International Journal of Clinical Medicine
Vol.4 No.1(2013), Article ID:26918,3 pages DOI:10.4236/ijcm.2013.41007
Hodgkin’s Lymphoma Presenting as Chest Pain*
![]()
Department of Internal Medicine, Catholic University of Rome, Rome, Italy.
Email: antonio.mirijello@gmail.com
Received November 20th, 2012; revised December 28th, 2012; accepted January 14th, 2013
Keywords: Chest Pain; Chest X-Ray
ABSTRACT
We report the case of a Hodgkin’s lymphoma presenting as chest pain due to the presence of multiple lymphoadenopathies of the superior mediastinum and a poly-lobated mass in the middle lobe of the right lung. Diagnostic approach and differential diagnosis are discussed.
1. Introduction
Hodgkin lymphoma (HL) is one of the most frequent lymphomas in the Western world. This lymphoid malignancy involves peripheral lymph nodes and can also affect organs such as liver, lung, and bone marrow [1]. Hodgkin’s lymphoma typical presentation consists in painless lymphadenopathies, frequently cervical or supraclavicular. A mediastinal mass can be found in more than 50% of patients, which can be asymptomatic or can present as dyspnoea, cough, or obstruction of the superior vena cava [2-3].
Chest pain is a common symptom in Internal Medicine, being the manifestation of a variety of diseases, ranging from functional, but disabling disorders, to life-threatening conditions. The differential diagnosis represents a challenge for the physician since it should consider a wide spectrum of causes, such as chest wall, cardiac, vascular, pulmonary, gastrointestinal and psychogenic aetiologies [4]. Data from literature highlight that chest pain aetiologies vary according to the population studied. In particular, life-threatening diseases are more common among emergency department patients, while benign causes are more frequent in primary care settings [5].
Thus, the physician’s clinical eye should understand chest pain cause by collecting a detailed history (e.g. pain description, associated symptoms, radiation, factors increasing or decreasing pain) and performing a complete physical examination. Moreover, the evaluation of disease’s risk factors can help in the diagnostic process. Electrocardiogram (ECG) and chest X-ray are diagnostic tests that should always be performed to support clinical hypotheses and to proceed with differential diagnosis.
Here we report the case of a young woman complaining of chest pain, being an atypical presentation of Hodgkin’s lymphoma. A detailed clinical history and a complete physical examination led us to perform a chest Xray that revealed the extra-cardiac cause of chest pain.
2. Case Report
A 27-year-old woman was referred to our Internal Medicine outpatients unit because of a 10-day history of chest pain. Pain was felt as a continuous anterior mid-chest pressure radiating to the right side of chest wall and to the jugulum. Physical activity did not increase the pain. The patient was also complaining of mild fatigue and moderate shortness of breath. She denied palpitations, fever, cough, sputum, or similar episodes in the past. She had been in good health prior to the occurrence of this symptom and had no limitation in effort tolerance. Previous medical history was unremarkable. She denied any family history of heart disease or cancer. She worked as reporter, and had smoked 10 cigarettes/day over the past 10 years. She denied use of alcohol or of any drugs.
At physical examination the patient appeared comfortable and not in pain or respiratory distress. She was neither icteric nor pale. Her blood pressure was 120/80 mmHg, pulse was 88 beats/min, respiratory rate was 15 breaths/min and she had a temperature of 37.0˚C.
Cardiac examination showed a regular S1 and S2 without murmurs and ECG was normal. Thoracic examination was within normal limits. The abdomen was soft and non-tender, with normal bowel sounds and no hepatosplenomegaly. Genitourinary, cutaneous, and neurologic examinations were normal, as well as the examination of her arms and legs.
The examination of neck region showed the presence, in both supraclavicular spaces, of several rubbery non-tender enlarged lymph-nodes which, at ultrasound evaluation, were round-shaped, hypoechoic and partially conglobated (30 mm of maximum diameter). On the basis of these findings, a chest X-ray was performed (Figure 1) showing multiple lyphoadenopathy of the superior mediastinum and a poly-lobated mass in the middle lobe of the right lung (5.5 cm size).
The patient underwent surgical excision of a supraclavicular lymph-node that, at pathological examination, was diagnostic for nodular sclerosis HL. The diagnostic work-up included a bone marrow biopsy showing no bone marrow involvement and a PET-CT scan (Figure 2) which showed multiple, partially conglobated lymphoadenopathies located in the anterior mediastinum (8.7 cm size), in the supraclavicular fossae, and in the right pulmonary hilum, with intraparenchimal peribronchial extension. According with the diagnosis of a stage IIA HL, ABVD chemotherapy plus sequential radiotherapy was started.
Patient experienced a rapid improvement of chest pain, achieving a complete remission of lymphoma after treatment. A chest X-ray at 1 year from the diagnosis shows normal findings (Figure 3).
3. Discussion
The present case describes the diagnostic approach to a young patient referred to our Internal Medicine outpatients unit because of chest pain. Although from an “a posteriori” point of view chest pain could be a symptom referred by HL patients with mediastinal involvement, from an “a priori” point of view HL represents an atypical cause of chest pain.
Considering young age, good general conditions (patient was appearing comfortable at medical visit), and
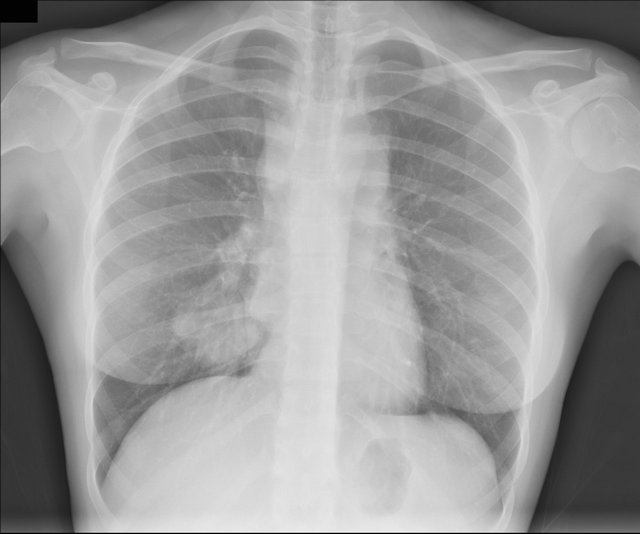
Figure 1. Chest X-ray findings: multiple lymphoadenopathies of the superior mediastinum and a poly-lobated mass in the middle lobe of the right lung (5.5 cm).
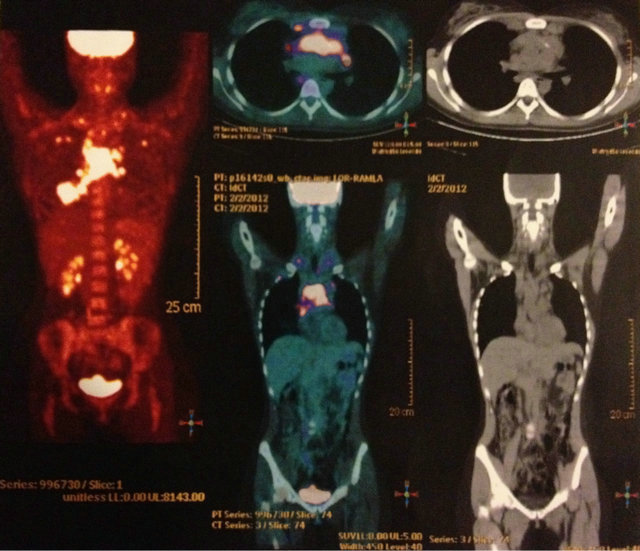
Figure 2. PET-CT scan findings: multiple, partially conglobated lympho-adenopathies located in the anterior mediastinum (8.7 cm), in the supraclavicular fossae, and in the right pulmonary hilum, with intraparenchimal extension.

Figure 3. Normal chest X-ray findings after ABVD treatment.
long duration of chest pain (10 days), cardiac ischemia and life-threatening diseases (i.e. pulmonary embolism, tension pneumothorax) were unlikely. The absence of any relation with physical activity was not consistent with the hypothesis of pericarditis, cardiac ischemia or pleuritis. Moreover, the absence of fever, cough and sputum was not meeting clinical criteria of pneumonia. Considering the normality of thoracic clinical examination, a chest wall cause (i.e. costochondritis, herpes zoster, rib fracture, sterno-clavicular arthritis) was unlikely. A hypothesis of gastro-oesophageal reflux disease or of cholelithiasis was not likely since the pain was continuous, not related to meals and it was not described as epigastric pain. Moreover, patient was calm, non-anxious and this was in contrast with a diagnosis of psychiatric cause of chest pain.
In contrast, the 2nd - 3rd decade represents the peak of incidence of HL. Basing on the description of the symptom (“continuous anterior mid-chest pressure radiating to the right side of chest wall and to the jugulum”) and on the presence of bilateral supraclavicular enlarged lymph-nodes, the hypothesis of a mediastinal mass was formulated and chest X-ray was performed. In the present case, chest pain was due to the presence of multiple lymphoadenopathies of the superior mediastinum and of a poly-lobated mass in the middle lobe of the right lung (Figure 1).
According to literature, intrathoracic involvement is commonly seen in the nodular sclerosis subtype of HL. Approximately 50% of HL patients have mediastinal and/or hilar lymphadenopathy with or without lung parenchymal lesions [6]. Interestingly, PET-CT findings (Figure 2) were strictly comparable with standard radiology findings.
4. Conclusion
Chest pain is one of the most common symptoms in Internal Medicine and, when it manifests as mid-chest pressure, a cardiac origin is usually feared. However an extra-cardiac origin should be considered and evaluated in all patients. In young patients, in whom cardiac ischemia is unlikely, pericarditis and esophagitis are preferentially investigated. A simple chest X-ray may help to orientate the diagnosis [7] and to explore mediastinal abnormalities.
5. Consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
REFERENCES
- R. Küppers, A. Engert and M. Hansmann, “Hodgkin Lymphoma,” Journal of Clinical Investigation, Vol. 122, No. 10, 2012, pp. 3439-3447. doi:10.1172/JCI61245
- P. M. Mauch, L. A. Kalish, M. Kadin, C. N. Coleman, R. Osteen and S. Hellman, “Patterns of Presentation of Hodgkin Disease. Implications for Etiology and Pathogenesis,” Cancer, Vol. 71, No. 6, 1993, pp. 2062-2071. doi:10.1002/1097-0142(19930315)71:6<2062::AID-CNCR2820710622>3.0.CO;2-0
- W. Townsend and D. Linch, “Hodgkin’s Lymphoma in Adults,” Lancet, Vol. 380, No. 9844, 2012, pp. 836-847. doi:10.1016/S0140-6736(12)60035-X
- M. S. Klinkman, D. Stevens and D. W. Gorenflo, “Episodes of Care for Chest Pain: A Preliminary Report from MIRNET. Michigan Research Network,” The Journal of Family Practice, Vol. 38, No. 4, 1994, pp. 345-352.
- F. Buntinx, D. Knockaert, R. Bruyninckx, et al., “Chest Pain in General Practice or in the Hospital Emergency Department: Is It the Same?” Family Practice, Vol. 18, No. 6, 2001, pp. 586. doi:10.1093/fampra/18.6.586
- S. Diederich, T. M. Link, H. Zuhlsdorf, E. Steinmeyer, D. Wormanns and W. Heindel, “Pulmonary Manifestations of Hodgkin’s Disease: Radiographic and CT Findings,” European Radiology, Vol. 11, No. 11, 2001, pp. 2295- 2305. doi:10.1007/s003300100866
- S. Raoof, D. Feigin, A. Sung, S. Raoof, L. Irugulpati and E. C. Rosenow, 3rd. “Interpretation of Plain Chest Roentgenogram,” Chest, Vol. 141, No. 2, 2012, pp. 545-558. doi:10.1378/chest.10-1302
NOTES
*Conflict of interest: All Authors declare no conflict of interest.