Surgical Science, 2011, 2, 376-378
doi:10.4236/ss.2011.27082 Published Online September 2011 (http://www.SciRP.org/journal/ss)
Copyright © 2011 SciRes. SS
Eyelid Fissure Narrowing after Recession of the Medial
Rectus Muscle
Hirohiko Kakizaki1*, Yasuhiro Takahashi1, Akihiro Ichinose2, Masayoshi Iwaki1
1Department of Ophthalmolog y, Aichi Medical University, Nagakute, Aichi, Japan
2Department of Plastic Surgery, Kobe University, Chuo, Kobe, Japan
E-mail: *cosme@d1.dion.ne.jp
Received January 13, 2011; revised February 5, 2011; accepted March 12, 2011
Abstract
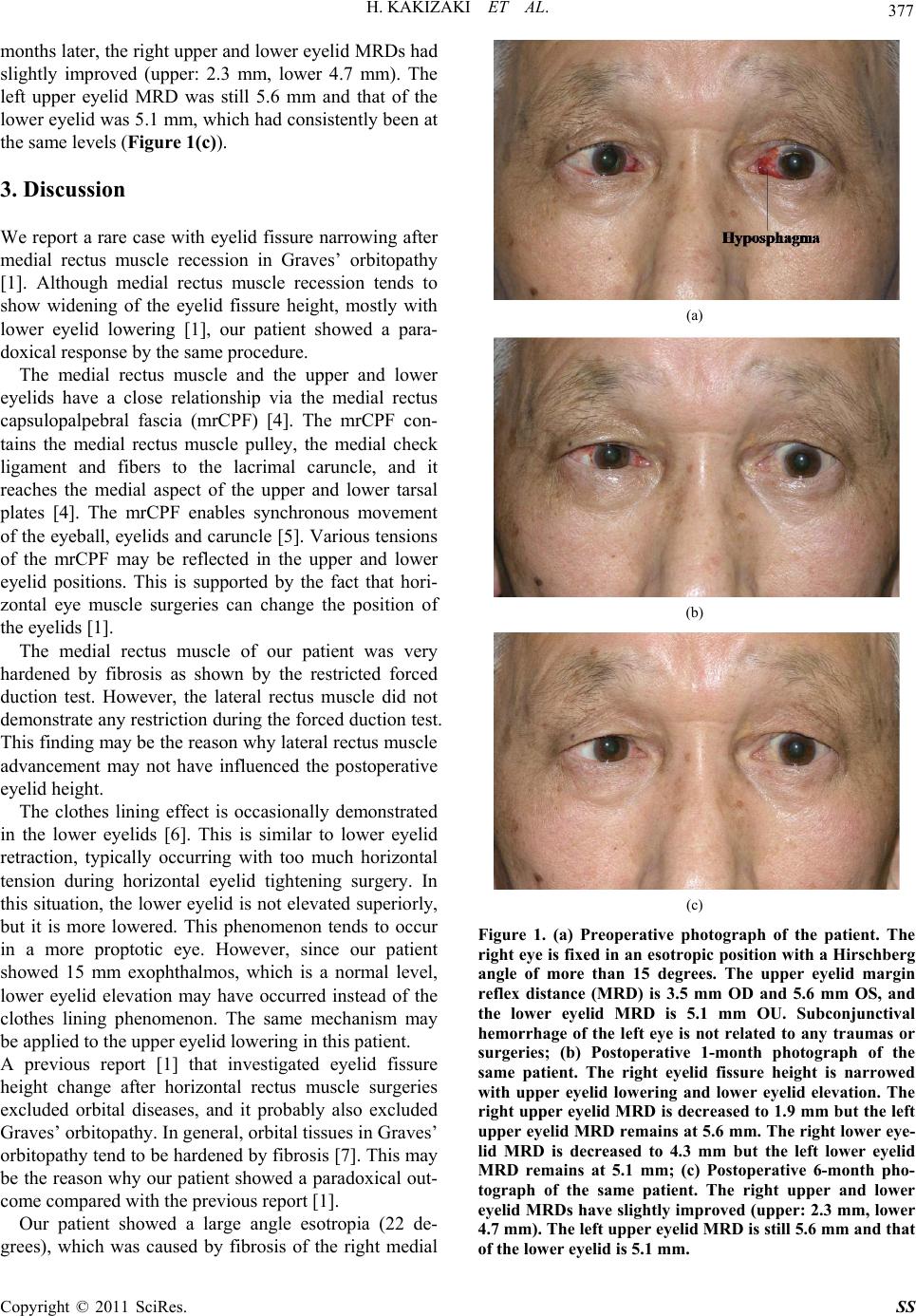
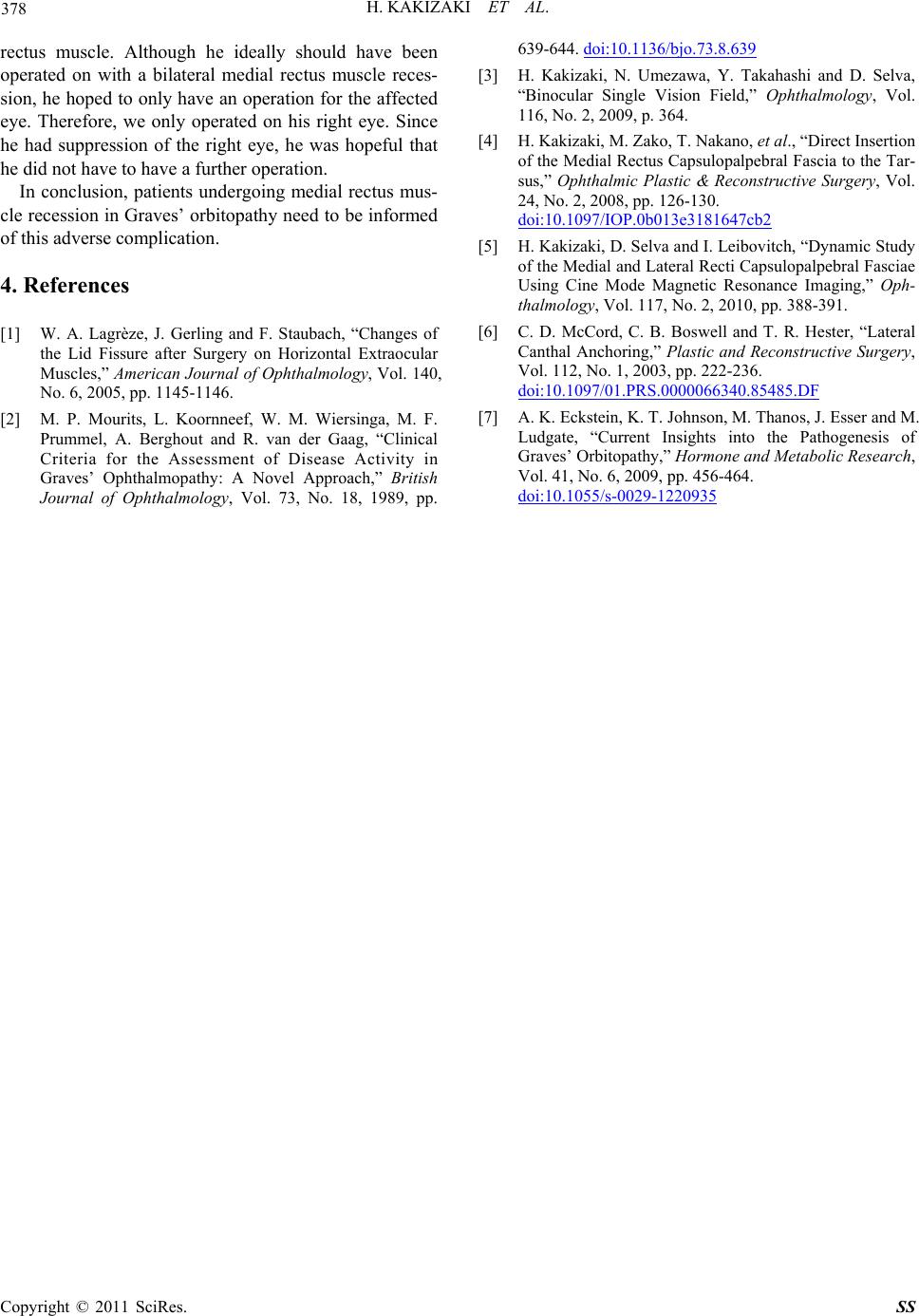
A 67-year-old male had suffered from eye movement disturbance from Graves’ orbitopathy. His right eye
was fixed in an esotropic position. Examination by synoptophore showed that his right eye deviation was 22
degrees medially. The upper eyelid margin reflex distance (MRD) was 3.5 mm OD and 5.6 mm OS, and the
lower eyelid MRD was 5.1 mm OU. Six mm medial rectus muscle recession with tenotomy was performed
in the patient. The next day after the surgery, his eye position did not change and the right eyelid fissure
demonstrated narrowing with upper eyelid lowering and lower eyelid elevation. The right upper eyelid MRD
was decreased to 1.9 mm and the right lower eyelid MRD was similarly decreased to 4.3 mm. On the same
day, 4 mm resection of the ipsilateral lateral rectus muscle was performed, but the same MRDs were ob-
served postoperatively. Patients undergoing medial rectus muscle recession in Graves’ orbitopathy need to
be informed of this potential complication.
Keywords: Graves’ Orbitopathy, Lower Eyelid Elevation, Margin Reflex Distance, Medial Rectus Muscle,
Upper Eyelid Lowering
1. Introduction
Surgery on the medial rectus muscle is known to have
the complication of a change in eyelid fissure heigh t [1].
Recession tends to show widening of the eyelid fissure
height, and then narrowing which is mostly caused by
resection [1]. Although these results are mainly due to
changes in the lower eyelid position, upper eyelid low-
ering by recession is a rare response [1].
We report a case with eyelid fissure height narrowing
with upper eyelid lowering and lower eyelid elevation
after medial rectus muscle recession in Graves’ orbito-
pathy.
2. Case Report
A 67-year-old male had suffered from eye movement
disturbance from Graves’ orbitopathy. At first admission,
his thyroid hormone level was normal and his clinical
activity score [2] was 0 points. He was administered two
times steroid pulse therapy more than 1 year prior to the
admission. His visual acuity was 0.6 OD and 0.9 OS, the
loss of which was caused by a cataract. Hertel exoph-
thalmometry showed 15 mm OU. His right eye was fixed
in an esotrop ic position with a Hirschberg angle of more
than 15 degrees (Figure 1(a)). A binocular single vision
field [3] showed no single vision area at the time, but he
suppressed his right eye under the unconscious. A forced
duction test demonstrated lateral restriction but it did not
show any medial resistance. According to a synopto-
phore, his right eye deviation was 22 degrees medially.
The upper eyelid margin reflex distance (MRD) was 3.5
mm OD and 5.6 mm OS, and the lower eyelid MRD was
5.1 mm OU (Figure 1(a)).
Six mm medial rectus muscle recession with tenotomy
was initially performed in the patient. The nex t day after
surgery, his eye position did not change, but the right
eyelid fissure height demonstrated narrowing with upper
eyelid lowering and lower eyelid elevation. The right
upper eyelid MRD was decreased to 1.9 mm, but the left
upper eyelid MRD remained at 5.6 mm. In addition, the
right lower eyelid MRD was decreased to 4.3 mm but the
left lower eyelid MRD remained at 5.1 mm. On the same
day, 4 mm advancement of the ipsilateral lateral rectus
muscle was performed, but unfortunately, the same
MRDs were observed postoperatively (Figure 1(b)). Six