G. AL-SAIED ET AL.
383
with the remainder either in the head and neck or the
trunk. There is seldom discolouration of the lesions in
the limb in contrast to those in the head and neck [6].
Infantile hemangiopericytoma tends to be located more
superficially than that in adults [9].
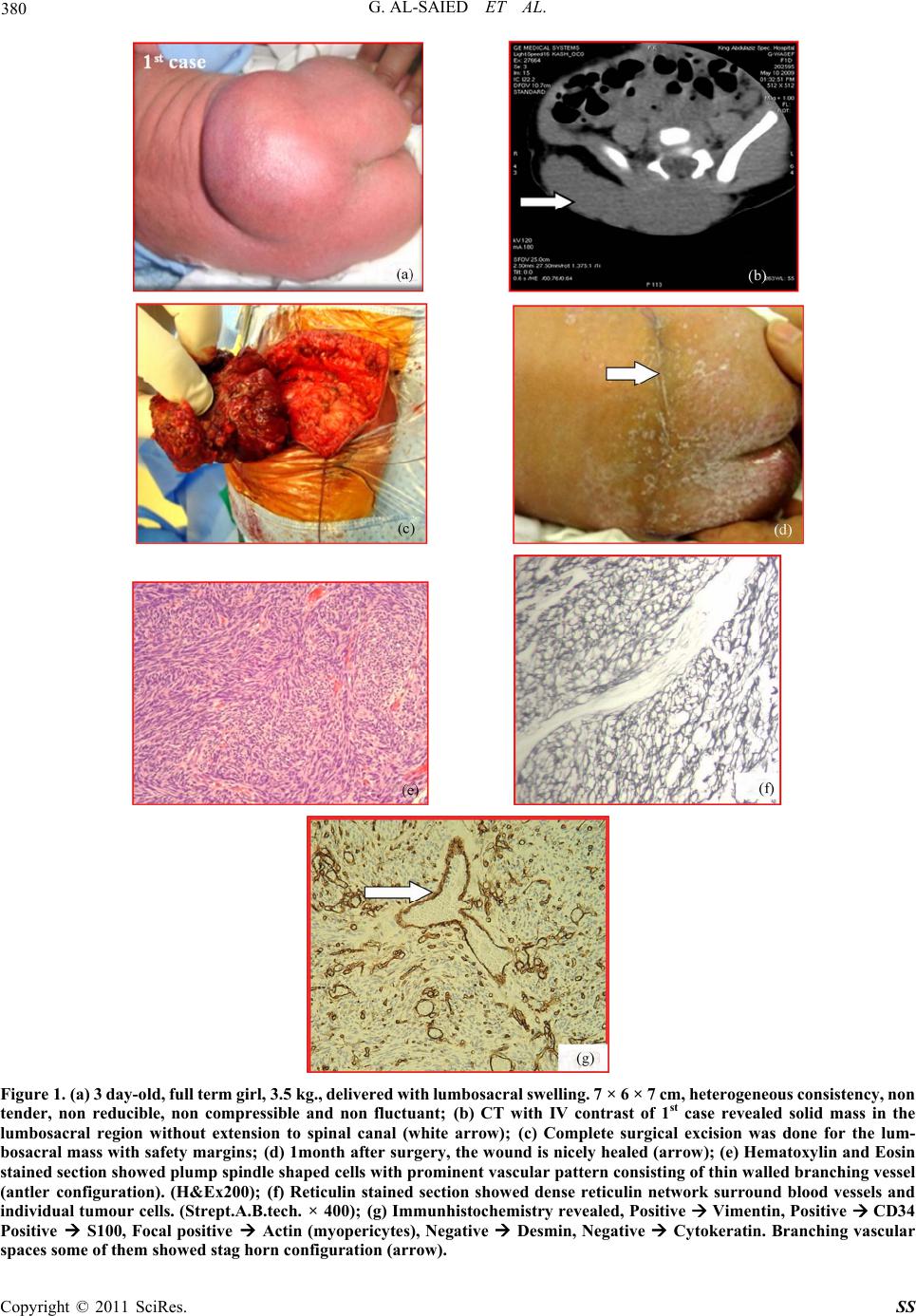
In our two cases, both masses were lying subcutane-
ously, in lumbosacral region without skin discoloration
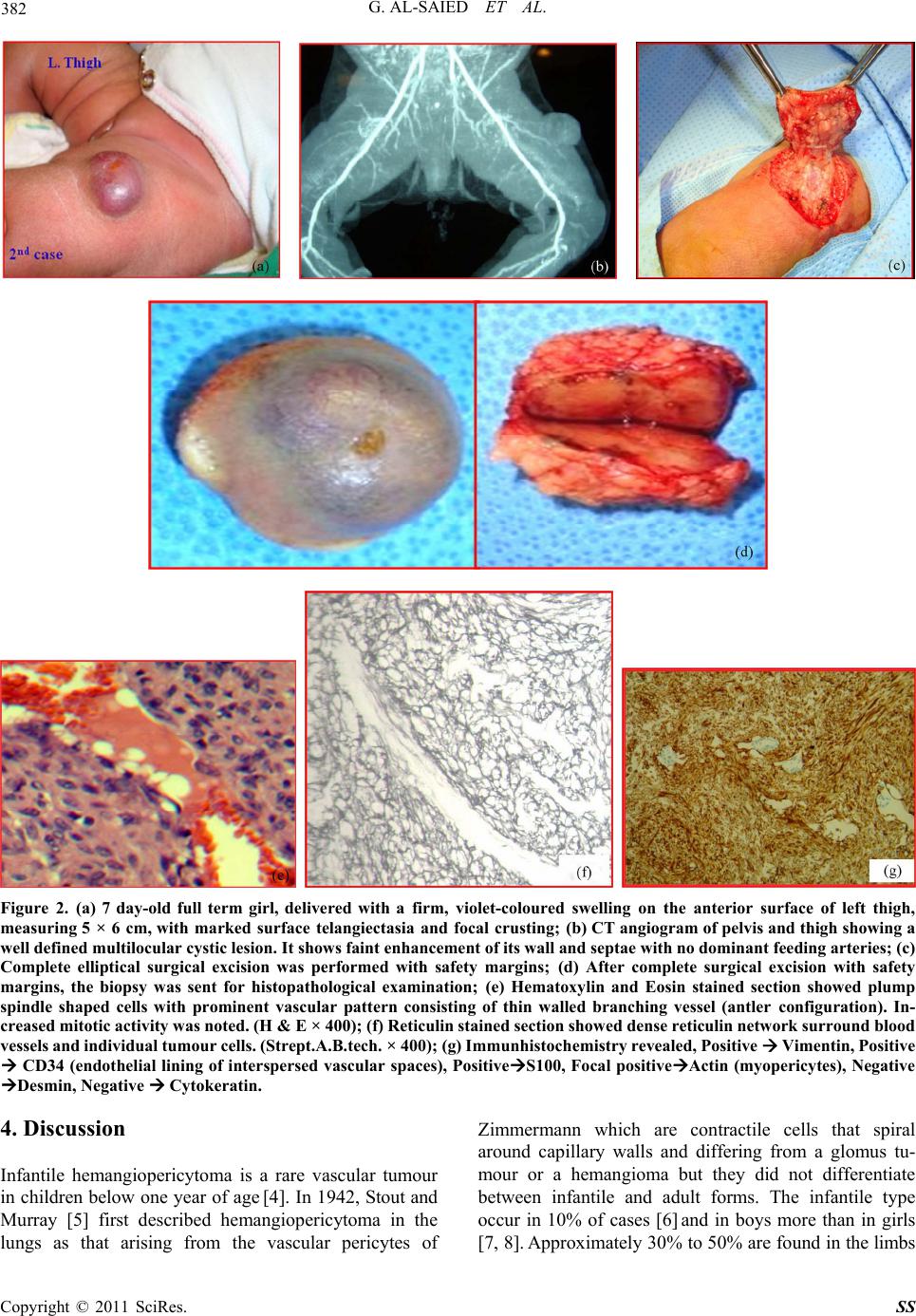
in 1st cases. Whereas, the 2nd mass was violet-coloured
on the anterior surface of left thigh.
The diagnosis can be aided by plain radiography
which shows a soft-tissue mass, with or without calcific
stippling. Ultrasound determines the size of the lesion,
vascular loops, the echogenic content and whether or not
a capsule is present, and angiography shows the vascular
pattern and the presence of feeder vessels. CT and MRI
can provide information about the extent of the tumour
and help in preoperative planning [9].
MRI and CT scan of lumbo-sacral canal (pre-and post
IV contrast ) of 1st case incorrectly interpreted the lesion as
teratoma versus myelomeningocele.
CT angiogram of pelvis and thigh of 2nd case, initially
diagnosed the lesion as a hemangiomatous malformation.
The diagnosis is confirmed by excisional biopsy [9].
The gross appearance of this lesion is usually transparent
or white-grey [6]. Feeder vessels may be prominent, and
the infantile form tends to be more multilobular than in
the adult. Microscopically; the pericyte may be round or
oval in shape. The tumour tends to be densely cellular,
with prominent vascular channels. Mitotic figures are
usually easily identified. The tumour cells stain posi-
tively with vimentin [6,9].
In our two cases the final diagnosis was achieved by
excisional biopsy. The histological and Immunhistochem-
istry features were consisting with infantile heman-
giopericytoma. In accordance with Enzinger and Smith's
criteria [3], both lesions were histologically benign.
There was no evidence of malignancy at the time of ex-
amination.
The differential diagnosis of congenital hemangio-
pericytoma includes all tumours which present as a soft
tissue mass, including lipoma, hemangioma, and lym-
phangioma. Some tumours have similar histological fea-
tures, such as infantile myofibromatosis, synovial sar-
coma, fibrosarcoma, malignant fibrous histiocytoma,
mesenchymal chondro sarcoma, and leiomyosarcoma [10-
13]. It is therefore impo rtan t to examine multip le areas of
the specimen to confirm the diagnosis [9].
The management of infantile hemangiopericytoma
differs from that in adults, but there is no consensus as to
the best method [9]. Wide surgical excision with safety
margin is the most accepted method of treatment
[6,14,15]. That is was our preferred method in manage-
ment of both cases. Some centres use adjuvant therapy to
reduce the risk of local recurrence [6-20] but the value is
difficult to assess because of the rarity of these tumours.
Chemotherapeutic regimens have included the use of
vincristine, doxorubicin, actinomycin and cyclophos-
phamide. Jha et al. [21] reported success with radiother-
apy when there was gross or microscopic evidence of
tumour remaining after excision, and adjuvant radio-
therapy was used with success by Borg and Benjamin
[22]. Other authors have reported that radiotherapy is
ineffective [14,15,23]. Metastatic disease has only been
reported in three cases of congenital hemangiopericy-
toma [4,15,24] although the adult form of the tumour has
a rate of distant metastasis of up to 56%, mainly to the
lung and skeleton [8,25]. Careful follow up is therefore
required. When recurrence does occur, adjunctive che-
motherapy has been used successfully [15].
Fortunately, there is no evidence of local recurrence or
distant metastasis during last 20 and 17 months in 1st
case and 2nd case respectively.
5. Conclusions
Most infantile hemangiopericytoma follow a benign
course. Rarely these tumours behave aggressively with
local infiltration, recurrences and even distant metastases.
Careful follow up is therefore essential.
6. References
[1] I. Hatzokos, I. Gigis, E. Iosifidou, A. Drakou and J.
Pournaras, “Primary Hemangiopericytoma of the Tibia.
Treatment by en Bloc Resection and Bone Transportation.
A Case Report,” Acta orthopaedica Belgica, Vol. 71,
2005, pp. 122-127.
[2] P. V. Bailey, T. R. Weber, T. F. Tracy, D. M. O’Connor
and C. Sotelo-Avila, “Congenital Hemangiopericytoma:
an Unusual Vascular Neoplasm of Infancy,” Bottom of
Form Surgery, Vol. 114, 1993, pp. 936-941.
[3] M. J. Hahn, R. Dawnson, J. A. Esterly and D. J. Joseph,
“Hemangiopericytoma. An Ultrastructural Study,” Can-
cer, Vol. 31, No1, 1973, pp. 255-261.
[4] S. L. Kauffman and A. P. Stout, “Hemangiopericytoma in
Children,” Cancer, Vol. 13, No. 4, 1960, pp. 695-710.
[5] A. P. Stout and M. R. Murray, “Hemangiopericytoma: A
Vascular Tumor Featuring Zimmermann’s Pericytes,”
Annals of Surgery, Vol. 116, No. 1, 1942, pp. 26-33.
doi:10.1097/00000658-194207000-00004
[6] S. A. Hoey, R. M. Letts and C. Jinemez, “Infantile He-
mangiopericytoma of the Musculoskeletal System: Case
Report and Literature Review,” Journal of Pediatric Or-
thopaedics, Vol. 18, No. 3, 998, pp. 359-362.
[7] D. L. Baker, D. Oda and R. W. Myall, “Intraoral Infantile
Hemangiopericytoma: Literature Review and Addition of
a Case,” Oral Surgery, Oral Medicine, Oral Pathology,
Oral Radiology and Endodontology, Vol. 73, No. 5, 1992,
pp. 596-602.
Copyright © 2011 SciRes. SS