 Journal of Environmental Protection, 2011, 2, 683-691 doi:10.4236/jep.2011.26079 Published Online August 2011 (http://www.SciRP.org/journal/jep) Copyright © 2011 SciRes. JEP 683 Persistent Organochlorine Exposure and Pregnancy Loss: A Prospective Cohort Study Anna Z. Pollack1, Germaine M. Buck Louis1, Courtney D. Lynch2, Paul J. Kostyniak3 1Epidemiology Branch, Eunice Kennedy Shriver National Institute of Child Health and Human Development, Bethesda, USA; 2Division of Epidemiology & Department of Obstetrics and Gynecology, Ohio State University, Columbus, USA; 3Department of Pharmacology and Toxicology, School of Medicine and Biomedical Sciences, University of New York, Buffalo, USA. Email: pollacka@mail.nih.gov Received March 23rd, 2011; revised May 6th, 2011; accepted June 21st, 2011. ABSTRACT Polychlorinated biphenyls (PCBs) and 1,1-dichloro-2,2-bis(p-chlorophenyl)ethylene (DDE) are suspected reproductive toxicants. We assessed serum concentration of 76 PCB congeners, DDE, and risk of human chorionic gonadotropin confirmed pregnancy loss among 79 women followed for up to 12 menstrual cycles or until pregnancy. 55 women had live births, 14 experienced pregnancy losses, and 10 did not achieve pregnancy. PCBs and DDE were quantified using gas chromatography with electron capture. PCBs were grouped a priori by biologic activity. Cox proportional hazard regression adjusting for age (categorized 24 - 29, 30 - 34) and average stand ardized alcoho l and cigarette in take (con- tinuous) was used to estimate hazard ratios (HR) of pregnancy loss. Estrogenic PCBs (HR = 1.66, 95% CI: 0.68, 4.02), anti-estrogenic PCBs (HR = 0.10, 95% CI: <0.01, 67.07) and DDE (HR = 1.43, 95% CI: 0.45, 4.52) were not statisti- cally significantly associated with pregnancy loss. Our results provide some signal that estrogenic and antiestrogenic PCBs may be differentially associated with pregnancy loss. Further research is needed to elucidate these associations. Keywords: 1,Dichloro-2,2-Bis(P-Chlorophenyl)Ethylene, Fecundity, Organochlorine, Polychlorinated Biphenyl, Pregnancy Loss 1. Introduction Fecundity is defined as the biologic capacity for repro- duction [1] and can be conceptualized to include im- pairments such as conception delay, infertility, or preg- nancy loss. Fecundity is an essential aspect when assess- ing potential reproductive or developmental toxicity of environmental agents. Exposures adversely impacting fecundity can be identified by estimating differences in the time-to-pregnancy among exposed women relative to unexposed women [2] or in estimating the risk of preg- nancy loss [3]. There has been speculation that a global reduction in human fecundity is underway [4]. Available evidence suggests that environmental agents, particularly the endocrine disrupting class of chemicals, may contrib- ute to this decline [5]. Recent reviews have summarized the available evi- dence regarding the reproductive and/or developmental toxicity (RADT) of persistent organochlorines such as polychlorinated biphenyls (PCBs) and 1,1-dichloro-2,2- bis(p-chlorophenyl)ethylene (DDE) [6-8]. Past research has attempted to assess the potential RADT of polyhalo- genated aromatic hydrocarbons in relation to human fe- cundity, but often has relied upon proxy exposure meas- urements such as PCB contaminated fish consumption [9,10], occupation [11], residence [12], or quantified se- rum or plasma concentrations often collected years fol- lowing reproductive outcomes [13,14]. Estimating the effect of environmental chemical exposure and preg- nancy loss is challenging for many reasons, including the high proportion of losses occurring prior to (woman/ clinical) recognition and the competing risk of infertility, in that women who do not conceive are not at risk of pregnancy loss. Prospective cohort designs with precon- ception recruitment of women or couples and with bio- monitoring of human chorionic gonadaotropin (hCG) pregnancy remains the gold standard for assessing envi- ronmental RADT, particularly those occurring in the sensitive periconceptional window [15,16]. While chal- lenging, the utility and feasibility of such approaches have been established [17]. Spontaneous pregnancy loss is a sensitive endpoint in- dicative of impaired fecundity. In relation to DDT expo- sure, pregnancy loss has been assessed by questionnaire 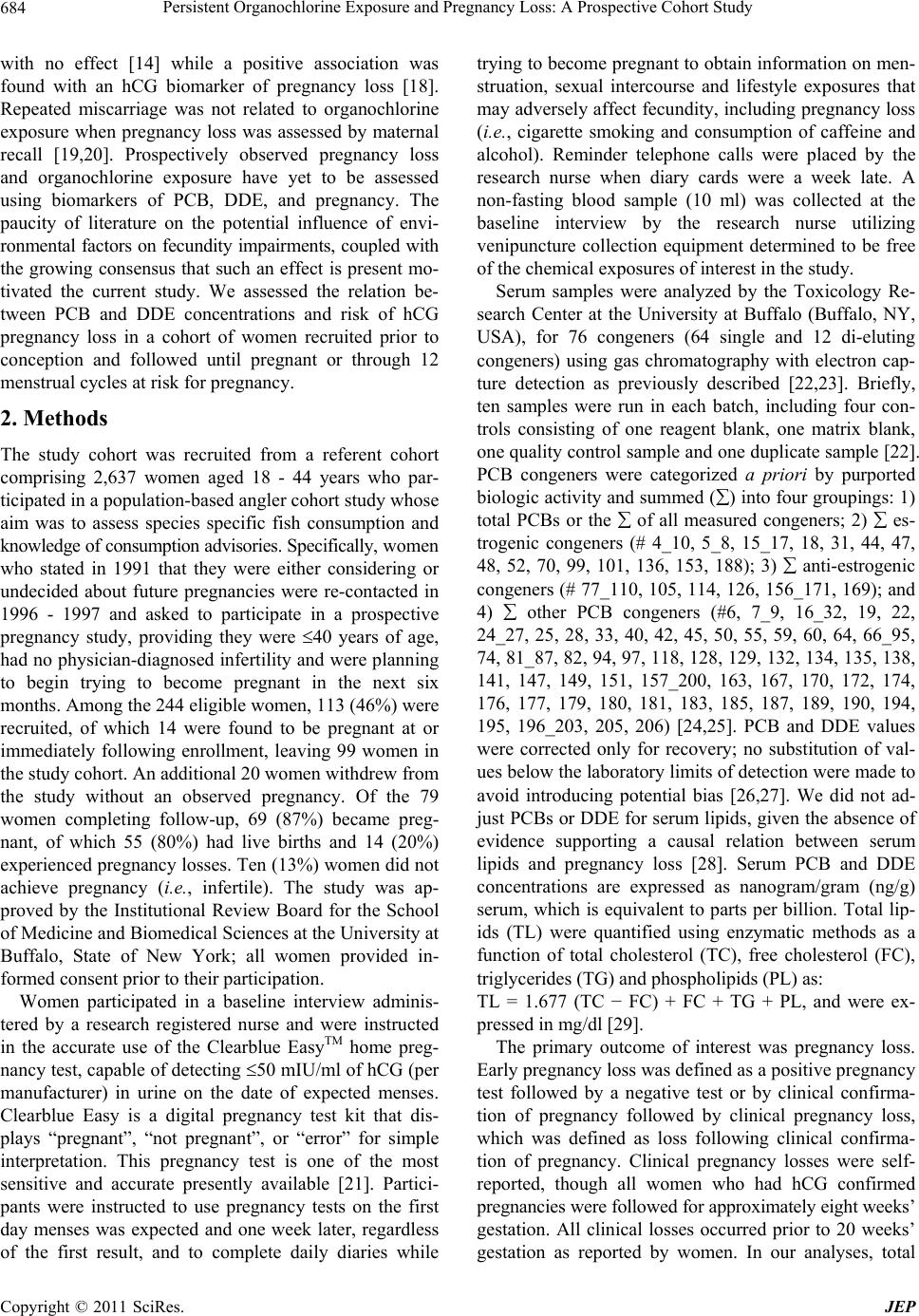 Persistent Organochlorine Exposure and Pregnancy Loss: A Prospective Cohort Study 684 with no effect [14] while a positive association was found with an hCG biomarker of pregnancy loss [18]. Repeated miscarriage was not related to organochlorine exposure when pregnancy loss was assessed by maternal recall [19,20]. Prospectively observed pregnancy loss and organochlorine exposure have yet to be assessed using biomarkers of PCB, DDE, and pregnancy. The paucity of literature on the potential influence of envi- ronmental factors on fecundity impairments, coupled with the growing consensus that such an effect is present mo- tivated the current study. We assessed the relation be- tween PCB and DDE concentrations and risk of hCG pregnancy loss in a cohort of women recruited prior to conception and followed until pregnant or through 12 menstrual cycles at risk for pregnancy. 2. Methods The study cohort was recruited from a referent cohort comprising 2,637 women aged 18 - 44 years who par- ticipated in a population-based angler cohort study whose aim was to assess species specific fish consumption and knowledge of consumption advisories. Specifically, women who stated in 1991 that they were either considering or undecided about future pregnancies were re-contacted in 1996 - 1997 and asked to participate in a prospective pregnancy study, providing they were 40 years of age, had no physician-diagnosed infertility and were planning to begin trying to become pregnant in the next six months. Among the 244 eligible women, 113 (46%) were recruited, of which 14 were found to be pregnant at or immediately following enrollment, leaving 99 women in the study cohort. An additional 20 women withdrew from the study without an observed pregnancy. Of the 79 women completing follow-up, 69 (87%) became preg- nant, of which 55 (80%) had live births and 14 (20%) experienced pregnancy losses. Ten (13%) women did not achieve pregnancy (i.e., infertile). The study was ap- proved by the Institutional Review Board for the School of Medicine and Biomedical Sciences at the University at Buffalo, State of New York; all women provided in- formed consent prior to their participation. Women participated in a baseline interview adminis- tered by a research registered nurse and were instructed in the accurate use of the Clearblue EasyTM home preg- nancy test, capable of detecting 50 mIU/ml of hCG (per manufacturer) in urine on the date of expected menses. Clearblue Easy is a digital pregnancy test kit that dis- plays “pregnant”, “not pregnant”, or “error” for simple interpretation. This pregnancy test is one of the most sensitive and accurate presently available [21]. Partici- pants were instructed to use pregnancy tests on the first day menses was expected and one week later, regardless of the first result, and to complete daily diaries while trying to become pregnant to obtain information on men- struation, sexual intercourse and lifestyle exposures that may adversely affect fecundity, including pregnancy loss (i.e., cigarette smoking and consumption of caffeine and alcohol). Reminder telephone calls were placed by the research nurse when diary cards were a week late. A non-fasting blood sample (10 ml) was collected at the baseline interview by the research nurse utilizing venipuncture collection equipment determined to be free of the chemical exposures of interest in the study. Serum samples were analyzed by the Toxicology Re- search Center at the University at Buffalo (Buffalo, NY, USA), for 76 congeners (64 single and 12 di-eluting congeners) using gas chromatography with electron cap- ture detection as previously described [22,23]. Briefly, ten samples were run in each batch, including four con- trols consisting of one reagent blank, one matrix blank, one quality control sample and one duplicate sample [22]. PCB congeners were categorized a priori by purported biologic activity and summed () into four groupings: 1) total PCBs or the of all measured congeners; 2) es- trogenic congeners (# 4_10, 5_8, 15_17, 18, 31, 44, 47, 48, 52, 70, 99, 101, 136, 153, 188); 3) anti-estrogenic congeners (# 77_110, 105, 114, 126, 156_171, 169); and 4) other PCB congeners (#6, 7_9, 16_32, 19, 22, 24_27, 25, 28, 33, 40, 42, 45, 50, 55, 59, 60, 64, 66_95, 74, 81_87, 82, 94, 97, 118, 128, 129, 132, 134, 135, 138, 141, 147, 149, 151, 157_200, 163, 167, 170, 172, 174, 176, 177, 179, 180, 181, 183, 185, 187, 189, 190, 194, 195, 196_203, 205, 206) [24,25]. PCB and DDE values were corrected only for recovery; no substitution of val- ues below the laboratory limits of detection were made to avoid introducing potential bias [26,27]. We did not ad- just PCBs or DDE for serum lipids, given the absence of evidence supporting a causal relation between serum lipids and pregnancy loss [28]. Serum PCB and DDE concentrations are expressed as nanogram/gram (ng/g) serum, which is equivalent to parts per billion. Total lip- ids (TL) were quantified using enzymatic methods as a function of total cholesterol (TC), free cholesterol (FC), triglycerides (TG) and phospholipids (PL) as: TL = 1.677 (TC − FC) + FC + TG + PL, and were ex- pressed in mg/dl [29]. The primary outcome of interest was pregnancy loss. Early pregnancy loss was defined as a positive pregnancy test followed by a negative test or by clinical confirma- tion of pregnancy followed by clinical pregnancy loss, which was defined as loss following clinical confirma- tion of pregnancy. Clinical pregnancy losses were self- reported, though all women who had hCG confirmed pregnancies were followed for approximately eight weeks’ gestation. All clinical losses occurred prior to 20 weeks’ gestation as reported by women. In our analyses, total Copyright © 2011 SciRes. JEP 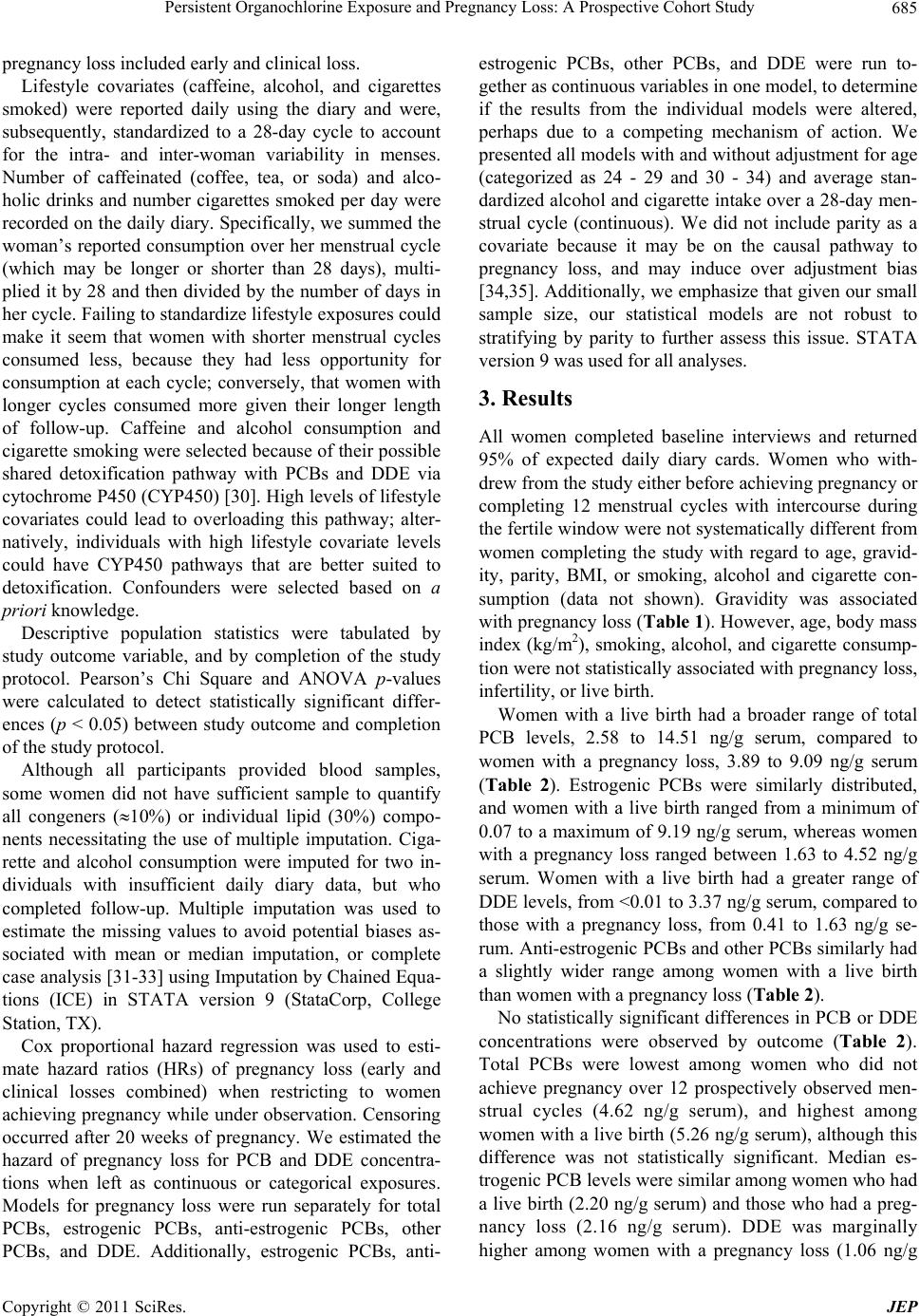 Persistent Organochlorine Exposure and Pregnancy Loss: A Prospective Cohort Study Copyright © 2011 SciRes. JEP 685 pregnancy loss included early and clinical loss. Lifestyle covariates (caffeine, alcohol, and cigarettes smoked) were reported daily using the diary and were, subsequently, standardized to a 28-day cycle to account for the intra- and inter-woman variability in menses. Number of caffeinated (coffee, tea, or soda) and alco- holic drinks and number cigarettes smoked per day were recorded on the daily diary. Specifically, we summed the woman’s reported consumption over her menstrual cycle (which may be longer or shorter than 28 days), multi- plied it by 28 and then divided by the number of days in her cycle. Failing to standardize lifestyle exposures could make it seem that women with shorter menstrual cycles consumed less, because they had less opportunity for consumption at each cycle; conversely, that women with longer cycles consumed more given their longer length of follow-up. Caffeine and alcohol consumption and cigarette smoking were selected because of their possible shared detoxification pathway with PCBs and DDE via cytochrome P450 (CYP450) [30]. High levels of lifestyle covariates could lead to overloading this pathway; alter- natively, individuals with high lifestyle covariate levels could have CYP450 pathways that are better suited to detoxification. Confounders were selected based on a priori knowledge. Descriptive population statistics were tabulated by study outcome variable, and by completion of the study protocol. Pearson’s Chi Square and ANOVA p-values were calculated to detect statistically significant differ- ences (p < 0.05) between study outcome and completion of the study protocol. Although all participants provided blood samples, some women did not have sufficient sample to quantify all congeners (10%) or individual lipid (30%) compo- nents necessitating the use of multiple imputation. Ciga- rette and alcohol consumption were imputed for two in- dividuals with insufficient daily diary data, but who completed follow-up. Multiple imputation was used to estimate the missing values to avoid potential biases as- sociated with mean or median imputation, or complete case analysis [31-33] using Imputation by Chained Equa- tions (ICE) in STATA version 9 (StataCorp, College Station, TX). Cox proportional hazard regression was used to esti- mate hazard ratios (HRs) of pregnancy loss (early and clinical losses combined) when restricting to women achieving pregnancy while under observation. Censoring occurred after 20 weeks of pregnancy. We estimated the hazard of pregnancy loss for PCB and DDE concentra- tions when left as continuous or categorical exposures. Models for pregnancy loss were run separately for total PCBs, estrogenic PCBs, anti-estrogenic PCBs, other PCBs, and DDE. Additionally, estrogenic PCBs, anti- estrogenic PCBs, other PCBs, and DDE were run to- gether as continuous variables in one model, to determine if the results from the individual models were altered, perhaps due to a competing mechanism of action. We presented all models with and without adjustment for age (categorized as 24 - 29 and 30 - 34) and average stan- dardized alcohol and cigarette intake over a 28-day men- strual cycle (continuous). We did not include parity as a covariate because it may be on the causal pathway to pregnancy loss, and may induce over adjustment bias [34,35]. Additionally, we emphasize that given our small sample size, our statistical models are not robust to stratifying by parity to further assess this issue. STATA version 9 was used for all analyses. 3. Results All women completed baseline interviews and returned 95% of expected daily diary cards. Women who with- drew from the study either before achieving pregnancy or completing 12 menstrual cycles with intercourse during the fertile window were not systematically different from women completing the study with regard to age, gravid- ity, parity, BMI, or smoking, alcohol and cigarette con- sumption (data not shown). Gravidity was associated with pregnancy loss (Table 1). However, age, body mass index (kg/m2), smoking, alcohol, and cigarette consump- tion were not statistically associated with pregnancy loss, infertility, or live birth. Women with a live birth had a broader range of total PCB levels, 2.58 to 14.51 ng/g serum, compared to women with a pregnancy loss, 3.89 to 9.09 ng/g serum (Table 2). Estrogenic PCBs were similarly distributed, and women with a live birth ranged from a minimum of 0.07 to a maximum of 9.19 ng/g serum, whereas women with a pregnancy loss ranged between 1.63 to 4.52 ng/g serum. Women with a live birth had a greater range of DDE levels, from <0.01 to 3.37 ng/g serum, compared to those with a pregnancy loss, from 0.41 to 1.63 ng/g se- rum. Anti-estrogenic PCBs and other PCBs similarly had a slightly wider range among women with a live birth than women with a pregnancy loss (Table 2). No statistically significant differences in PCB or DDE concentrations were observed by outcome (Table 2). Total PCBs were lowest among women who did not achieve pregnancy over 12 prospectively observed men- strual cycles (4.62 ng/g serum), and highest among women with a live birth (5.26 ng/g serum), although this difference was not statistically significant. Median es- trogenic PCB levels were similar among women who had a live birth (2.20 ng/g serum) and those who had a preg- nancy loss (2.16 ng/g serum). DDE was marginally higher among women with apregnancy loss (1.06 ng/g  Persistent Organochlorine Exposure and Pregnancy Loss: A Prospective Cohort Study 686 Table 1. Sociodemographic characteristics of cohort by study outcome (n = 79). Characteristic Live Birth n (%) Pregnancy Loss n (%) Infertile n (%) P value 55 (70) 14 (17) 10 (13) Age (in years) 0.25 <30 19 (34) 8 (57) 5 (50) 30 36 (65) 6 (43) 5 (50) Gravidity (# live births) 0.01 0 10 (18) 6 (43) 6 (75) 1 36 (65) 5 (36) 1 (12) 2+ 9 (16) 3 (21) 1 (12) Parity (# pregnancies) 0.10 0 8 (14) 5 (36) 5 (50) 1 24 (44) 4 (28) 3 (30) 2+ 23 (42) 5 (36) 2 (20) Body mass index (kg/m2) 0.88 <25 34 (62) 9 (64) 7 (70) 25 21 (38) 5 (36) 3 (30) Mean (SDb) Daily # cigarettes smoked 1.9 (4.5) 0.4 (1.4) 0.4 (1.3) 0.28 Daily # alcoholic beverages 0.3 (0.3) 0.2 (0.5) 0.5 (0.4) 0.33 Daily # caffeinated beverages 1.8 (1.5) 0.9 (0.9) 1.4 (1.2) 0.10 NOTE: Cigarette usage was imputed for 9 women, 9 for alcohol and 9 for caffeine consumption. Gravidity is missing for 2 women. Excludes 20 women who withdrew from study before an outcome. aTTP, denotes number of menstrual cycles at risk for pregnancy. bSD, denotes standard deviation. Table 2. Median serum concentration of polychlorinated biphenyl (PCBs) and 1,1-dichloro-2,2-bis(p-chlorophenyl)ethylene (DDE) concentrations by study outcome (n = 79). Serum Concentration (ng/g serum) Live Birth (n = 55) Median (min, max) Pregnancy Loss (n = 14) Median (min, max) Infertile (n = 10) Median (min, max) Total PCBs 5.26 (2.58, 14.51) 5.14 (3.89, 9.09) 4.62 (4.09, 11.08) Estrogenic PCBs 2.20 (0.07, 9.19) 2.16 (1.63, 4.52) 1.99 (0.63, 5.99) Anti-estrogenic PCBs 0.20 (<0.02, 0.68) 0.18 (0.03, 0.32) 0.22 (0.06, 0.35) Other PCBs 2.88 (1.58, 9.07) 2.83 (2.04, 4.68) 2.47 (2.23, 4.99) DDE 0.93 (<0.01, 3.37) 1.06 (0.41, 1.63) 0.80 (0.47, 3.59) Serum lipids (mg/dL) 558.35 (369.67, 881.49) 555.95 (324.20, 967.13) 537.74 (402.55, 713.80) Note: Cigarette usage was imputed for 9 women, 9 for alcohol and 9 for caffeine consumption. Gravidity is missing for 2 women. Excludes 20 women who withdrew from study before an outcome. serum) compared to those with a live birth (0.93 ng/g serum). Total PCBs, estrogenic PCBs, anti-estrogenic PCBs and DDE were not statistically significantly associated with the adjusted hazard of pregnancy loss (Table 3). However, the point estimates were greater than one for total and estrogenic PCBs and DDE and less than one for anti-estrogenic PCBs. Relative to the lowest tertile, the aHR for pregnancy loss among those in the highest DDE tertile was 1.45 (95% CI: 0.3, 5.70). The highest estro- 7 Copyright © 2011 SciRes. JEP  Persistent Organochlorine Exposure and Pregnancy Loss: A Prospective Cohort Study687 Table 3. Serum concentration of polychlorinated biphenyl (PCBs) and 1,1-dichloro-2,2-bis(p-chlorophenyl)ethylene (DDE) concentrations and hazard of pregnanc y loss (n = 69). Serum Concentration (ng/g serum) Unadjusted HR (95% CI) Adjusted HR (95% CI)a Total PCBs Low (1.62 - 5.02) 1.00 (referent) 1.00 (referent) Medium (5.03 - 5.71) 1.06 (0.28, 4.00) 0.98 (0.25, 3.82) High (5.72 - 12.68) 0.98 (0.26, 3.66) 1.20 (0.31, 4.67) Total PCBs (continuous) 1.04 (0.77, 1.50) 1.15 (0.84, 1.58) Estrogenic PCBs: Low (1.49 - 2.06) 1.00 (referent) 1.00 (referent) Med (2.07 - 2.28) 0.59 (0.16, 2.23) 0.60 (0.16, 2.31) High (2.29 - 4.53) 0.75 (0.21, 2.66) 0.86 (0.23, 3.11) Estrogenic PCBs (continuous) 1.61 (0.64, 4.02) 1.66 (0.68, 4.02) Anti-estrogenic PCBs: Low (0.02 - 0.16) 1.00 (referent) 1.00 (referent) Med (0.17 - 0.22) 0.70 (0.21, 2.35) 0.83 (0.24, 2.85) High (0.23 - 0.65) 0.48 (0.12, 1.97) 0.71 (0.16, 3.10) Anti-estrogenic PCBs (continuous) 0.03 (<0.01, 18.79) 0.10 (<0.01, 67.07) Other PCBs: Low (1.97 - 2.70) 1.00 (referent) 1.00 (referent) Med (2.71 - 3.11) 1.43 (0.35, 5.80) 1.61 (0.39, 6.72) High (3.12 - 9.07) 1.25 (0.30, 5.32) 1.70 (0.38, 7.49) Other PCBs (continuous) 0.99 (0.58, 1.70) 1.09 (0.66, 1.81) DDE Low (0.39 - 0.82) 1.00 (referent) 1.00 (referent) Med (0.83 - 1.14) 1.07 (0.28, 4.06) 1.08 (0.28, 4.21) High (1.15 - 3.60) 1.21 (0.32, 4.59) 1.45 (0.37, 5.70) DDE (continuous) 1.09 (0.38, 3.15) 1.43 (0.45, 4.52) NOTE: Estrogenic PCBs includes congeners 4_10, 5_8, 15_17, 18, 31, 44, 47, 48, 52, 70, 99, 101, 136, 153, 188; anti-estrogenic PCBs includes congeners 77_110, 105, 114, 126, 156_171, 169; and other includes PCB congeners 6, 7_9, 16_32, 19, 22, 24_27, 25, 28, 33, 40, 42, 45, 50, 55, 59, 60, 64, 66_95, 74, 81_87, 82, 94, 97, 118, 128, 129, 132, 134, 135, 138, 141, 147, 149, 151, 157_200, 163, 167, 170, 172, 174, 176, 177, 179, 180, 181, 183, 185, 187, 189, 190, 194, 195, 196_203, 205, 206. Analysis restricted to women becoming pregnant while under observation in the prospective cohort. Cox proportional hazards regression. aAdjusted for: age (24 - 30 versus 30 - 34) and mean alcohol consumption and cigarette smoking standardized to a 28-day menstrual cycle. genic PCB tertile was not positively associated with pregnancy loss when compared with the lowest estro- genic PCB tertile (aHR = 0.86, 95% CI: 0.23, 3.11). When continuous estrogenic, anti-estrogenic, and other PCBs and DDE were jointly included in the model, es- trogenic PCBs (aHR = 1.77, 95% CI: 0.34, 9.25) and DDE (aHR = 1.68, 95% CI: 0.50, 5.61) yielded positive point estimates and wide confidence intervals that in- cluded the null (Table 4). We conducted sensitivity analyses first restricting the models to women with com- plete exposure data (no imputations) and then substitut- ng log transformed PCB and DDE values for the raw i Copyright © 2011 SciRes. JEP  Persistent Organochlorine Exposure and Pregnancy Loss: A Prospective Cohort Study 688 Table 4. Hazard of pregnancy loss and serum concentration of polychlorinated biphenyl (PCBs) and 1,1-dichloro-2,2-bis (p-chlorophenyl)ethylene (DDE) analyzed jointly (n = 69). Serum Concentration (ng/g serum) Unadjusted HR (95% CI) Adjusted HR (95% CI)a Estrogenic PCBs 1.64 (0.29, 9.36) 1.77 (0.34, 9.25) Anti-estrogenic PCBs 0.02 (<0.01, 196.01) 0.09 (<0.01, 632.71) Other PCBs 0.96 (0.18, 5.09) 0.91 (0.19, 4.41) DDE 1.38 (0.44, 4.39) 1.68 (0.50, 5.61) NOTE: Estrogenic PCBs includes congeners 4_10, 5_8, 15_17, 18, 31, 44, 47, 48, 52, 70, 99, 101, 136, 153, 188; anti-estrogenic PCBs includes congeners 77_110, 105, 114, 126, 156_171, 169; and other includes PCB congeners 6, 7_9, 16_32, 19, 22, 24_27, 25, 28, 33, 40, 42, 45, 50, 55, 59, 60, 64, 66_95, 74, 81_87, 82, 94, 97, 118, 128, 129, 132, 134, 135, 138, 141, 147, 149, 151, 157_200, 163, 167, 170, 172, 174, 176, 177, 179, 180, 181, 183, 185, 187, 189, 190, 194, 195, 196_203, 205, 206. Analysis restricted to women becoming pregnant while under observation in the prospective cohort. Cox proportional hazards regression. aAdjusted for: age (24 - 30 versus 30 - 34) and mean alcohol consumption and cigarette smoking standardized to a 28-day menstrual cycle. measurements and observed similar results (data not shown). 4. Discussion Our prospective pregnancy study with preconception enrollment of women and a sensitive hCG biomarker of pregnancy did not find statistically significant associa- tions between DDE, total, estrogenic, and anti-estrogenic PCBs, and pregnancy loss. The point estimates for an- ti-estrogenic PCBs were less than one, possibly suggest- ing a different direction of effect, but the estimate was imprecise. One possible explanation for the suggestion of a protective effect on the hazard of pregnancy loss for anti-estrogenic PCBs may be attributed to the concept of competing risk. If an exposure reduces pregnancy likeli- hood, fewer losses would be expected, given that preg- -nancy is a necessary criterion for a loss. Anti-estrogenic PCB concentrations were associated with a reduction in fecundability or a longer time to pregnancy for this co- hort [25]. In this cohort, 6- and 12-month cumulative pregnancies were 76% and 94%, which are similar to the two other prospective pregnancy studies conducting 12 month follow-up of couples. Cumulative 6-and 12-cycle pregnancy rates for other prospective cohort studies fol- lowing women through 12 cycles ranged from 81% - 90% [36] and 92% - 95% [37]. Another explanation may be attributed to the labora- tory precision in measuring the anti-estrogenic PCB congeners or the absence of uniform criteria for grouping congeners with regard to biologic activity. The sugges- tion of opposing directions for our point estimates by congener grouping supports the need to more fully assess the mixture of compounds in relation to sensitive repro- ductive and developmental outcomes, particularly in pre- conception cohort studies with ample power for the de- tection of pregnancy losses. The only other prospective cohort study that utilized preconception enrollment of women, enabling the au- thors to identify incident pregnancy losses found a posi- tive association between pregnancy loss and DDT [18]. Specifically, 388 nulliparous Chinese women provided a blood specimen for the quantification of serum DDE and daily urine samples for up to one year for the detection of hCG pregnancy. An increased odds ratio (OR) for early pregnancy loss of 1.17 (95% CI: 1.05, 1.29) was associ- ated with a 10-ng/g increase in serum total DDT, and in a categorical analysis comparing the third tertile of expo- sure to the first, found an adjusted OR 2.12 (95% CI: 1.26, 3.57) [18]. Concentrations were notably higher among the Chinese women (median p,p’-DDE and total DDT of 26.24 ng/g and 27.9, respectively) than in our study (median DDE 0.97 ng/g), possibly reflecting the more recent use of DDT in China compared to the United States [38]. Increased odds of spontaneous abortion have been associated for DDE in a subset of the US Collabo- rative Pregnancy Cohort, which recruited already preg- nant women at median gestational age 21 weeks [14,39]. A small case control study of 30 Chinese factory workers also reported that p,p’-DDE was associated with a 1.13 (CI: 1.02, 1.26) increased odds of spontaneous pregnancy loss [13]. Lastly, support for an association between PCB and/or DDE exposure and pregnancy loss comes from several studies that relied upon retrospectively reported exposures or outcomes and often without added attention to the role of lactation history in mediating effects [40-42]. Women with pregnancy losses have less oppor- tunity to decrease their body burden of PCBs and DDE than women giving birth, especially if they opt to breast- fed. Retrospective exposures that rely on complex decay models for estimating exposures at some time in the past such as during pregnancy may be a source of potential exposure misclassification [43]. Our results are not in- consistent with the existing literature on DDE and are subject to limited power, though the direction of effect, particularly for DDE, signals a similar direction of effect as prior work. Copyright © 2011 SciRes. JEP  Persistent Organochlorine Exposure and Pregnancy Loss: A Prospective Cohort Study689 The mechanism of action by which DDE interferes with pregnancy maintenance is not known, but DDE isomers are believed to act similarly to estradiol [44,45] and, thereby, may interfere with endocrine function. Al- ternatively, DDE and PCBs have been demonstrated to induce cytochrome P450 hepatic enzymes, which could interfere with normal hormonal production necessary for pregnancy maintenance [46,47] or the metabolism of other xenobiotics, which may enhance or diminish hor- monal or biochemical processes [48,49]. Further, persis- tent organochlorine compounds may disrupt the placental cell sodium channel barrier and, thereby, affect proges- terone receptor binding [14]. 5. Conclusions We sought to assess a mixture of persistent organochlo- rine compounds in relation to impaired fecundity, par- ticularly the risk of pregnancy loss, to better model hu- man exposures by addressing biological mechanism of action. The use of daily diaries for ascertaining lifestyle exposures believed relevant for human fecundity is ad- vantageous, since women reported lifestyle exposures prior to knowledge of pregnancy outcome. We system- atically ascertained pregnancy via sensitive home preg- nancy test kits, and we know no a priori reason why test results would vary by exposure status. Our findings await replication from larger cohort studies with preconception enrollment and longitudinal data collection with the eventual expectation of filling critical data gaps regard- ing the impact of persistent compounds on sensitive markers of human reproduction and development. Our findings are not inconsistent with prior findings of an association between DDE and estrogenic PCBs and pregnancy loss. Though limited by a lack of power, our results underscore the value of efforts to measure chemi- cal mixtures and better approximate the biological mode of action. Further, due to preconceptional enrollment of women and the pregnancy testing protocol, there is very little possibility for missed pregnancy losses. 6. Acknowledgements This research was supported by the Intramural Research Program of the Eunice Kennedy Shriver National Insti- tute of Child Health and Human Development, National Institutes of Health. REFERENCES [1] J. M. Wood, “Dynamics of Human Reproduction: Biol- ogy, Biometry, Demography.” Aldine de Gruyter, New York, 1994. [2] C. Gini, “Premieres Recheres Sur la Fecondabilite de la Femme,” Proceedings of the International Mathematical Conference, Vol. 2, 1924, pp. 889-892. [3] A. J. Wilcox, C. R. Weinberg, J. F. O’Connor, D. D. Baird, J. P. Schlatterer, R. E. Canfield, et al., “Incidence of Early Loss of Pregnancy,” New England Journal of Medicine, Vol. 319, No. 4, 1988, pp. 189-194. doi:10.1056/NEJM198807283190401 [4] G. P. Daston, J. W. Gooch, W. J. Breslin, et al., “Envi- ronmental Estrogens and Reproductive Health: A Discus- sion of the Human and Environmental Data,” Reproduc- tive Toxicology, Vol. 11, No. 4, 1997, pp. 465-481. doi:10.1016/S0890-6238(97)00014-2 [5] E. Diamanti-Kandarakis, J. P. Bourguignon, L. C. Giudice, R. Hauser, G. S. Prins, A. M. Soto, et al., “En- docrine-Disrupting Chemicals: An Endocrine Society Sci- entific Statement,” Endocrine Reviews, Vol. 30, No. 4, 2009, pp. 293-342. doi:10.1210/er.2009-0002 [6] G. Toft, L. Hagmar, A. Giwercman and J. P. Bonde, “Epidemiological Evidence on Reproductive Effects of Persistent Organochlorines in Humans,” Reproductive Toxicology, Vol. 19, No. 1, 2004, pp. 5-26. doi:10.1016/j.reprotox.2004.05.006 [7] T. M. Crisp, E. D. Clegg, R. L. Cooper, W. P. Wood, D. G. Anderson, K. P. Baetcke, et al., “Environmental En- docrine Disruption: An Effects Assessment and Analy- sis,” Environ Health Perspect, Vol. 106, Supplement 1, 1998, pp. 11-56. [8] L. G. M. Buck, C. D. Lynch and M. A. Cooney, “Envi- ronmental Influences on Female Fecundity and Fertility,” Seminars in Reproductive Medicine, Vol. 24, No. 3, 2006, pp. 147-155. doi:10.1055/s-2006-944421 [9] P. Mendola, G. M. Buck, J. E. Vena, M. Zielezny and L. E. Sever, “Consumption of PCB-Contaminated Sport Fish and Risk of Spontaneous Fetal Death,” Environ Health Perspect, Vol. 103, No. 5, 1995, pp. 498-502. doi:10.1289/ehp.95103498 [10] A. Axmon, L. Rylander, U. Stromberg and L. Hagmar, “Miscarriages and Stillbirths in Women with a High In- take of Fish Contaminated with Persistent Organochlorine Compounds,” International Archives of Occupational and Environmental Health, Vol. 73, No. 3, 2000, pp. 204-208. doi:10.1007/s004200050028 [11] K. Hemminki, M. L. Niemi, I. Saloniemi, H. Vainio and E. Hemminki, “Spontaneous Abortions by Occupation and Social Class in Finland,” International Journal of Epidemiology, Vol. 9, No. 2, 1980, pp. 149-153. doi:10.1093/ije/9.2.149 [12] D. O. Carpenter, Y. Shen, T. Nguyen, L. Le and L. L. Lininger, “Incidence of Endocrine Disease among Resi- dents of New York Areas of Concern,” Environmental Health Perspectives, Vol. 109, Supplement 6, 2001, pp. 845-851. doi:10.2307/3454646 [13] S. A. Korrick, C. Chen, A. I. Damokosh, J. Ni, X. Liu, S. I. Cho, et al., “Association of DDT with Spontaneous Abortion: A Case-Control Study,” Annals of Epidemiol- ogy, Vol. 11, No. 7, 2001, pp. 491-496. doi:10.1016/S1047-2797(01)00239-3 [14] M. P. Longnecker, M. A. Klebanoff, D. B. Dunson, X. Copyright © 2011 SciRes. JEP  Persistent Organochlorine Exposure and Pregnancy Loss: A Prospective Cohort Study 690 Guo, Z. Chen, H. Zhou, et al., “Maternal Serum Level of the DDT Metabolite DDE in Relation to Fetal Loss in Previous Pregnancies,” Environmental Research, Vol. 97, No. 2, 2005, pp. 127-133. doi:10.1016/S0013-9351(03)00108-7 [15] A. M. Sweeney, M. R. Meyer, J. H. Aarons, J. L. Mills and R. E. LaPorte, “Evaluation of Methods for the Pro- spective Identification of Early Fetal Losses in Environ- mental Epidemiology Studies,” American Journal of Epidemiology, Vol. 127, No. 4, 1988, pp. 843-850. [16] R. E. Chapin, W. A. Robbins, L. A. Schieve, A. M. Sweeney, S. A. Tabacova and K. M. Tomashek, “Off to a Good Start: The Influence of Pre- and Periconceptional Exposures, Parental Fertility, and Nutrition on Children’s Health,” Environmental Health Perspectives, Vol. 112, No. 1, 2004, pp. 69-78. doi:10.1289/ehp.6261 [17] G. M. Buck, C. D. Lynch, J. B. Stanford, A. M. Sweeny, L. A. Schieve, J. C. Rockett, et al., “Prospective Preg- nancy Study Designs for Assessing Reproductive and Developmental Toxicants,” Environmental Health Per- spectives, Vol. 112, No. 1, 2004, pp. 79-86. doi:10.1289/ehp.6262 [18] S. A. Venners, S. Korrick, X. Xu, C. Chen, W. Guang, A. Huang, et al., “Preconception Serum DDT And Pregnancy Loss: A Prospective Study Using A Biomarker Of Preg- nancy,” American Journal of Epidemiology, Vol. 162, No. 8, 2005, pp. 709-716. doi:10.1093/aje/kwi275 [19] M. Sugiura-Ogasawara, Y. Ozaki, S. Sonta, T. Makino and K. Suzumori, “PCBs, Hexachlorobenzene and DDE Are Not Associated with Recurrent Miscarriage,” Ameri- can Journal of Epidemiology, Vol. 50, No. 6, 2003, pp. 485-489. [20] I. Gerhard, V. Daniel, S. Link, B. Monga and B. Runne- baum, “Chlorinated Hydrocarbons in Women with Re- peated Miscarriages,” Environmental Health Perspectives, Vol. 106, No. 10, 1998, pp. 675-681. doi:10.1289/ehp.98106675 [21] L. A. Cole, S. A. Khanlian, J. M. Sutton, S. Davies and W. F. Rayburn, “Accuracy of Home Pregnancy Tests at the Time of Missed Menses,” American Journal of Obstetrics and Gynecology, Vol. 190, No. 1, 2004, pp. 100-105. doi:10.1016/j.ajog.2003.08.043 [22] M. S. Bloom, L. G. M. Buck, E. F. Schisterman, A. Liu and P. J. Kostyniak, “Maternal Serum Polychlorinated Biphenyl Concentrations Across Critical Windows of Human Development,” Environmental Health Perspec- tives, Vol. 115, No. 9, 2007, pp. 1320-1324. doi:10.1289/ehp.10086 [23] H. B. Greizerstein, P. Gigliotti, J. Vena, J. Freudenheim and P. J. Kostyniak, “Standardization of a Method for the Routine Analysis of Polychlorinated Biphenyl Congeners and Selected Pesticides in Human Serum and Milk,” Journal of Analytical Toxicology, Vol. 21, No. 7, 1997, pp. 558-566. [24] P. S. Cooke, T. Sato and D. L. Buchanan, “Disruption of Steroid Hormone Signaling by PCBs,” In: L. W. Robert- son and L. G. Hansen, Eds., PCBs: Recent Advances in Environmental Toxicology and Health Effects, The Uni- versity Press of Kentucky, Lexington, 2001, pp. 257-263. [25] L. G. M. Buck, J. Dmochowski, C. Lynch, P. Kostyniak, B. M. McGuinness and J. E. Vena, “Polychlorinated Bi- phenyl Serum Concentrations, Lifestyle and Time-to- Pregnancy,” Human Reproduction, Vol. 24, No. 2, 2009, pp. 451-458. doi:10.1093/humrep/den373 [26] E. F. Schisterman, A. Vexler, B. W. Whitcomb and A. Liu, “The Limitations Due to Exposure Detection Limits for Regression Models,” American Journal of Epidemi- ology, Vol. 163, No. 4, 2006, pp. 374-383. doi:10.1093/aje/kwj039 [27] D. B. Richardson and A. Ciampi, “Effects of Exposure Measurement Error When an Exposure Variable Is Con- strained by a Lower Limit,” American Journal of Epide- miology, Vol. 157, No. 4, 2003, pp. 355-363. doi:10.1093/aje/kwf217 [28] E. F. Schisterman, B. W. Whitcomb, G. M. Louis and T. A. Louis, “Lipid Adjustment in the Analysis of Environ- mental Contaminants and Human Health Risks,” Environ Health Perspect, Vol. 113, No. 7, 2005, pp. 853-857. doi:10.1289/ehp.7640 [29] D. L. Phillips, J. L. Pirkle, V. W. Burse, J. T. Bernert, L. O. Henderson and L. L. Needham, “Chlorinated Hydro- carbon Levels in Human Serum: Effects of Fasting and Feeding,” Archives of Environmental Contamination and Toxicology, Vol. 18, No. 4, 1989, pp. 495-500. doi:10.1007/BF01055015 [30] S. D. Holladay and R. J. Smialowicz, “Development of the Murine and Human Immune System: Differential Ef- fects of Immunotoxicants Depend on Time of Exposure,” Environmental Health Perspectives, Vol. 108, No. S3, 2000, pp. 463-473. doi:10.2307/3454538 [31] G. J. van der Heijden, A. R. Donders, T. Stijnen and K. G. Moons, “Imputation of Missing Values Is Superior to Complete Case Analysis and the Missing-Indicator Method in Multivariable Diagnostic Research: A Clinical Example,” Journal of Clinical Epidemiology, Vol. 59, No. 10, 2006, pp. 1102-1109. doi:10.1016/j.jclinepi.2006.01.015 [32] K. G. Moons, R. A. Donders, T. Stijnen and F. E. Harrell, “Using the Outcome for Imputation of Missing Predictor Values Was Preferred,” Journal of Clinical Epidemiology, Vol. 59, No. 10, 2006, pp. 1092-1101. doi:10.1016/j.jclinepi.2006.01.009 [33] W. Vach and M. Blettner, “Biased Estimation of the Odds Ratio in Case-Control Studies Due to the Use of Ad Hoc Methods of Correcting for Missing Values for Con- founding Variables,” American Journal of Epidemiology, Vol. 134, No. 8, 1991, pp. 895-907. [34] P. P. Howards, E. F. Schisterman and P. J. Heagerty, “Potential Confounding by Exposure History and Prior Outcomes: An Example from Perinatal Epidemiology,” Epidemiology, Vol. 18, No. 5, 2007, pp. 544-551. doi:10.1097/EDE.0b013e31812001e6 [35] C. R. Weinberg, “Toward a Clearer Definition of Con- founding,” American Journal of Epidemiology, Vol. 137, Copyright © 2011 SciRes. JEP  Persistent Organochlorine Exposure and Pregnancy Loss: A Prospective Cohort Study Copyright © 2011 SciRes. JEP 691 No. 1, 1993, pp. 1-8. [36] C. Gnoth, D. Godehardt, E. Godehardt, P. Frank-Herr- mann and G. Freundl, “Time to Pregnancy: Results of the German Prospective Study and Impact on the Manage- ment of Infertility,” Human Reproduction, Vol. 18, No. 9, 2003, pp. 1959-1966. doi:10.1093/humrep/deg366 [37] X. Wang, C. Chen, L. Wang, D. Chen, W. Guang and J. French, “Conception, Early Pregnancy Loss, and Time to Clinical Pregnancy: A Population-Based Prospective Study,” Fertility and Sterility, Vol. 79, No. 3, 2003, pp. 577-584. doi:10.1016/S0015-0282(02)04694-0 [38] W. J. Rogan and A. Chen, “Health Risks and Benefits of Bis(4-Chlorophenyl)-1,1,1-Trichloroethane (DDT),” Lancet, Vol. 366, No. 9487, 2005, pp. 763-773. doi:10.1016/S0140-6736(05)67182-6 [39] A. Chen, M. L. Pennell, M. A. Klebanoff, W. J. Rogan and M. P. Longnecker, “Maternal Smoking during Preg- nancy in Relation to Child Overweight: Follow-up to Age 8 Years,” International Journal of Epidemiology, Vol. 35, No. 1, 2006, pp. 121-130. doi:10.1093/ije/dyi218 [40] L. E. Redding, M. D. Sohn, T. E. McKone, J. W. Chen, S. L. Wang, D. P. Hsieh, et al., “Population Physiologically Based Pharmacokinetic Modeling for the Human Lacta- tional Transfer of PCB-153 with Consideration of World- wide Human Biomonitoring Results,” Environmental Health Perspectives, Vol. 116, No. 12, 2008, pp. 1629- 1635. Perspectives, Vol. 116, No. 12, 2008, pp. 1629- 1635. doi:10.1289/ehp.11519 [41] H. R. Chao, S. L. Wang, C. C. Lee, H. Y. Yu, Y. K. Lu and O. Papke, “Level of Polychlorinated Dibenzo-P-Diox- ins, Dibenzofurans and Biphenyls (PCDD/Fs, Pcbs) in Human Milk and the Input to Infant Body Burden,” Food and Chemical Toxicology, Vol. 42, No. 8, 2004, pp. 1299-1308. doi:10.1016/j.fct.2004.03.008 [42] L. A. Gallenberg and M. J. Vodicnik, “Potential Mecha- nisms for Redistribution of Polychlorinated Biphenyls during Pregnancy and Lactation,” Xenobiotica, Vol. 17, No. 3, 1987, pp. 299-310. doi:10.3109/00498258709043940 [43] A. Axmon, A. M. Thulstrup, A. Rignell-Hydbom, H. S. Pedersen, V. Zvyezday, J. K. Ludwicki, et al., “Time to Pregnancy as a Function of Male and Female Serum Concentrations of 2,2'4,4'5,5'-Hexachlorobiphenyl (CB-153) and 1,1-Dichloro-2,2-Bis (P-Chlorophenyl)-Ethylene (p,p'- DDE),” Human Reproduction, Vol. 21, No. 3, 2006, pp. 657-665. doi:10.1093/humrep/dei397 [44] J. S. Ireland, V. R. Mukku, A. K. Robison and G. M. Stancel, “Stimulation of Uterine Deoxyribonucleic Acid Synthesis by 1,1,1-Trichloro-2-(p-Chlorophenyl)-2-(o- Chlorophenyl)ethane (o,p'-DDT),” Biochemical Pharma- cology, Vol. 29, No. 11, 1980, pp. 1469-1474. doi:10.1016/0006-2952(80)90596-1 [45] G. M. Stancel, J. S. Ireland, V. R. Mukku and A. K. Robi- son, “The Estrogenic Activity of DDT: In Vivo and in Vitro Induction of a Specific Estrogen Inducible Uterine Protein by o,p’-DDT,” Life Science, Vol. 27, No. 12, 1980, pp. 1111-1117. doi:10.1016/0024-3205(80)90037-5 [46] R. W. Nims, R. A. Lubet, S. D. Fox, P. E. Thomas, A. B. Reddy, T. A. Kocarek, et al., “Comparative Pharmaco- dynamics of CYP2B Induction by DDT, DDE, and DDD in Male Rat Liver and Cultured Rat Hepatocytes,” Jour- nal of Toxicology and Environmental Health, Part A, Vol. 53, No. 6, 1998, pp. 455-477. doi:10.1080/009841098159187 [47] R. W. Nims and R. A. Lubet, “Induction of Cytochrome P-450 in the Norway Rat, Rattus Norvegicus, Following Exposure to Potential Environmental Contaminants,” Journal of Toxicology and Environmental Health, Vol. 46, No. 3, 1995, pp. 271-292. doi:10.1080/15287399509532035 [48] M. S. Petersen, J. Halling, P. Damkier, N. Flemming, P. Grandjean, P. Weihe, et al., “Polychlorinated Biphenyl (PCB) Induction of CYP3A4 Enzyme Activity in Healthy Faroese Adults,” Toxicology and Applied Pharmacology, Vol. 224, No. 2, 2007, pp. 202-206. doi:10.1016/j.taap.2007.07.002 [49] F. P. Guengerich, D. H. Kim and M. Iwasaki, “Role of human cytochrome P-450 IIE1 in the oxidation of many low molecular weight cancer suspects,” Chemical Re- search in Toxicology, Vol. 4, No. 2, 1991, pp. 168-179. doi:10.1021/tx00020a008
|