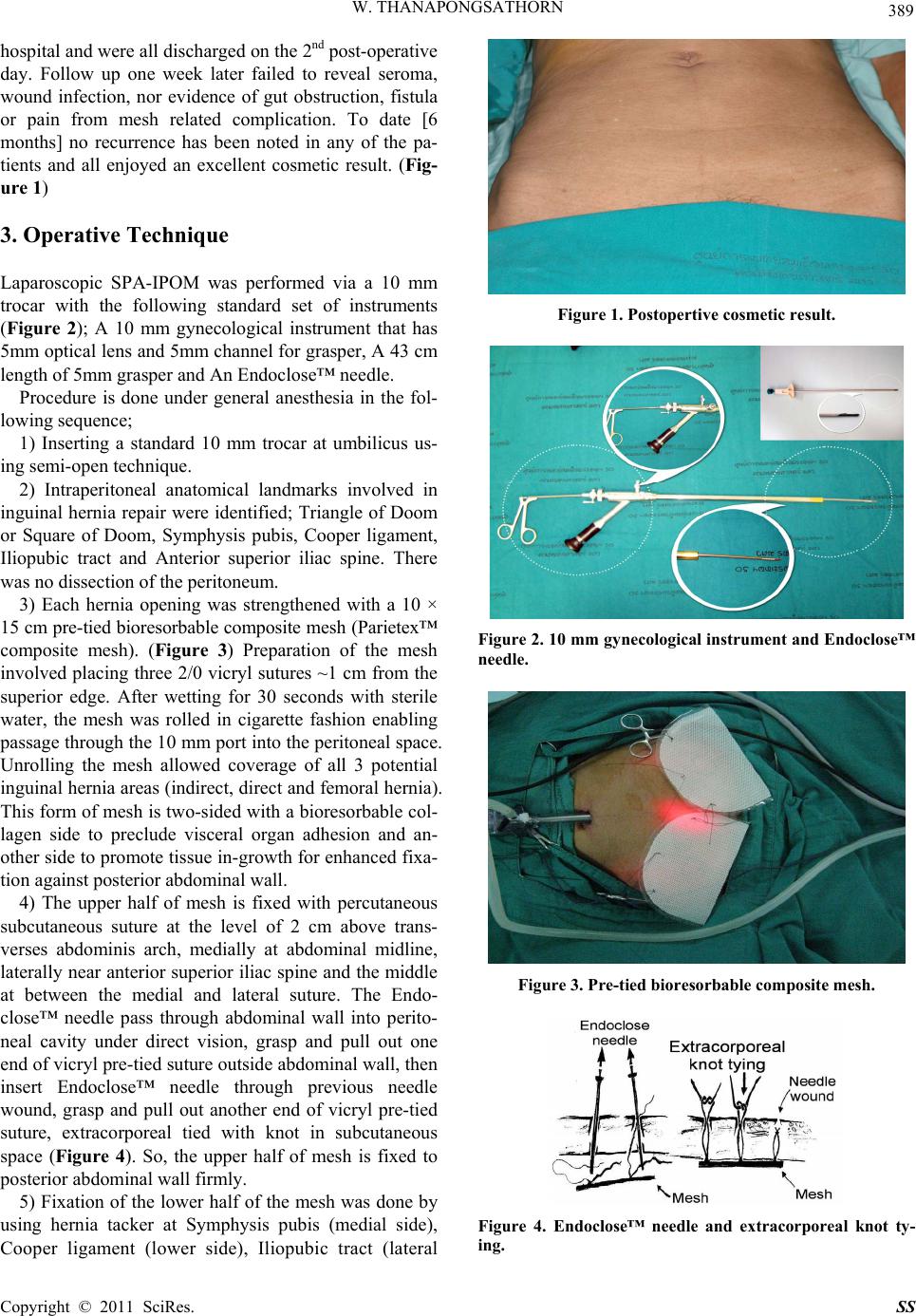
7) superior cosmetic wound
8) quicker recovery and early discharge
9) early return to work
To date no report has utilized suture for mesh fixation
under one 10mm trocar SPA-IPOM technique. Our re-
port shows personal technique using 10mm-Single-Port
Access IntraPeritoneal Onlay Mesh (SPA-IPOM) tech-
nique with bioresorbable composite mesh (Parietex™
composite mesh) fixed in place with suture and hernia
tacker.
5. Summary
Our experience showed that 10mm SPA-IPOM for bilat-
eral inguinal hernia repair fixed with su ture and tacker, is
an optional operation and easier to perform than TAPP or
TEP technique. But prospective randomized controlled
trial should be done for long term benefit and cost effec-
tiveness to the patient and health care system. In our ap-
proach of Laparo-Endoscopic Single Site Surgery [LESS]
and Mesh Onlay Reinforced with Endoclose suture
[MORE] perhaps the architects of modern surgery will
find like Ludwig Mies van der Rohe that “less is more”.
6. Author’s Declaration
Open Access
This article is distributed under the terms of the Creative
Commons Attribution Noncommercial License which
permits any noncommercial use, distribution and repro-
duction in any medium, provided the original author and
source are credited.
7. References
[1] C. J. Davis and M. E. Arregui, “Laparoscopic Repair for
Groin Hernias,” Surgical Clinics of North America, Vol.
83, December 2003, pp. 1143-1161.
[2] P. Roy and A. De, “Single-Incision Laparoscopic TAPP
Mesh Hernioplasty Using Conventional Instruments: An
Evolving Technique,” Langenbeck’s Archives of Surgery,
Vol. 395, No. 8, November 2010, pp. 1157-1160.
doi:10.1007/s00423-010-0656-8
[3] E. R. MacDonald and I. Ahmed, “‘Scar Less’ Laparoscopic
TAPP Inguinal Hernia Repair Using a Single Port,” The
Surgeon, Vol. 8, No. 3, June 2010, pp. 179- 181.
doi:10.1016/j.surge.2009.11.006
[4] C. Menenakos, M. Kilian and J. Hartmann, “Single-Port
Access in Laparoscopic Bilateral Inguinal Hernia Repair:
First Clinical Report of a Novel Technique,” Hernia, Vol.
14, No. 3, June 2010, pp. 309-312.
[5] K. He, H. Chen, R. Ding, R. Hua and Q. Yao, “Single
Incision Laparoscopic Totally Extraperitoneal Inguinal
Hernia Repair,” Hernia, Vol. 15, No. 4, May 2010, pp.
451-453.
[6] O. Surgit, “Single-Incision Laparoscopic Surgery for
Total Extraperitoneal Repair of Inguinal Hernias in 23
Patients,” Surgical Laparoscopy, Endoscopy & Percuta-
neous Techniques, Vol. 20, No. 2, April 2010, pp.
114-118. doi:10.1097/SLE.0b013e3181d848c3
[7] S. Agrawal, A. Shaw and Y. Soon, “Single-Port Laparo-
Scopic Totally Extraperitoneal Inguinal Hernia Repair
with the Triport System: Initial Experience,” Surgical
Endoscopy, Vol. 24, No. 4, April 2010, pp. 952-956.
doi:10.1007/s00464-009-0663-4
[8] H. Mofid and C . Zornig, “Single-Access Surgery Laparo-
Copyright © 2011 SciRes. SS