386 C. BODE ET AL.
to chance and unless otherwise stated, P < 0.05 was con-
sidered statistically significant.
3. Results
25 babies with EA/TEF were seen within the study pe-
riod. There were 14 (56%) males and 11 (44%) females,
giving a male:female ratio of 1.2:1. Their ages ranged
from 10 hours to 25 days with a mean age of 8.8 ± 5.2
days at presentation. The babies were all full-term, with a
mean birth weight of 2.6 ± 0.4 kg (range 2.1 - 3.7 kg).
Seventeen (68 % ) of these babies were first borns.
Maternal age ranged from 20 - 31 years, with a mean
of 24.5 ± 3.3 years. All the 25 mothers were Nigerian.
There was no preponderance of any ethnic group or oc-
cupation among the mothers. None of the mothers gave
any history of exposure to heavy metals or known tera-
togens. None of the babies was prenatally diagnosed as
having EA/TEF. Twenty four mothers (96%) lived in
low socio-economic parts of Lagos.
3.1. Monthly Frequency of EA/TEF Occurence
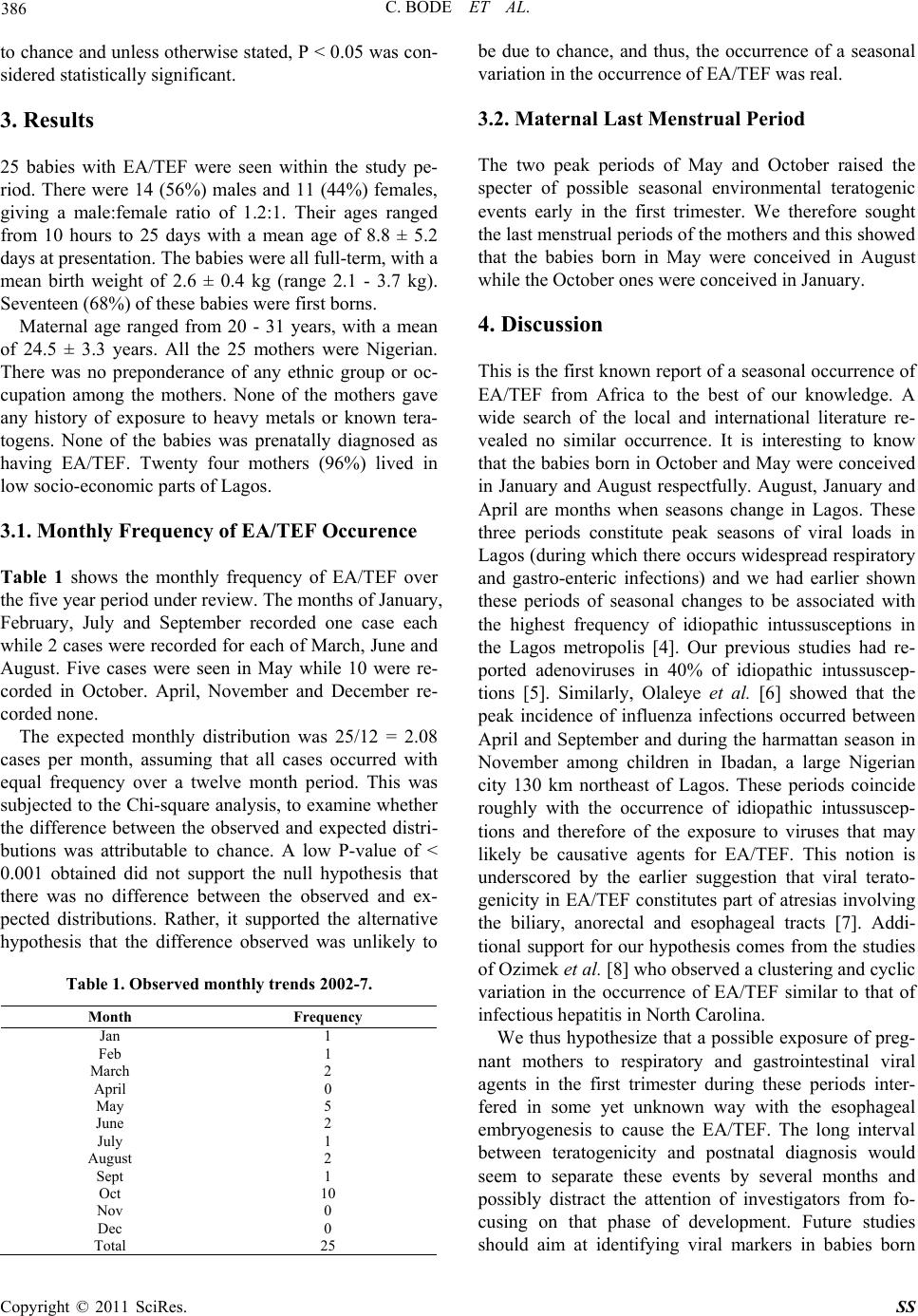
Table 1 shows the monthly frequency of EA/TEF over
the five year period under re view. Th e month s of Januar y,
February, July and September recorded one case each
while 2 cases were recorded for each of March, June and
August. Five cases were seen in May while 10 were re-
corded in October. April, November and December re-
corded none.
The expected monthly distribution was 25/12 = 2.08
cases per month, assuming that all cases occurred with
equal frequency over a twelve month period. This was
subjected to the Ch i-square analysis, to examine whether
the difference between the observed and expected distri-
butions was attributable to chance. A low P-value of <
0.001 obtained did not support the null hypothesis that
there was no difference between the observed and ex-
pected distributions. Rather, it supported the alternative
hypothesis that the difference observed was unlikely to
Table 1. Observed monthly trends 2002-7.
be due to chance, and thus, the occurrence of a seasonal
variation in the occurrence of EA/TEF was real.
3.2. Maternal Last Menst rual Period
The two peak periods of May and October raised the
specter of possible seasonal environmental teratogenic
events early in the first trimester. We therefore sought
the last menstrual periods of the mothers and this showed
that the babies born in May were conceived in August
while the October ones were conceived in January.
4. Discussion
This is the first known report of a seasonal occurrence of
EA/TEF from Africa to the best of our knowledge. A
wide search of the local and international literature re-
vealed no similar occurrence. It is interesting to know
that the babies born in October and May were conceived
in January and August respectfully. August, January and
April are months when seasons change in Lagos. These
three periods constitute peak seasons of viral loads in
Lagos (during which there occurs widespread respiratory
and gastro-enteric infections) and we had earlier shown
these periods of seasonal changes to be associated with
the highest frequency of idiopathic intussusceptions in
the Lagos metropolis [4]. Our previous studies had re-
ported adenoviruses in 40% of idiopathic intussuscep-
tions [5]. Similarly, Olaleye et al. [6] showed that the
peak incidence of influenza infections occurred between
April and September and during the harmattan season in
November among children in Ibadan, a large Nigerian
city 130 km northeast of Lagos. These periods coincide
roughly with the occurrence of idiopathic intussuscep-
tions and therefore of the exposure to viruses that may
likely be causative agents for EA/TEF. This notion is
underscored by the earlier suggestion that viral terato-
genicity in EA/TEF constitutes part of atresias involving
the biliary, anorectal and esophageal tracts [7]. Addi-
tional support for our hypothesis comes from the studies
of Ozimek et al. [8] who observed a clustering and cyclic
variation in the occurrence of EA/TEF similar to that of
infectious hepatitis in North Carolina.
We thus hypothesize that a possible exposure of preg-
nant mothers to respiratory and gastrointestinal viral
agents in the first trimester during these periods inter-
fered in some yet unknown way with the esophageal
embryogenesis to cause the EA/TEF. The long interval
between teratogenicity and postnatal diagnosis would
seem to separate these events by several months and
possibly distract the attention of investigators from fo-
cusing on that phase of development. Future studies
should aim at identifying viral markers in babies born
Month Frequency
Jan 1
Feb 1
March 2
April 0
May 5
June 2
July 1
August 2
Sept 1
Oct 10
Nov 0
Dec 0
Total 25
Copyright © 2011 SciRes. SS