Y. T. Zhou et al. / World Journal of Neuroscience 1 (2011) 28-30 29
function test, and coagu lation studies were all normal. A
diagnosis of SAH was suspected (Hunt-Hess grade I
grade).
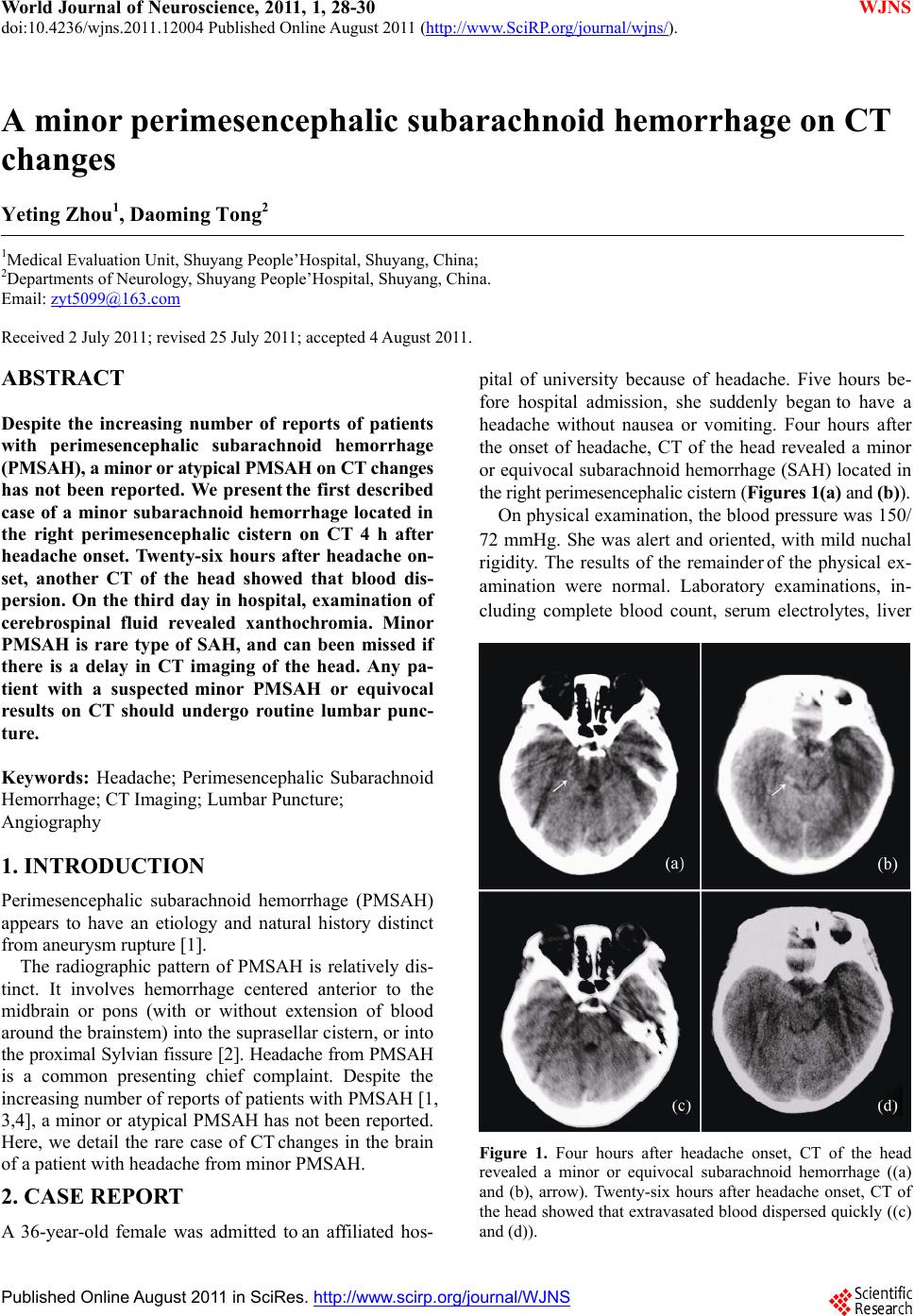
Twenty-six hours after the onset of headache, CT of
the head showed that extravasated blood dispersed
quickly (Figures 1(c) and (d)). On the third day of hos-
pital admission, examination of cerebrospinal fluid (CSF)
revealed xanthochromia, and cytologic examination of
CSF showed metemoglobin; these are characteristic fea-
tures of subarachnoid hemorrhage. On the fifth day of
hospital admission, digital subtraction cerebral angiogra-
phy did not demonstrate an aneurysm stemming from the
basilar, anterior cerebral, middle cerebral or posterior
cerebral arteries. The patient reported no specific risk
factors for arterial dissection (e.g., trauma) and had no
significant medical history of hypertension. We made a
diagnosis of minor PMSAH.
The patient was treated with intravenous anti-fibri-
nolytic agents. Within 3 days her symptoms and signs
had resolved. She was discharged home in excellent con-
dition 2 weeks after hospital admission. No further epi-
sodes occurred during the subsequent 12-month follow-
up.
3. CONCLUSION
PMSAH is diagnosed on the basis of CT or MRI. These
imaging methods demonstrate a localized area of hem-
orrhage centered within the perimesencephalic or pre-
pontine cisterns without intracerebral or intraventricular
extension [1,3]. Very few reports describe CT changes of
minor or atypical PMSAH.
Currently our patient, within 4 h after the onset of a
sudden headache, a minor or equivocal area of hemor-
rhage in the right perimesencephalic cistern was seen on
head CT. This suggested the possibility of minor PMSAH.
Twenty-six hours after headache onset, CT of the head
showed that extravasated blood had dispersed quickly.
On the third day of hospital admission, our patient re-
vealed xanthochromia by lumbar puncture, and cytologic
examination of CSF showed metemoglobin. A minor
PMSAH was demonstrated.
PMSAHs account for ~5% of all cases of subarach-
noid hemorrhage [5]. However, in our case, a typical
PMSAH was not revealed on head CT 26 h after head-
ache onset. Hence, the diagnosis of minor PMSAH
would have been missed if our patient with this condi-
tion had not presented to a hospital or delayed in the
time of CT scan.
CT may be less sensitive in patients with a SAH pre-
senting with “minor leaks” or normal neurological status
[6]. A diagnosis of SAH with a negative CT of the head
accounts for 7% of cases with SAH [7]. Therefore, we
speculated that the true prevalence of PMSAH may be
>5%. This also suggests that some patients with a SAH
with a negative finding on head CT may have a minor
PMSAH. One explanation of this finding is that some
patients have only a small amount of blood on initial CT
imaging and, in some patients, the extravasation might be
too small to be detected [6]. The present study showed
that a low grade on the Hunt-Hess scale, normal d iast olic
blood pressure, and a delay in the time of CT imaging
after hospital admission could be the cause of SAH with
negative findings on head CT [8]. Lumbar puncture
should therefore be carried out in any patient with sus-
pected SAH and negative (or equivocal) results on head
CT [9].
Studies indicate that most of the causes in patients
with PMSAH are non-aneurysmal [3,4], but some can
also be aneurismal [1,3,10]. In our patient, diagnostic
cerebral angiography did not reveal an aneurysm, but
aneurysmal PMSAH was not excluded. Minor PMSAH
is rare. Our case did not reveal typical PMSAH on CT. It
also serves as a reminder of the importance of lumbar
puncture and the variability of angiographic results dis-
played by PMSAH. PMSAH accounts for approximately
one-third of cases of non-aneurysmal SAH [5]. The re-
maining cases of non-aneurysmal SAH are heterogene-
ous, including SAH caused by vascular malformations,
venous bleeding [11], and not confined to cases of idio-
pathic SAH [5], Aneurysm rupture occasionally pro-
duces a PMSAH-like pattern of bleeding [10,12], In a
review of 3 large series concerning the neurological
complications associated with DSA, the complication
rate for patients with SAH was 0.25% [13], so studies
recommemded that CT angiography only is the most
beneficial approach in patients with a perimesencephalic
hemorrhage on CT, and accurately excludes and detects
vertebrobasilar aneurysms [12,14].
In conclusion, minor PMSAH is rare type of SAH,
and can been missed if there is a delay in CT imaging of
the head. Any patient with a suspected minor PMSAH or
equivocal results on CT should undergo routine lumbar
puncture.
REFERENCES
[1] Rinkel, G.J.E., Wijdicks, E.F.M., Hasan, D., et al. (1991)
Outcome in patients with subarachnoid haemorrhage and
negative angiography according to pattern of haemor-
rhage on computed tomography. Lancet, 338, 964-968.
doi:10.1016/0140-6736(91)91836-J
[2] Schwartz, T.H. and Solomon, R.A. (1996) Perimesen-
cephalic nonaneurysmal subarachnoid hemorrhage: Re-
view of the literature. Neurosurgery, 39, 433-440.
[3] Van Gijn, J., Van Dongen, K.J., Vermeulen, M., et al.
(1985) Perimesencephalic hemorrhage: A nonaneurysmal
and benign form of subarachnoid hemorrhage. Neurology,
35, 493-497.
C
opyright © 2011 SciRes. WJNS