Open Journal of Obstetrics and Gynecology
Vol. 2 No. 1 (2012) , Article ID: 18350 , 2 pages DOI:10.4236/ojog.2012.21007
Natural course of ovarian torsion after untwisting: A case report with radiographic imaging
![]()
Department of Obstetrics and Gynecology, Maimonides Medical Center, New York, USA
Email: *Dmitry.Fridman@gmail.com
Received 26 January 2012; revised 23 February 2012; accepted 10 March 2012
Keywords: adnexal torsion; radiographic imaging
ABSTRACT
Background: Radiographic studies largely contribute to prompt diagnosis of ovarian torsion, though postoperative changes are not described and might contribute to unnecessary intervention. Case: We report a case of ovarian torsion diagnosed based on clinical presentation and radiographic findings. The detorsion was successfully performed through laparosopic access. Subsequently patient presented for elective ultrasonography and MRI which diagnosed multicystic ovarian mass, attributed to hematoma which resolved spontaneously with no intervention in 3 weeks. Conclusion: Ovarian changes after detorsion consistent with development of hematoma may be benign and resolve spontaneously.
1. INTRODUCTION
Untwisting the torsed adnexa is a safe and efficient method of treating this condition and preserving the ovarian tissue [1,2]. A case report describing second look laparoscopy 36 hours after untwisting [3] describes normal looking ovary. Similar results were shown by Kamprath S. et al., 1998 [4] and Li Y.K. et al., 2005 [5], who confirmed viability with color-Doppler study and second look laparoscopy. Radiographic studies largely contribute to diagnosis and management of ovarian torsion [6]. Nevertheless, literature is lacking in description of postoperative imaging of the untwisted ovary, which we found, could be misleading in the management.
2. CASE
A 17 year old nulliparous woman with no past medical or surgical history presented with abdominal pain in right lower quadrant over the last month. The pain has been present on and off. She reported no diarrhea, constipation or vomiting. On rectal exam a tender right adnexal mass was palpated.
On laboratory work up, the white blood count was 11.5 with 79% neutrophils. An abdominal sonogram visualized a 6.1 × 8.2 × 7.6 right ovarian complex mass which was confirmed by CT scan. Diagnostic laparoscopy revealed the double torsion of right adnexa over the infundibulo-pelvic ligament. No cyst or mass were visualized. An untwisting was performed with immediate return of color with perfusion. The postoperative course was uneventful and patient was discharged to follow up with sonogram.
The patient returned in 3 weeks for sonogram which revealed a complex right adnexal mass 9.96 × 9.4 × 7.75 with cystic and solid components and no flow on Doppler was visualized. Patient was referred for MRI—which confirmed the findings (complex non-enhanced mass with multiple cystic components) (Figure 1). Patient was asymptomatic and in view of previous benign intraoperative findings, it was decided to withhold surgical intervention and further follow up was planned.
Follow up sonogram in 10 weeks revealed normal size ovary 5.48 × 4.49 × 2.9 cm with good flow on Doppler.
3. DISCUSSION
This case report of radiographic presentation of untwisted ovary describes the natural changes undergoing in the ovary. Definitive diagnosis of ovarian torsion is usually made during surgical intervention [7]. Clinical diagnosis is based on presentation in adjunct with imaging studies [8]. The management of torsion includes salpingoophorectomy and conservative surgery, including detorsion and cyst aspiration or cystectomy as necessary [1]. Ovariopexy is suggested to prevent ipsilateral recurrence or contralateral occurrence. This management is particularly valuable in case of previous removal of one of the ovaries [9].
Follow up in case of ovarian preservation (detorsion) usually includes a sonogram performed 6 to 8 weeks after surgery [8]. In our case patient presented earlier than the scheduled follow up and was found to have a
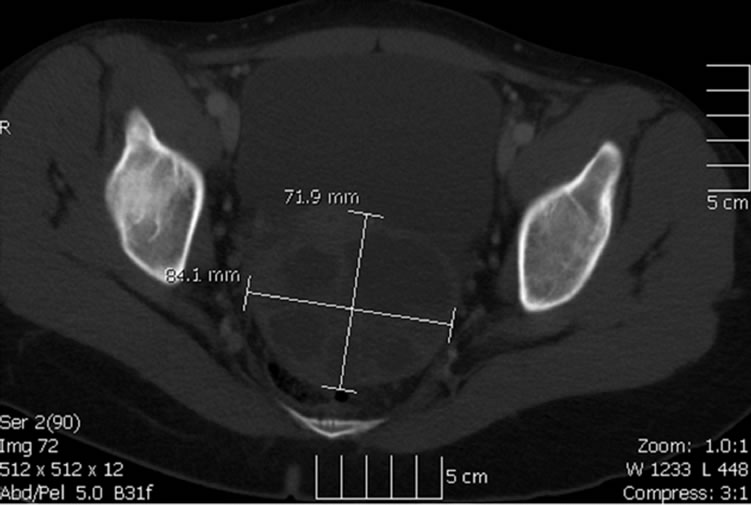
Figure 1. Complex right adnexal mass 9.96 × 9.4 × 7.75—An MRI image consistent with hematoma formation.
complex non-enhancing mass with multiple cystic components on ultrasound. This description is highly consistent with hematoma formed after reperfusion. Absence of clinical manifestations and knowledge about normal anatomy obtained during surgery allowed us to proceed with conservative management without any further surgical intervention. The fact that subsequent imaging studies revealed normal appearing ovaries, shows that multiple cystic changes in view of the absent mass on prior laparoscopy could represent multiple different stages hematoma after reperfusion which underwent spontaneous resolution. Therefore, our case highlights the importance of conservative management after detorsion follow up, especially in the absence of clinical signs and symptoms.
REFERENCES
- Oelsner, G., et al. (1993) Long-term follow-up of the twisted ischemic adnexa managed by detorsion. Fertility and Sterility, 60, 976-979.
- Wagaman, R. and Williams, R.S. (1990) Conservative therapy for adnexal torsion. A case report. Journal of Reproductive Medicine, 35, 833-834.
- Harkins, G. (2007) Ovarian torsion treated with untwisting: Second look 36 hours after untwisting. Journal of Minimally Invasive Gynecology, 14, 270. doi:10.1016/j.jmig.2006.10.006
- Kamprath, S., et al. (1998) Laparoscopic adnexal preservation in a patient with complete torsion—A case report. European Journal of Obstetrics & Gynecology and Reproductive Biology, 78, 113-115. doi:10.1016/S0301-2115(97)00273-X
- Li, Y.T., et al. (2005) Laparoscopic detorsion of twisted ovary. Journal of the Chinese Medical Association, 68, 595-598. doi:10.1016/S1726-4901(09)70100-5
- Chang, H.C., Bhatt, S. and Dogra, V.S. (2008) Pearls and pitfalls in diagnosis of ovarian torsion. Radiographics, 28, 1355-1368. doi:10.1148/rg.285075130
- Argenta, P.A., et al. (2000) Torsion of the uterine adnexa. Pathologic correlations and current management trends. Journal of Reproductive Medicine, 45, 831-836.
- Galinier, P., et al. (2009) Ovarian torsion. Management and ovarian prognosis: A report of 45 cases. Journal of Pediatric Surgery, 44, 1759-1765. doi:10.1016/j.jpedsurg.2008.11.058
- Dolgin, S.E., Lublin, M. and Shlasko, E. (2000) Maximizing ovarian salvage when treating idiopathic adnexal torsion. Journal of Pediatric Surgery, 35, 624-626. doi:10.1053/jpsu.2000.0350624
NOTES
*Corresponding author.