Vol.1, No.2, 111-116 (2009)
doi:10.4236/health.2009.12018
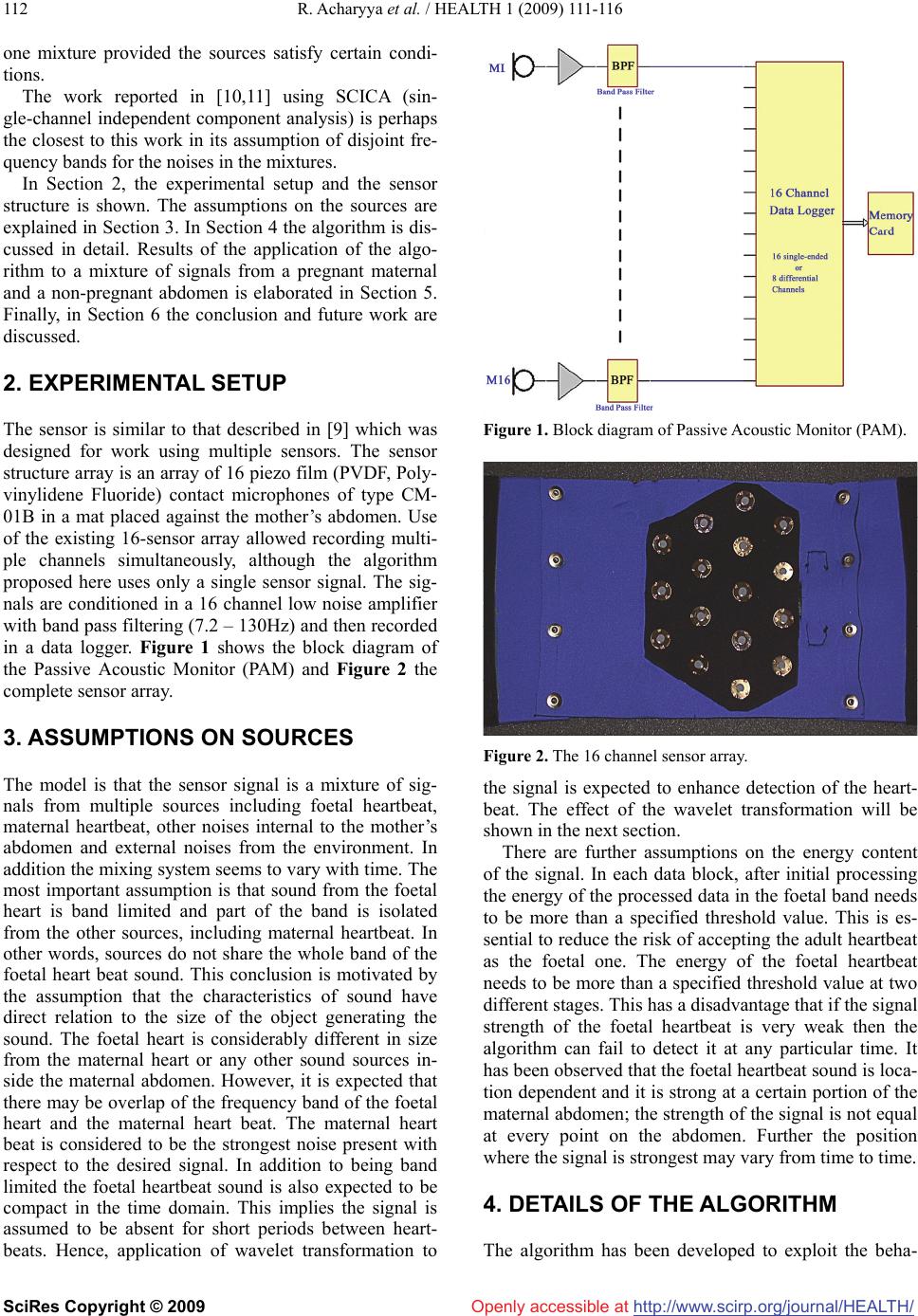
SciRes
Copyright © 2009 Openly accessible at http://www.scirp.org/journal/HEALTH/
Health
Non-invasive foetal heartbeat rate extraction from an
underdetermined single signal
Ranjan Acharyya1, Neil L Scott1, Paul D Teal2
1Industrial Research Ltd, Wellington, New Zealand; r.achary ya@i rl.c ri.nz, n.scottt@irl.cri.nz
2Victoria University of Wellington, Wellington, New Zealand; mailto:paul.teal@vuw.ac.nz
Received 17 June 2009; revised 20 July 2009; accepted 23 July 2009.
ABSTRACT
Extraction of foetal heartbeat rate from a single
passive sound sensor on the mother’s abdomen
is demonstrated. The extraction is based on the
assumption that a disjoint band of frequencies
exist and foetal signal is concentrated in this
band, and further that it can be represented
conveniently as a set of wavelet coefficients.
The algorithm has been applied to each stream
of data obtained from six different channels and
the detection performance is elaborated. The
algorithm has also been tested on signals from
non-pregnant abdomens to show successful
rejection of adult heartbeat. The extraction of
the desired signal is done in two stages so as to
eliminate components from the maternal heart-
beat.
Keywords: Underdetermined System; Foetal
Heartbeat Rate; Wavelet, Blind Source Separation;
Non-Invasive; Passive.
1. INTRODUCTION
Monitoring of foetal heartrate using a non-invasive tech-
nique is still a challenging problem with a variety of
approaches [1,2]. Usually, foetal heartbeat is monitored
using a Doppler ultrasound device which transmits ul-
trasonic sound waves into the uterus. Most researchers
consider that the power used in these devices is perfectly
safe, although there are some exceptions [6]. In many
cases women prefer that ultrasound is not used on them.
Detailed motivation for development and use of accurate,
non-invasive techniques for monitoring the foetal heart
is covered in the excellent introduction of [1]. This paper
describes a method for detection of the foetal heart with
a passive acoustic monitoring device (PAM). The proc-
ess involves collection of signals with microphones and
subsequent signal processing.
The passive monitoring of foetal heartrate may be
considered as one class of Blind source separation (BSS)
problem, which has been an active research area for sev-
eral decades now. It refers to the problem of estimating
the original sources from a mixture. In most cases the
mixing system and the number of sources are unknown.
Sensors placed on the maternal abdomen provide signals
which are mixtures of an unknown number of sources
and the nature of the mixing is also unknown. In this
section a quick review of other techniques and overview
of the technique of this paper is given.
Independent Component Analysis (ICA) is a tech-
nique to obtain statistically independent components
from a mixture and a solution technique for BSS prob-
lems. One way to categorise BSS problems is based on
the number of sensor and source signals. Three different
scenarios are, the number of sensors are greater than,
equal to or less than the number of sources. The third
case, which is equivalent to solving for an underdeter-
mined system or for an overcomplete basis, resembles
the problem at hand. Detail and an in-depth analysis of
algorithms can be found in [3,4,5]. A well known algo-
rithm for sparse sources is known as DUET (degenerate
unmixing estimation techniques) [5], which does time-
frequency masking. The applicability of the algorithm
depends on a W disjoint orthogonal [5] condition of the
sources and availability of at least two sensor signals.
Extraction of foetal heartrate using ICA [7] has been
attempted in [8] and some interesting results were ob-
tained. In this paper a new algorithm is developed based
on certain assumptions on the foetal heartbeat signal.
This paper is an extension of an earlier work [9] demon-
strating estimation of the foetal heartrate by frequency
masking. A crucial difference of this paper compared to
[9] is that it avoids filtering of the signal in the time do-
main. Filtering in the time domain was done in [9] to
suppress the maternal heartbeat. The issue of suppress-
ing the maternal signal in the overlap region is addressed
in this paper by performing the filtering in two steps. In
addition to filtering in the frequency domain the resolu-
tion of the signals is enhanced by using a wavelet trans-
formation. The process is discussed in detail in later sec-
tions. The method described in this paper requires only