S. Nagata et al. / Open Journal of Pediatrics, 2011, 1, 27-29
28
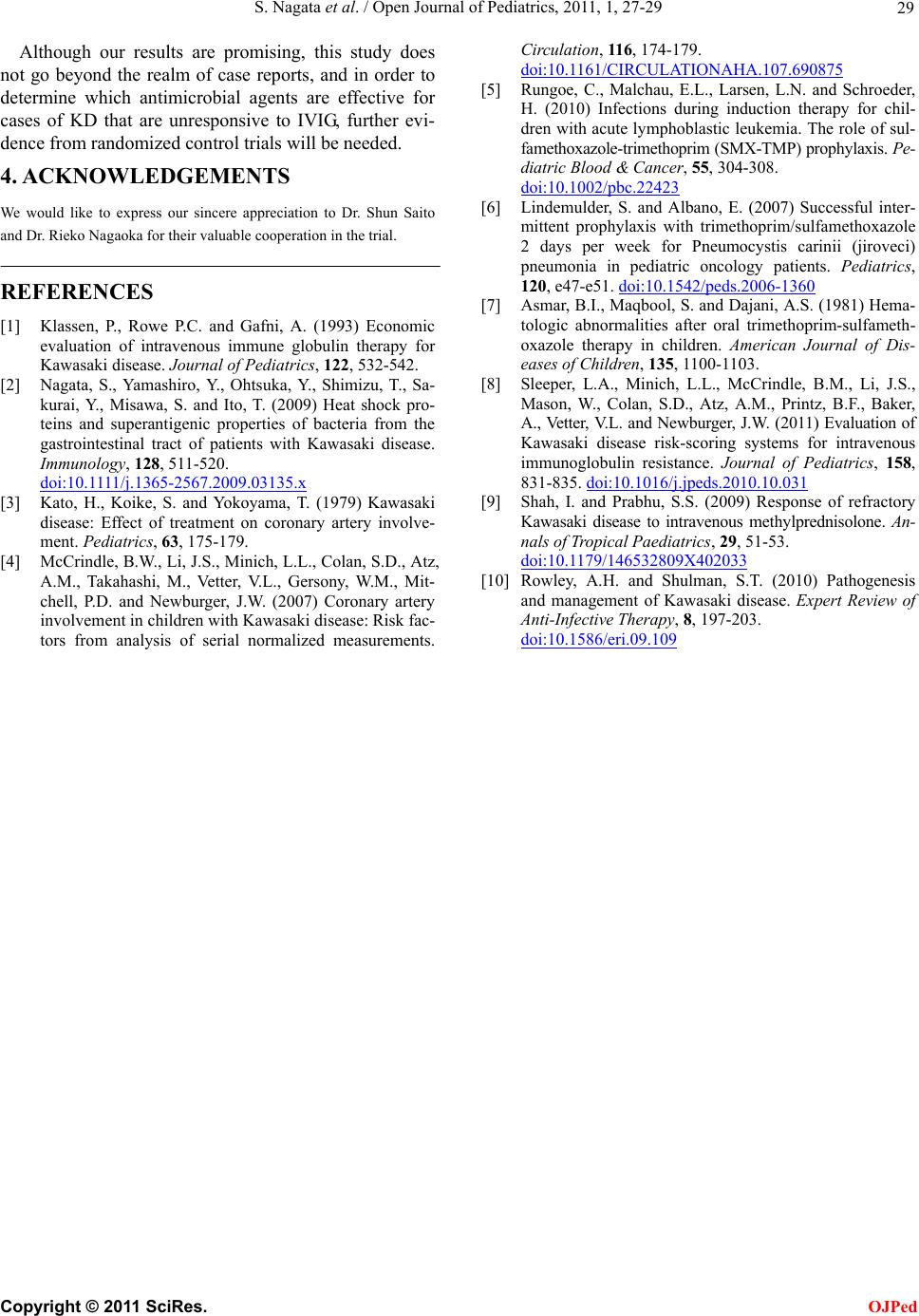
Table 1. Demographic characteristics of the patients with Ka-
wasaki disease.
Treatment
Case Age Sex 1st 2nd 3rd
Hospital
day
of the 1st
treatment
PSL used
concomitantly
with
SMX-TMP
1 5 m M IVIG IVP IVIG 5 2 mg/kg/d
2 10 m M IVIG IVP IVIG 5 1 mg/kg/d
3 2 y 4 m M IVIG IVP IVIG 5 2 mg/kg/d
4 4 y 6 m M IVIG IVIG IVP 4 1 mg/kg/d
5 5 y 3 m M IVIG IVIG IVP 5 1 mg/kg/d
6 10 m F IVIG IVIG IVP 7 2 mg/kg/d
7 2 y 3 m F IVIG IVP IVIG 5 1 mg/kg/d
SMX-TMP: sulfamethoxazole trimethoprim; IVIG; intravenous immuno-
globulin; IVP: pulsed in traveno us methylpre dnisolone; PSL: pr ednisolone.
these therapies as well, and no decrease in fever was
observed for 24 hours or more, one of the authors (SN)
was consulted, and upon receiving authorization from
the families of the patients, the use of SMX-TMP was
attempted.
At the time of the co nsult, 5 of the 7 cases already had
coronary artery aneurysms, and in 1 case that had been
diagnosed and treated late, giant aneurysms had formed.
In blood tests of the patients performed immediately be-
fore starting SMX-TMP administration, the C reactive
protein (CRP) values were 6.9 to 16.4 mg/dl (mean: 11.8).
In all cases, SMX-TMP was orally administered 2 times
per day at a dose of 0.04 g/kg/time, which is the general
dose for infants, for 5 consecutive days. For concomitant
treatment, aspirin was administered 3 times per day at 10
mg/kg/time, and prednisolone was administered orally at
1 - 2 mg/kg/ day as supp ort i ve therapy fo r IVP.
After SMX-TMP administration, a decline in fever
was observed w ithin 2 days (mean: 1.5 days) in 6 out of
the 7 cases (Ta bl e 2 ). In the case that had formed giant
aneurysms, a decrease in the fever was observed after 8
days. In the blood tests of the patients taken 1 week after
SMX-TMP administration, the CRP values were 4.7 to
17.2 mg/dL (mean: 8.3). At 2 weeks after SMX-TMP
administration, the coronary lesions had undergone ei-
ther minimal growth or had regressed, with the excep-
tion of the 1 case that had formed giant aneurysms. In
this case, an enlargement of the aneurysms was observed.
In all of the cases, no side effects that were believed to
have been caused by SMX-TMP were observed during
the course of treatment or follow-up.
3. DISCUSSION
It is often considered common knowledge that antimicr-
obial agents are ineffective for KD [3]. In 6 of the 7 ca se s
described in this study, the KD was unresponsive to
IVIG, but there was a decrease in fever within 2 days of
starting SMX-TMP administration. Because concomitant
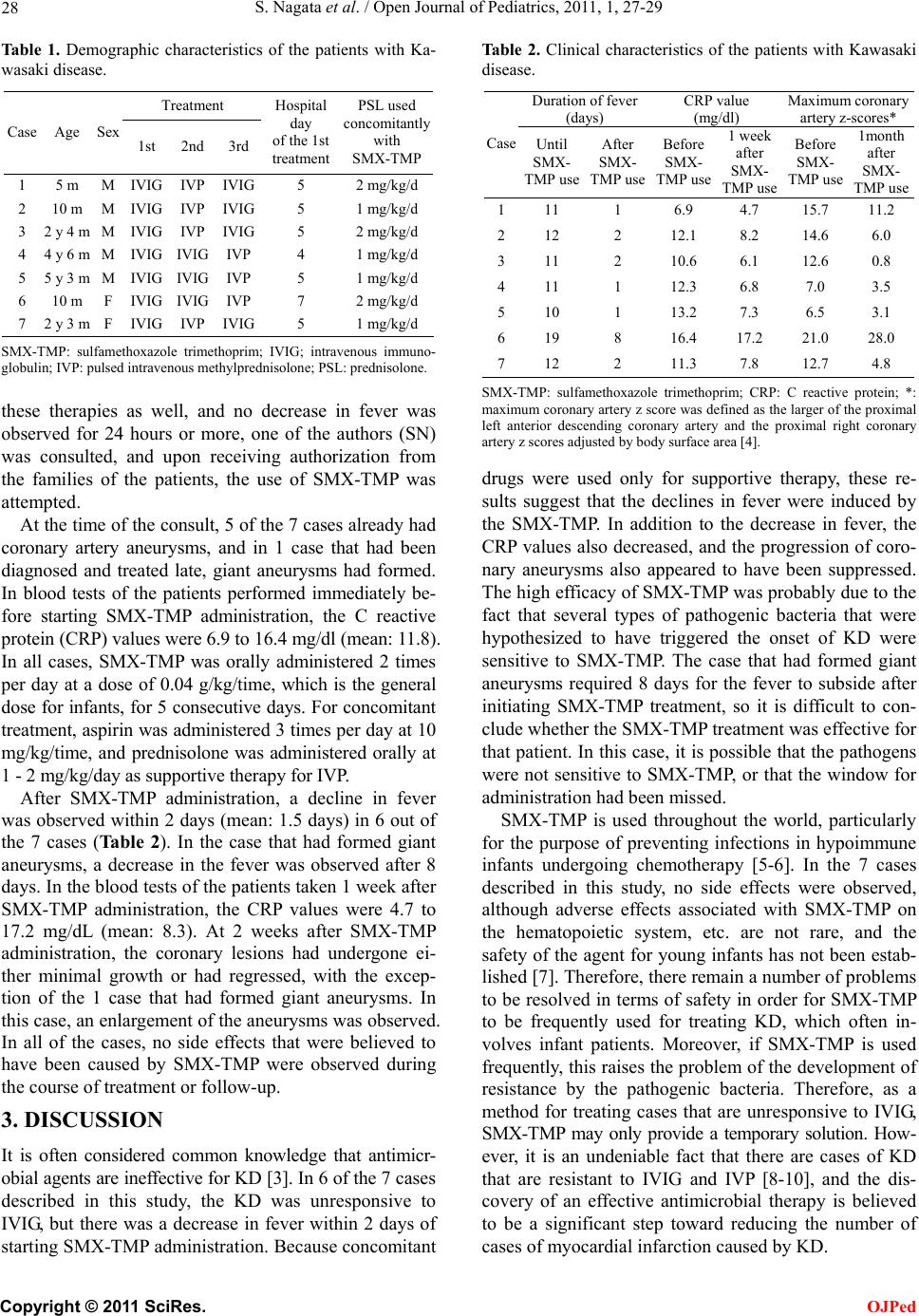
Table 2. Clinical characteristics of the patients with Kawasaki
disease.
Duration of fever
(days) CRP value
(mg/dl) Maximum cor onary
artery z-scores*
Case Until
SMX-
TMP use
After
SMX-
TMP use
Before
SMX-
TMP use
1 week
after
SMX-
TMP use
Before
SMX-
TMP use
1month
after
SMX-
TMP use
111 1 6.9 4.7 15.7 11.2
212 2 12.1 8.2 14.6 6.0
311 2 10.6 6.1 12.6 0.8
411 1 12.3 6.8 7.0 3.5
510 1 13.2 7.3 6.5 3.1
619 8 16.4 17.2 21.0 28.0
712 2 11.3 7.8 12.7 4.8
SMX-TMP: sulfamethoxazole trimethoprim; CRP: C reactive protein; *:
maximum coronary artery z score was defined as the larger of the proximal
left anterior descending coronary artery and the proximal right coronary
artery z score s adjusted by body surface area [4].
drugs were used only for supportive therapy, these re-
sults suggest that the declines in fever were induced by
the SMX-TMP. In addition to the decrease in fever, the
CRP values also decreased, and the progression of coro-
nary aneurysms also appeared to have been suppressed.
The high efficacy of SMX-TMP w as probab ly due to the
fact that several types of pathogenic bacteria that were
hypothesized to have triggered the onset of KD were
sensitive to SMX-TMP. The case that had formed giant
aneurysms required 8 days for the fever to subside after
initiating SMX-TMP treatment, so it is difficult to con-
clude whether the SMX-TMP treatment was effective for
that patient. In this case, it is possible that the pathogens
were not sensitive to SMX-TMP, or that the window for
administration had been missed.
SMX-TMP is used throughout the world, particularly
for the purpose of preventing infections in hypoimmune
infants undergoing chemotherapy [5-6]. In the 7 cases
described in this study, no side effects were observed,
although adverse effects associated with SMX-TMP on
the hematopoietic system, etc. are not rare, and the
safety of the agen t for young infants has not been estab-
lished [7]. Therefore, there remain a number of problems
to be resolved in terms of safety in o rder for SMX-TMP
to be frequently used for treating KD, which often in-
volves infant patients. Moreover, if SMX-TMP is used
frequently, th is raises the problem of the development of
resistance by the pathogenic bacteria. Therefore, as a
method for treating cases that are unresponsive to IVIG,
SMX-TMP may only provide a temporary solution. How-
ever, it is an undeniable fact that there are cases of KD
that are resistant to IVIG and IVP [8-10], and the dis-
covery of an effective antimicrobial therapy is believed
to be a significant step toward reducing the number of
cases of myocardial infarction caused by KD.
C
opyright © 2011 SciRes. OJPed