Open Journal of Therapy and Rehabilitation
Vol.2 No.1(2014), Article ID:42924,5 pages DOI:10.4236/ojtr.2014.21007
Validation of VO2Peak and performance using a SciFit™ Arm Ergometer
![]()
1Department of Health and Human Performance, The University of Findlay, Findlay, USA
2Department of Health & Physical Education, Western Oregon University, Monmouth, USA; *Corresponding Author: armstroj@wou.edu
3Applied Physiology Laboratory, Eastern Michigan University, Ypsilanti, USA
Copyright © 2014 James A. Yaggie et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. In accordance of the Creative Commons Attribution License all Copyrights © 2014 are reserved for SCIRP and the owner of the intellectual property James A. Yaggie et al. All Copyright © 2014 are guarded by law and by SCIRP as a guardian.
Received 20 December 2013; revised 22 January 2014; accepted 31 January 2014
KEYWORDS
Reliability; Validity; Upper Body Ergometry; Swimmers
ABSTRACT
For individuals with lower extremity injury or disability, upper body exercise provides a mechanism of functional mobility training, cardiovascular fitness, as well as a means for clinical fitness assessment. However, the validity of fitness assessment relies on the efficacy of diagnostic tools and measures in order to provide meaningful data to clinicians. The purpose of this investigation was to determine if the SciFit™ Pro II Arm Ergometer, a widely available upper body ergometer (UBE), is a reliable device for the determination of VO2peak in fit able-bodied swimmers. Eight trained male swimmers (28 ± 9 yrs) performed two incremental protocols (VO2peak) consisting of a 4-min warm-up at 15 W followed by 2 min at 50 W and progressing 10 W every 2 min until volitional exhaustion. There was a linear relationship between workload and VO2 in all trials (R = 0.96; p ≤ 0.01) while Cronbach’s alpha for test-retest reliability for VO2 was 0.98. In conclusion, the UBE is an accurate and reliable device for determination of VO2peak in trained swimmers, and further may be a viable alternative training method for the injured athlete.
1. INTRODUCTION
Upper body exercise is an important factor in the training and exercise prescription of various populations; therefore, it is important that researchers, clinical practitioners and coaches are able to properly quantify performance, as well as provide a means for accurate, consistent testing. Arm ergometry provides clinicians with a reliable tool to measure metabolic variation in a wide range of clinical populations ranging from those with disability to elite athletes who primarily utilize upper body musculature for their given activity (e.g., swimmers). Further, arm ergometry may provide swimmers and other athletes with a means of training while injured or unable to perform swim activities.
In swimming, the majority of events are 200 meters, or less, and at the competitive levels are typically performed at a duration of 2 minutes or less [1]. Price and Campbell [2] demonstrated that higher crank rates (above 70 RPM) elicit higher oxygen consumption and delayed neuromuscular fatigue. Price and Campbell [2] also hypothesized that a higher crank rate would avoid high muscular tension that exceeds perfusion pressure and impairs oxygen delivery to the tissues. Therefore, in order to train appropriately, swimmers must perform ergometry bouts at higher speeds in order to gain benefit of available anaerobic energy systems.
The need for equipment that provides effective training and workload for athletes continues to be a prevalent issue for the sport and fitness industry. The purpose of this study is to determine if the Pro II Arm Ergometer (SciFit, OK) is an accurate and reliable device for the determination of cardiovascular capacity in trained swimmers and the possible application to the general/clinical population. All standard paper components have been specified for three reasons: 1) ease of use when formatting individual papers, 2) automatic compliance to electronic requirements that facilitate the concurrent or later production of electronic products, and 3) conformity of style throughout a journal paper. Margins, column widths, line spacing, and type styles are built-in; examples of the type styles are provided throughout this document and are identified in italic type, within parentheses, following the example. Some components, such as multi-leveled equations, graphics, and tables are not prescribed, although the various table text styles are provided. The formatter will need to create these components, incorporating the applicable criteria that follow.
2. METHOD
Eight trained male swimmers (mean = 28 ± 9 y; mean body mass = 81.0 ± 8.6 kg) volunteered to participate in this study. Training was not regulated, but subjects were required to provide detailed training logs for the duration of the study and were instructed to limit training to only mild-moderate exercise the day before testing. Subjects also refrained from alcohol consumption 24 hours prior to testing and caffeine the day of testing, as well as followed similar eating (including no eating less than 2 hours prior to testing) and rest patterns leading up to test days so these variables would not become confounding factors on the test results. The experimental protocol was described and practiced through a familiarization trial. Subjects completed health history and informed consent forms before testing; and the College of Health and Human Services Human Subjects Review Board at Eastern Michigan University approved all procedures. Subjects completed two separate trials no less than three days apart.
Miller [3] has shown that an angle greater than 0˚ in the elbow may have an adverse effect on VO2peak determination during upper body ergometry. Therefore, anthropometric data were recorded during the first testing session, and the seat height of the arm ergometer (Pro II Arm Ergometer; SciFit, OK) was adjusted such that the shoulders were parallel with the hub of the arm crank and the distance was adjusted to allow full arm extension when the pedal was at its most distal position, and all seat positions were recorded to ensure consistency on the subsequent tests. Once comfortably positioned at the ergometer, subjects were fitted with a face mask covering the mouth and nose to collect expired gasses for breath-by-breath analysis, (Jaeger Oxycon, Sensor Medics, Yorba Linda, CA), as well as a heart rate monitor (Polar Accurex, Polar Electro, Finland). For testing purposes, subjects were instructed to maintain a comfortable, yet steady, crank rate within 70 - 100 rpm. During the second test, the previous crank rate cadence was maintained to ensure consistency.
The testing protocol consisted of a four-minute warmup at 15 Watts (W), followed by a ramp protocol to volitional fatigue. The ramp workload began at 50 W and was increased 10 W every two minutes. Subjects were verbally encouraged throughout the test to extend the duration and ensure that peak oxygen consumption was achieved. Upon completion of the test, subjects were allowed to cool down at a light workload and an unregulated crank rate.
Pearson’s product correlations (α = 0.05) were calculated for the relationships between VO2 and workload. Repeated measures ANOVA (α = 0.05) was performed and reliability was determined for peak power (Powerpeak), absolute VO2peak ( ), relative VO2peak (
), relative VO2peak ( ), respiratory exchange ratio (RER), expiratory volume (VE), and peak heart rate (HRpeak) using Cronbach’s alpha. Linear, quadratic and cubic regressions were attempted for prediction of VO2 for each stage (α = 0.05). All statistical calculations were performed using SPSS 21.0 (IBM, New York).
), respiratory exchange ratio (RER), expiratory volume (VE), and peak heart rate (HRpeak) using Cronbach’s alpha. Linear, quadratic and cubic regressions were attempted for prediction of VO2 for each stage (α = 0.05). All statistical calculations were performed using SPSS 21.0 (IBM, New York).
3. RESULTS
3.1. Test-Retest Reliability
The results of the test (T1) and re-test (T2) values for Powerpeak,  ,
,  , RER, VE, and HRpeak are shown in Table 1. Powerpeak, VO2peak (both relative and absolute), and VE all showed an increased response between subjects from T1 to T2. None of these increases, however, were statistically significant (p < 0.01). Figure 1 depicts the estimated marginal means of
, RER, VE, and HRpeak are shown in Table 1. Powerpeak, VO2peak (both relative and absolute), and VE all showed an increased response between subjects from T1 to T2. None of these increases, however, were statistically significant (p < 0.01). Figure 1 depicts the estimated marginal means of  from T1 to T2 across workloads (WL).
from T1 to T2 across workloads (WL).
There was a linear relationship between WL and  at each stage for both trials (r2 = 0.922; p ≤ 0.01) while Cronbach’s alpha for test-retest reliability for
at each stage for both trials (r2 = 0.922; p ≤ 0.01) while Cronbach’s alpha for test-retest reliability for  was 0.98. Mean VO2 did not differ at any given workload between T1 and T2 (Figure 1). It should be noted that maximal WL varied between subjects. Figure 1 depicts WL data that were mutually attained by all subjects (60, 80, 100 & 120 W).
was 0.98. Mean VO2 did not differ at any given workload between T1 and T2 (Figure 1). It should be noted that maximal WL varied between subjects. Figure 1 depicts WL data that were mutually attained by all subjects (60, 80, 100 & 120 W).
3.2. Correlations
Strong positive correlations were found between  and WL between T1 and T2 (r > 0.95, p ≤ 0.001) (Table 2).
and WL between T1 and T2 (r > 0.95, p ≤ 0.001) (Table 2).
3.3. Regressions
Results of the regression curve fit of  versus WL may be viewed in Figure 2 (all data are included). Linear, quadratic and cubic regressions were attempted for prediction of VO2 for each stage. Linear regression was significant (p < 0.001; F = 1927.73; R = 0.96).
versus WL may be viewed in Figure 2 (all data are included). Linear, quadratic and cubic regressions were attempted for prediction of VO2 for each stage. Linear regression was significant (p < 0.001; F = 1927.73; R = 0.96).
4. DISCUSSION
VO2 increased linearly with workload during both trials indicating a direct correlation between the two values.
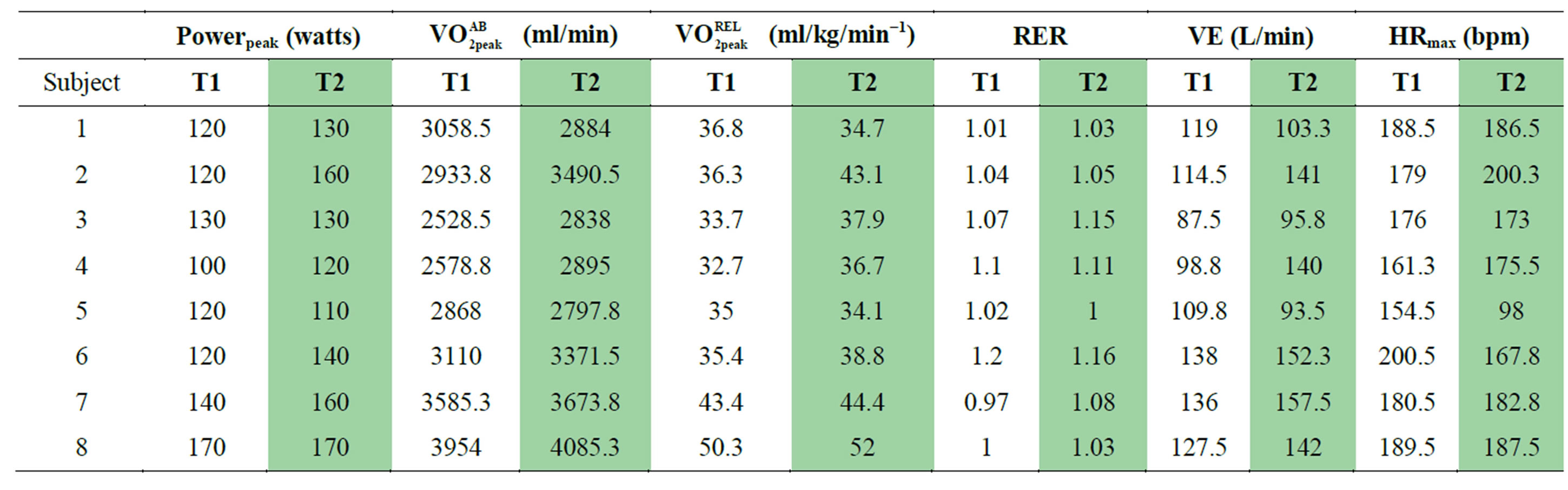
Table 1. Peak values of test (T1) and retest (T2) trials.

Table 2. Pearson’s r correlation matrix for Workload (WL) and Relative VO2 ( ) for test (T1) and retest (T2) trials. *indicates a significant correlation at the 0.01 level.
) for test (T1) and retest (T2) trials. *indicates a significant correlation at the 0.01 level.
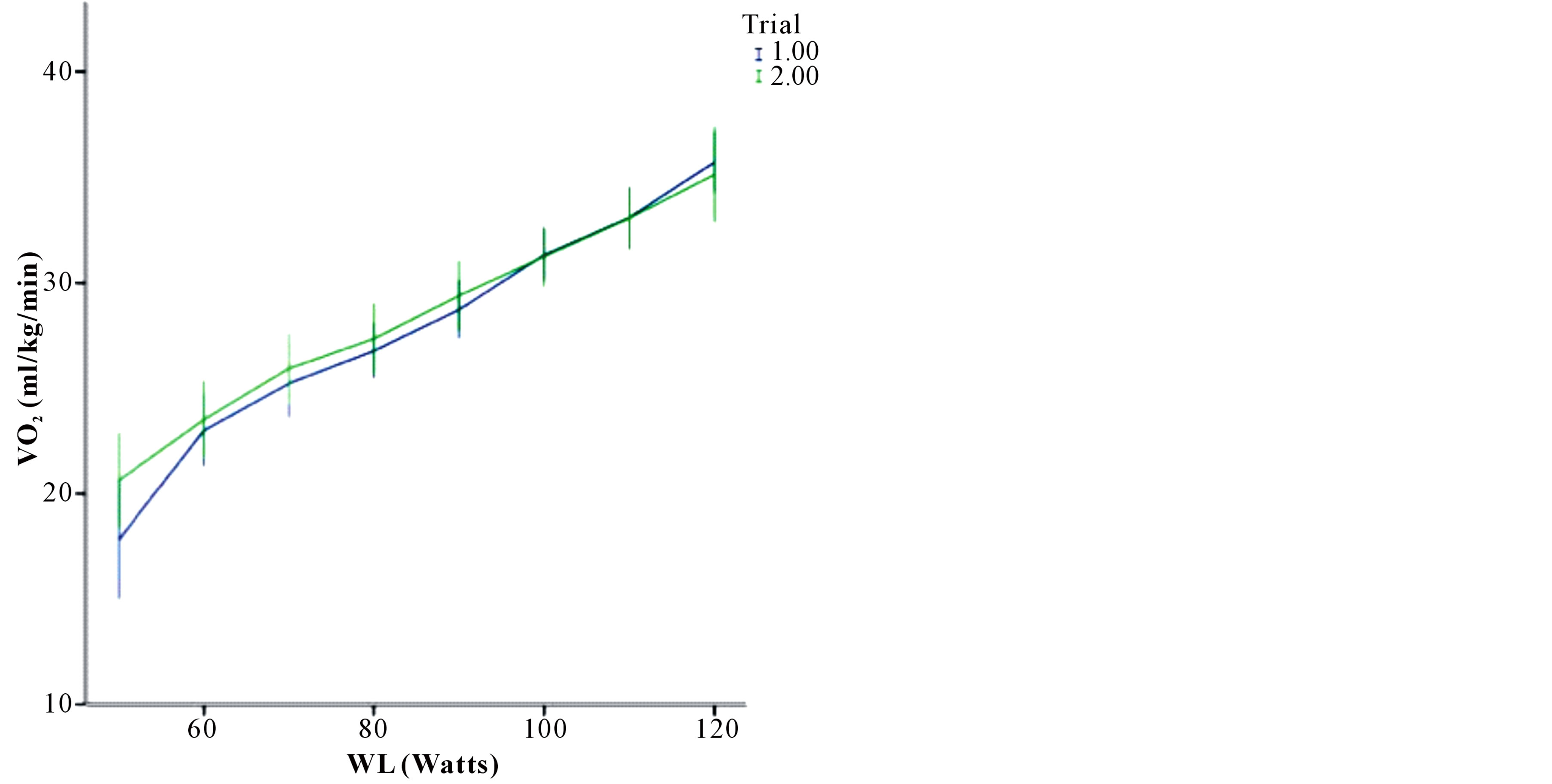
Figure 1. Estimated marginal means (±SD) of  between trials across WL.
between trials across WL.
Thus, as workload was increased at each progressive stage, oxygen consumption also increased in a linear fashion to meet the demand until subjects reached their peak. Although the ergometer trials were consistent, some subjects complained of mild to severe hand discomfort during the course of the ergometer trials. This discomfort may have influenced the ability of subjects to
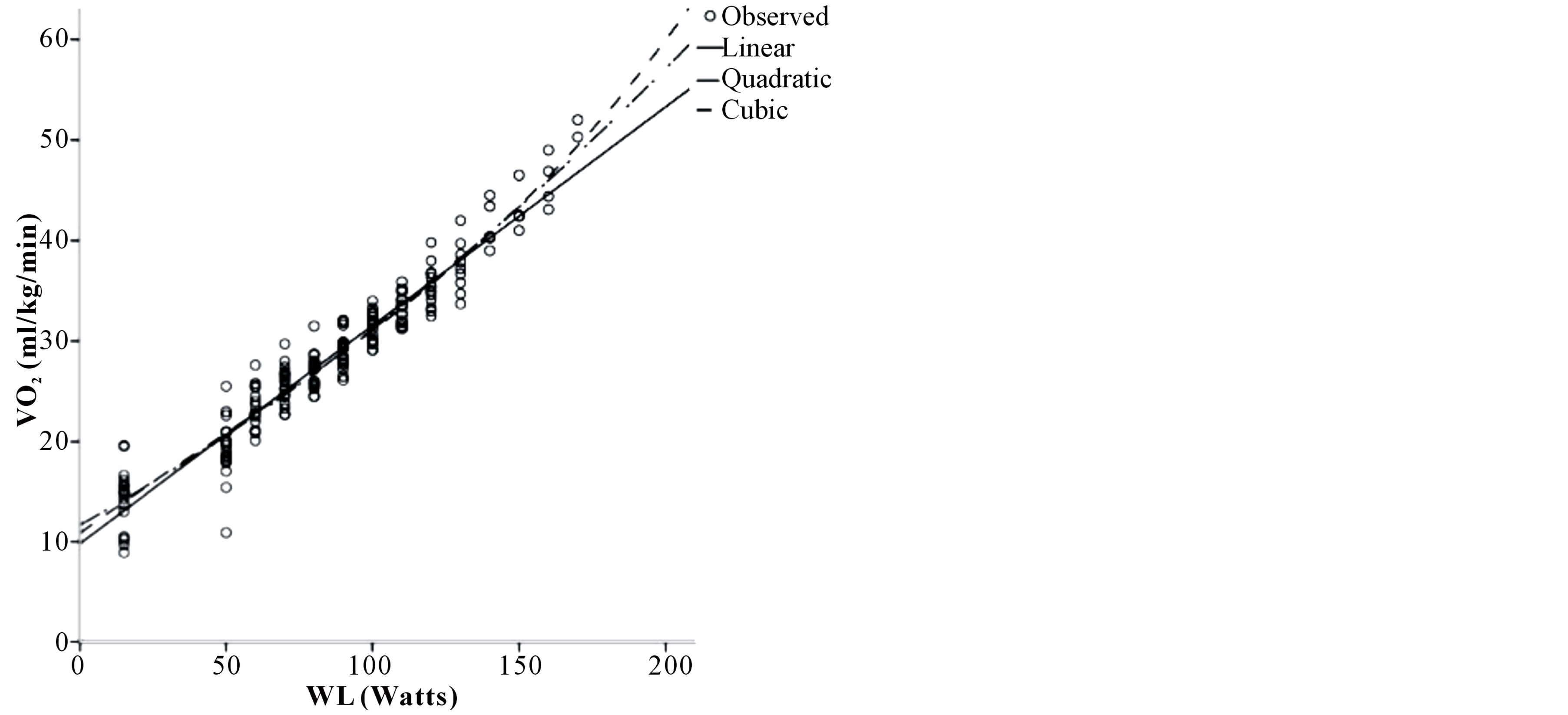
Figure 2. Regressions of  vs. WL.
vs. WL.
continue the test to a true VO2peak. Hooker and Wells [4] have shown, however, that although hand grasping during arm crank exercise increases subjects RPE, there is no difference in physiological parameters. The current findings are consistent with the work done by Price and Campbell [3] in that arm ergometry can provide accurate and consistent VO2peak measurements.
The consistent oxygen consumption at each workload between trials implies that the results of this study were reproducible and provided an accurate way to determine VO2peak as well as mean O2 consumption at each individual stage of testing. Although not statistically significant, shown trends for increased mean and maximal WL and VO2 by subject and by trial may be indicative of a learning effect, even in specifically trained athletes. Thus, familiarization trials may be warranted when using the UBE in intervention studies to assure that test-retest comparisons are most accurate.
This validation of the SciFit™ Arm Ergometer permits the future application of this device to evaluating cardiovascular performance and training outcomes in swimmers. These data may also serve additional utility for the treatment of individuals with a wide range of ability levels. The relationship between performance time and VO2peak determined on the UBE provides evidence of its value as a training device for all populations. Given the availability and accessibility of the device, it appears to be an appropriate diagnostic and training tool for clinics, medical fitness settings and other facilities that serve the able-bodied and disabled populations. From these data, further research may be conducted to modify the protocol based on functional ability and needs of the disabled client.
Only a small portion of the population with physically disabling conditions participates in recreation, leisure and training activities [5]. This may due to implications inherent to one’s condition or to a lack of access to appropriate fitness equipment, facilities and accommodating community programs. It is critical that barriers to activity be eliminated in order to provide individuals, regardless of injury or impairment status, access to training activities to improve fitness goals and functional ability. The literature indicates that the incidence of coronary artery disease in the spinal cord injured population is at least as high as the general population [6-8] and therefore effective assessment of cardiovascular function in this population is necessary in order to quantify cardiovascular risk and health status.
General cardiovascular responses in the spinal cord injured population are typically diminished, when compared to the able-bodied population. More specifically, functional capacity and VO2peak measures are significantly affected following spinal cord injury, but may be modified through training. Functional increases in VO2peak through aerobic work have shown to reduce cardiac risk [9], and also exhibit a reduction in reported strain in performing activities of daily living in the spinal cord injured population [10].
The development of valid cardiovascular assessment protocols for special populations can be a long and arduous undertaking. Initially, however, typical responses of cardiovascular work should be assessed in the ablebodied population to quantify to the repeatability and predictability of a measure’s functional characteristics. It has been documented that untrained able-bodied individuals exhibit a learning effect when performing measured exercise bouts [10,11]. The effects of learning are typically diminished through the use familiarization trials in untrained individuals. Trained participants, on the other hand, exhibit movement characteristics that tend to be more consistent and repeatable in successive trial [10]. Therefore, the use of trained athletes, with particular focus on those that perform upper extremity work, may provide a means of optimal measure in determining the effectiveness and validity of upper extremity ergometry, measures and protocols. From this, further development of submaximal protocols may be adapted to meet the needs of disabled populations.
5. CONCLUSION
Based on the results of this study it can be concluded that the SciFit Pro II Arm Ergometer is an accurate means of exercise testing. This machine elicited consistent metabolic responses between subjects on multiple occasions for both maximal and submaximal bouts. It is, however, important to take into consideration the possibility of training affects on these machines even in specifically trained populations. It is necessary to have all subjects of any study perform familiarization trials to ensure that measured values are in fact peak values and that all improvements in performance are due to physiological changes. These data may also be applied to development of more specific training and assessment protocols for individual with a range of ability levels.
REFERENCES
- Troup, J.P. and Trappe, T.A. (1994) Applications of research in swimming. In: Miyashita, M., Mutoh, Y. and Richardson, A.B., Eds., Medicine and Science in Aquatic Sport, Karger, Basel, 155-675.
- Price, M.J. and Campbell, I.G. (1997) Determination of peak oxygen consumption during upper body exercise. Ergonomics, 40, 491-499. http://dx.doi.org/10.1080/001401397188116
- Miller, T.L., Mattacola, C.G. and Santiago, M.C. (2004) Influence of varied, controlled distances from the arm crank axis on peak physiological responses during arm crank ergometry. Journal of Exercise Physiology Online, 7, 61-67.
- Hooker, S.P. and Wells, C.L. (1991) Physiologic responses to arm crank exercise with and without hand grasping. Clinical Kinesiology, 45, 3-8.
- Ferris, B.F. (1987) Reflections on the physical activity of patterns of disabled Canadians. Journal of Leisurability, 14, 18-23.
- Bauman, W.A., Spungen, A.M., Raza, M., et al. (1992) Coronary artery disease: Metabolic risk factors and latent disease in individuals with paraplegia. Mt Sinai Journal of Medicine, 59, 163-168.
- Yekutiel, M., Brooks, M.E., Ohry, A., Yarom, J. and Carel, R. (1989) The prevalence of hypertension, ischaemic heart disease and diabetes in traumatic spinal cord injured patients and amputees. Paraplegia, 27, 58-62. http://dx.doi.org/10.1038/sc.1989.9
- Dearwater, S.R., Laporte, R.E., Robertson, R.J., Brenes, G., Adams, L.L. and Becker, D. (1986) Activity in the spinal-cord injured patient: An epidemiologic analysis of metabolic parameters. Medicine and Science in Sports and Exercise, 18, 541-544. http://dx.doi.org/10.1249/00005768-198610000-00008
- Jansen, T.W., Van Oers, C.A., Rozendaal, E.P., Willemsen, E.M., Hollander, A.P. and Van der Woude, L.H. (1996) Changes in physical strain and physical capacity in men with spinal cord injuries. Medicine and Science in Sports and Exercise, 28, 551-559.
- Laursen, P.B., Shing, C.M. and Jenkins, D.G. (2003) Reproducibility of a laboratory-based 40-km cycle time-trial on a stationary wind-trainer in highly trained cyclists. International Journal of Sports Medicine, 24, 481-485. http://dx.doi.org/10.1055/s-2003-42012
- Lavcanska, V., Taylor N.F. and Schache, A.G. (2005) Familiarization to treadmill running in young unimpaired adults. Human Movement Science, 24, 544-557.