T. MUHONEN ET AL.
588
pants who had university education or managerial position
scored significantly higher on optimism, but optimism was not
related to gender, which is in line with earlier studies (Muhonen
& Torkelson, 2005).
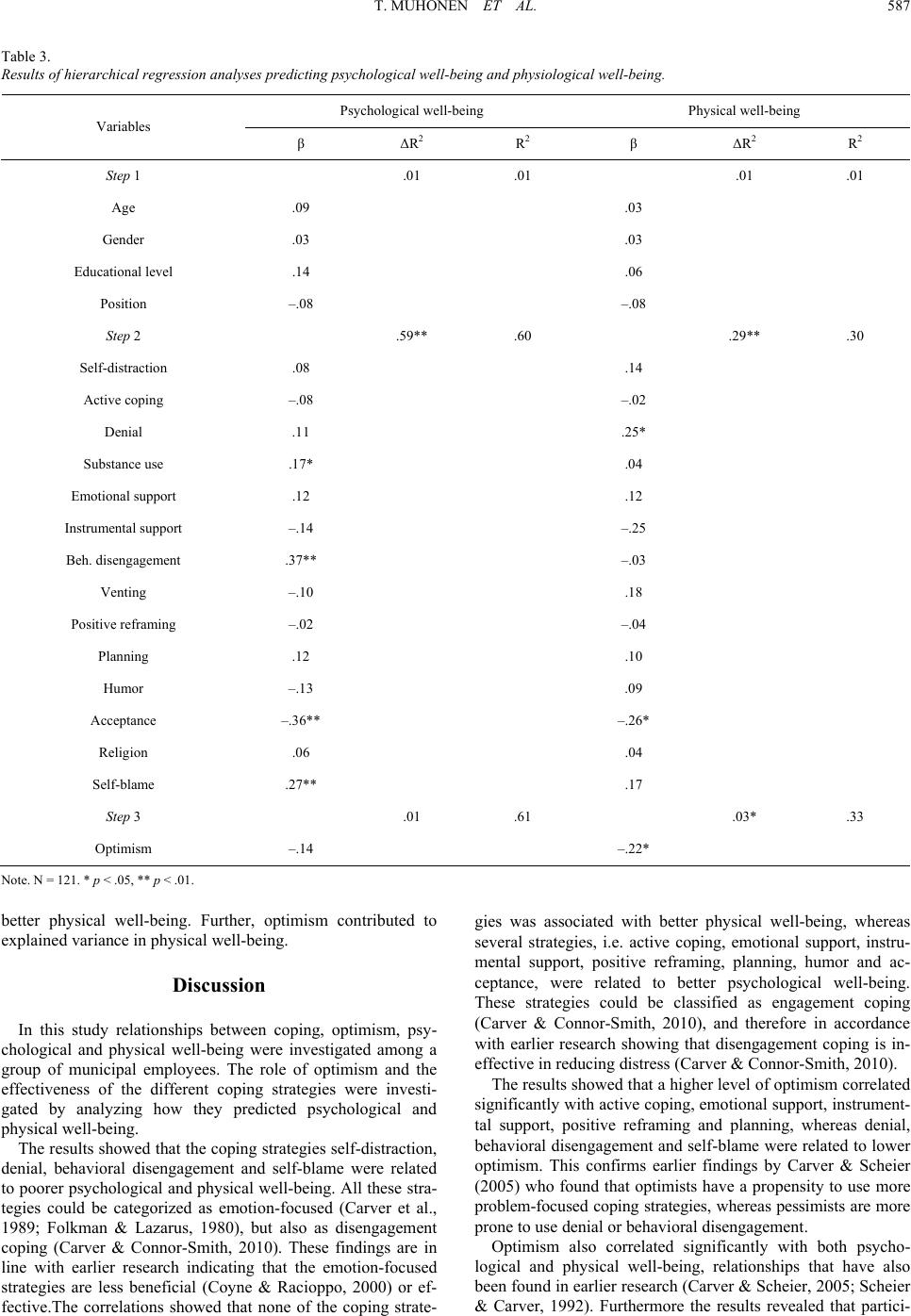
The results of the multiple regression analyses showed that
none of the background variables predicted psychological or
physical well-being. When it comes to coping, the results re-
vealed a somewhat different pattern for psychological and
physical well-being. Substance use, behavioral disengagement
and self-blame were related to poorer psychological well-being,
while acceptance was associated with better psychological
well-being. Only two of the coping strategies, namely denial
and acceptance, acted as predictors for physical well-being.
Denial was related to poorer physical well-being, whereas ac-
ceptance was related to better physical well-being. The results
of the study indicate that the most adaptive or effective coping
strategy when it comes to both psychological and physical
well-being was acceptance. The distinction between disenga-
gement and engagement coping (Carver & Connor-Smith, 2010)
is supported by the results of the study. The coping strategies
that predicted poorer psychological well-being, namely sub-
stance use, behavioral disengagement and self-blame, can be
classified as disengagement coping, whereas the coping stra-
tegy acceptance, which predicted both psychological and physi-
cal well-being, can be classified as engagement coping (Carver
& Connor-Smith, 2010). Disengagement coping in the form of
denial appeared to be ineffective, whereas engagement coping
in the form of acceptance seemed to be effective when it comes
to psychological and physical well-being. In earlier studies both
of these strategies have been categorized as emotion-focused
coping despite the fact that these strategies can lead to different
outcomes (Carver & Scheier, 2005). Denial is a strategy that
means refusing to face reality and attempting to rely on a view
that is no longer relevant, whereas acceptance indicates re-
structuring the experiences in order to cope with the reality of
the situation (Carver & Scheier, 2005).
The relationship between optimism and well-being appeared
to be somewhat inconclusive. Even though optimism correlated
significantly with both psychological and physical well-being,
it only predicted physical but not psychological well-being
when all the other variables in the model were controlled for.
This is a somewhat puzzling finding that needs to be investi-
gated further.
There are some limitations in this study that should be taken
into consideration. The number of participants is rather limited,
consisting of employees who represent a broad range of occu-
pations in the municipal sector. Some of the alpha values for
the coping scales, e.g. acceptance, denial, were somewhat low.
Since the reliability coefficient is related to the number of items
per scale (Cortina, 1993), it can be difficult to attain high reli-
ability values for scales that only consists of two items, as in
Brief COPE. And finally, since this a cross-sectional study, no
causal conclusions can be drawn.
In sum, the results of the study support the classification of
coping strategies into disengagement and engagement coping,
rather than using the emotion-focused and problem-focused dis-
tinction. The most adaptive or effective coping strategy con-
cerning psychological and physical well-being was acceptance,
which can be classified as engagement coping. Ineffective stra-
tegies regarding psychological well-being included disengage-
ment coping strategies such as substance use, behavioral disen-
gagement and self-blame. An ineffective strategy regarding
physiological well-being was denial, which can be classified as
a disengagement strategy. Optimism correlated significantly
with both psychological and physical well-being. However,
when all the variables in the model were included in the regres-
sion analysis, optimism explained additional variance in physi-
cal well-being but not in psychological wellbeing.
Considering the high rate of stress in current working life, it
is important to investigate further the effectiveness of disen-
gagement and engagement coping in order to be able to streng-
then coping capacity among employees.
References
Bhagat, R. S., Allie, S. M., & Ford, D. L. Jr. (1991). Organizational
stress, personal life stress and symptoms of life strain: An inquiry
into the moderating role of styles of coping. Journal of Social Be-
havior and Personality, 6, 163-184.
Carver, C. S. (1997). You want to measure coping but your protocol’s
too long: Consider the Brief COPE. International Journal of Behav-
ioral Medicine, 4, 92-100. doi:10.1207/s15327558ijbm0401_6
Carver, C. S., & Connor-Smith, J. (2010). Personality and coping.
Annual Review of Psychology, 61, 679-704.
doi:10.1146/annurev.psych.093008.100352
Carver, C. S., & Scheier, M. F. (2005). Optimism. In C. R. Snyder and
S. J. Lopez, (Eds.) Handbook of positive psychology (pp. 231-243).
New York: Oxford University Press.
Carver, C. S., Scheier, M. F., & Weintraub, J. K. (1989). Assessing
coping strategies: A theoretically based approach. Journal of Per-
sonality and Social P sychology, 56, 267-283.
doi:10.1037/0022-3514.56.2.267
Cortina, J. M. (1993). What is coefficient alpha? An examination of
theory and applications. Jou rnal of Applied Psychology, 78, 98-104.
doi:10.1037/0021-9010.78.1.98
Coyne, J. C., & Racioppo, M. W. (2000). Never the twain shall meet?
Closing the gap between coping research and clinical intervention
research. American P sy ch ol og is t, 55, 655-664.
doi:10.1037/0003-066X.55.6.655
Cunningham, J. L., De La Rosa, G. M., & Jex, S. M. (2008). The dy-
namic influence of individual characteristics on employees
well-being: a review of theory, research and future directions. In K.
Näswall, J. Hellgren and M. Sverke (Eds.), The individual in the
changing working life (pp. 258-283). Cambridge: Cambridge Uni-
versity Press.
Eriksen, H. R., Ihlebæk C., & Ursin, H. (1999). A scoring system for
subjective health complaints (SCH). Scandinavian Journal of Public
Health, 1, 63-72. doi:10.1177/14034948990270010401
Farley, T., Galves, A., Dickinson, M., & Perez, M. J. D. (2005). Stress,
coping, and health. A comparison of Mexican immigrants, Mexican-
Americans, and Non-Hispanic Whites. Journal of Immigrant Health,
7, 213-220. doi:10.1007/s10903-005-3678-5
Folkman, S., & Lazarus, R. S. (1980). An analysis of coping in mid-
dle-aged community sample. Journal of Health and Social Behavior,
21, 219-239. doi:10.2307/2136617
Goldberg, D. P. (1972). The detection of psychiatric illness by ques-
tionnaire. Oxford: Oxford University Press.
Lazarus, R. S., & Folkman, S. (1984). Stress, appraisal, and coping.
New York: Springer Publishing Company.
Meyer, B. (2001). Coping with severe mental illness: Relations of the
Brief COPE with symptoms, functioning and well-being. Journal of
Psychopathology and Behavioral Assessment, 23, 265-277.
doi:10.1023/A:1012731520781
Muhonen, T. (2010). Feeling double locked-in at work―implications
for health and job satisfaction among municipal employees. WORK,
36.
Muhonen, T., & Torkelson, E. (2005). Kortversioner av frågeformulär
inom arbets-och hälsopsykologi―om att mäta coping och optimism.
Nordisk Psykologi, 57, 288-297.
Pienaar, J. (2008). Skeleton key or siren song: is coping the answer to
balancing work and well-being? In K. Näswall, J. Hellgren and M.
Sverke (Eds.), The individual in the changing working life (pp.
235-257). Cambridge: Cambridge University Press.
Sconfienza, C. (1998). Mätning av psykiskt välbefinnande bland
ungdomar i Sverige. Användning av GHQ-12. [Measuring mental