Health Care Discrimination in HIV Care
102
ures compared to nurses except hand washing practices
where nurses are better [20,22]. There is no difference in
knowledge and discriminatory attitude with doctors/nur-
ses [8,21]. Some studies show incomplete knowledge
among nurses but even a perceived knowledge has weak
effect on compliance with UP and willingness to care
BBP infected [18,19]. High risk perception was noted
with doctors and poor knowledge of UP and Post Expo-
sure Prophylaxis (PEP) was noted with surgical trainee
[15,17].
Some studies notified least discriminatory behavior
with physician compared to nurses and the same is high
with servants [1,2], which may reflect knowledge and
educational influence on HCW towards attitude with
PLHAs. Provider not adopting UP and inadequate train-
ing are more likely to favor restrictive policies towards
PLHA [7]. Discriminatory attitud e and fear of infectivity
among HCWs decreases as contact with PLHAs/Homo-
sexuals increased [9]. Adequate UP training improves the
knowledge, adherence and supplies of UP in hospitals
[24].
Various studies done across the world so far have
proven that the mindset of HCWs regarding the immoral
behavior of PLHAs, the lacunae in adopting UP meas-
ures and lack of knowledge are mainly responsible for
the discriminatory behavior among HCWs towards PLHAs.
4. Conclusions
After the decades of HIV identification contact with
PLHAs over the time might made HCWs sensitized and
involved in caring PLHAs. Varying degr ee of knowledge
among professionals and countries should be tackled
with targeting multidisciplinary approach by providing
knowledge with training, workshop and creating profes-
sional/social models to interact.
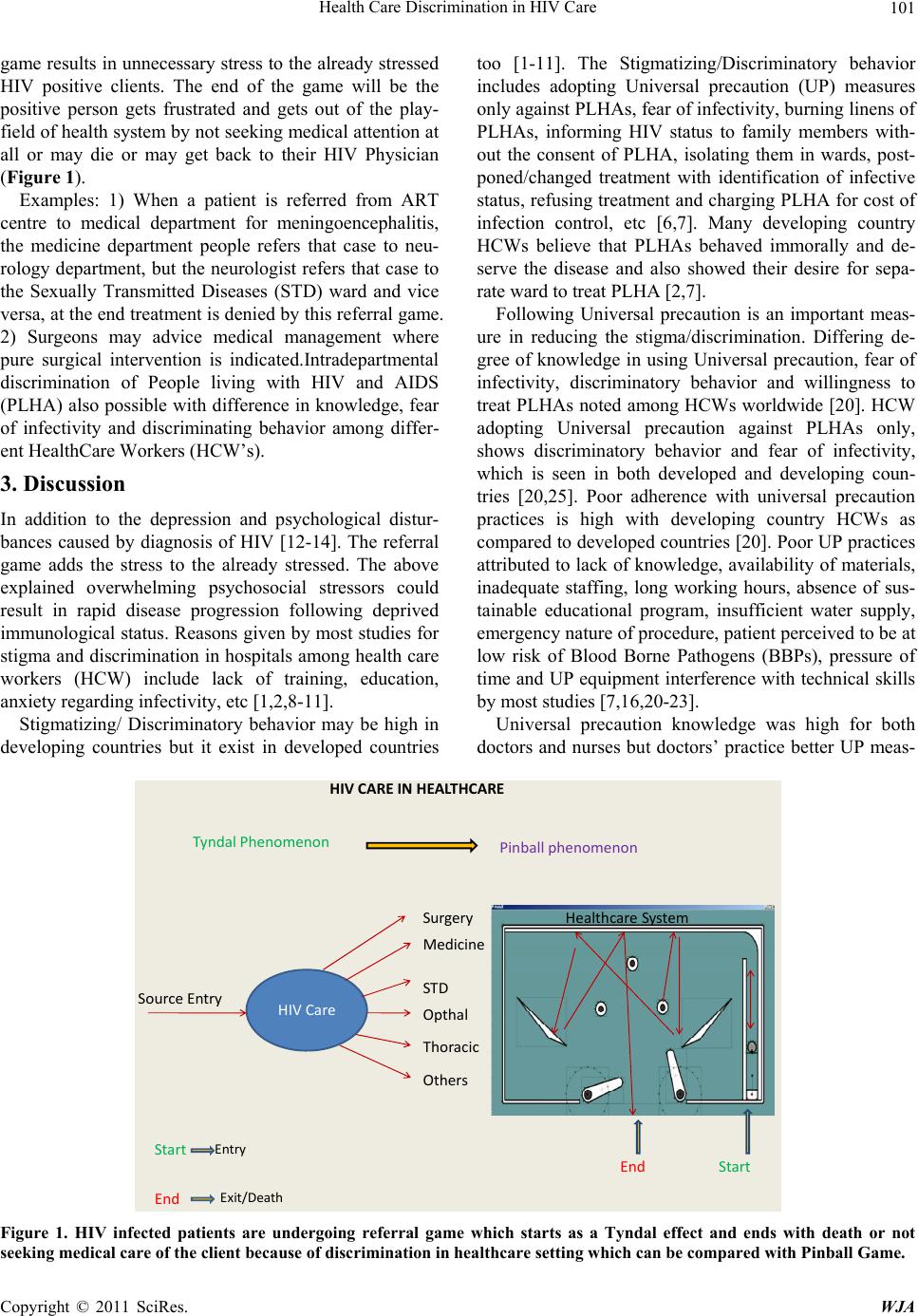
To improve the care of the HIV infected the referral
game should be demolished. So training for all healthcare
professionals is necessary regardless of their branch in
medicine. The hypothesized referral game should be ex-
plored by further studies to improve the care in HIV in-
fected clients.
REFERENCES
[1] V. S. Mahendra, L. Gilborn, S. Bharat, R. Mudoi, I.
Gupta, B. George, L. Samson, C. Daly and J. Pulerwitz,
“Understanding and Measuring AIDS-Related Stigma in
Health Care Settings: A Developing Country Perspec-
tive,” Journal of Social Aspects of HIV/AIDS, Vol. 4, No.
2, 2007, pp. 616-625.
[2] V. Menon and K. Bharucha, “Acquired Immunodefi-
ciency Syndrome and Health Care Professionals,” Jour-
nal of Association of Physicians of India, Vol. 42, No. 1,
1994, pp. 22-23.
[3] V. Chakrapani, P. A. Newman, M. Shunmugam, A. K.
Kurian and R. Dubrow, “Barriers to Free Antiretroviral
Treatment Access for Female Sex Workers in Chennai,
India, AIDS Patient Care and STDs, Vol. 23, No. 11,
2009, pp. 973-980. doi:10.1089/apc.2009.0035
[4] N. Kumarasamy, S. A. Sa fren, S. R. Ramina ni, R. Pickard,
R. James, A. K. Krishnan, S. Solomon and K. H. Mayer,
“Barriers and Facilitators to Antiretroviral Medication
Adherence among Patients with HIV in Chennai, India: A
Qualitative Study,” AIDS Patient Care and STDs, Vol. 19,
No. 8, 2005, pp. 526-537. doi:10.1089/apc.2005.19.526
[5] B. Thomas, A. Nyamathi and S. Swaminathan, “Impact of
HIV/AIDS on Mothers in Southern India: A Qualitative
Study,” AIDS and Behavior, Vol. 13, No. 5, 2009, pp.
989-996. doi:10.1007/s10461-008-9478-x
[6] M. Kurien, K. Thomas, R. C. Ahuja , A. Patel, P. R. Shyla,
N. Wig, M. Mangalani, Sathyanathan, A. Kasthuri, B.
Vyas, A. Brogen, T. D. Sudarsanam, A. Chaturvedi, O. C.
Abraham, P. Tharyan, K. G. Selvaraj and J. Mathew, “In-
diaCLEN HIV Screening Study Group. Screening for
HIV Infection by Health Professionals in India,” The Na-
tional Medical Journal of India, Vol. 20, No. 2, 2007, pp.
59-66.
[7] C. Reis, M. Heisler, L. L. Amowitz, R. S. Moreland, J. O.
Mafeni, C. Anyamele and V. Iacopino, “Discriminatory
Attitudes and Practices by Health Workers toward Pa-
tients with HIV/AIDS in Nigeria,” PLoS M edic ine , Vol. 2,
No. 8, 2005, p. e246. doi:10.1371/journal.pmed.0020246
[8] A. O. Aisien and M. O. Shobowale, “Health Care work-
ers’ Knowledge on HIV and AIDS: Universal Precautions
and Attitude towards PLWHA in Benin-City, Nigeria,”
Nigerian Journal Clinical Practice, Vol. 8, No. 2, 2005,
pp. 74-82.
[9] S. Bermingham and S. Kippax, “HIV-Related Discrimi-
nation: A Survey of New South Wales General Practitio-
ners,” The Australian and New Zealand Journal Public
Health, Vol. 22, No. 1, 1998, pp. 92-97.
doi:10.1111/j.1467-842X.1998.tb01151.x
[10] T. V. McCann and R. J. Sharkey, “Educational Interven-
tion with International Nurses and Changes in Knowledge,
Attitudes and Willingness to Provide Care to Patients
with HIV/AIDS,” Journal Advanced Nursing, Vol. 27,
No. 2, 1998, pp. 267-273.
doi:10.1046/j.1365-2648.1998.00513.x
[11] M. Fusilier, M. R. Manning, A. J. Santini Villar and D. T.
Rodriguez, “AIDS Knowledge and Attitudes of Health-
Care Workers in Mexico,” The Journal of Social Psycho-
logy, Vol. 138, No. 2, 1998, pp. 203-210.
doi:10.1080/00224549809600371
[12] U. Sambamoorthi, J. Walkup, M. Olfson and S. Crystal,
“Antidepressant Treatment and Health Services Utiliza-
tion among HIV-Infected Medicaid Patients Diagnosed
with Depression,” Journal of Genenal Internl Medicine,
Vol. 15, No. 5, 2000, pp. 311-320.
doi:10.1046/j.1525-1497.2000.06219.x
[13] R. N. Alves, M. J. Kovacs, R. Stall and V. Paiva, “Psy-
chosocial Aspects of HIV Infection among Women in
Brazil,” Revista de Saúde Pública, Vol. 36, Supplement 4,
2002, pp. 32-39.
Copyright © 2011 SciRes. WJA