Paper Menu >>
Journal Menu >>
 Surgical Science, 2011, 2, 338-340 doi:10.4236/ss.2011.26072 Published Online August 2011 (http://www.SciRP.org/journal/ss) Copyright © 2011 SciRes. SS Isolated Full Thickness Jejunal Necrosis Following Sulphuric Acid Cocktail Ingestion—A Clinical Case Report —Isolated Corrosive Jejunal Necrosis S. S. Pankaja, George J. Valooran, Sri Aurobindo Prasad Das, L. Suvasini, R. Aravind, Vikram Kate, Pankaj Kundra* Departments of Surgery and Anaesthesiology, Jawaharlal Institute of Postgraduate Medical Education and Res earch, Puducherry, India E-mail: *drvikramkate@gmail.com Received February 16, 2011; revised March 24, 201 1; acce p te d Ma y 16, 2011 Abstract Isolated involvement of the lower gastrointestinal tract with relative sparing of the oesophagus and the stomach is extremely rare following corrosive agent ingestion. We report a case of isolated full thickness jejunal necrosis following sulphuric acid cocktail ingestion. A 42 year old man presented with history of consuming 200 ml of sulphuric acid mixed with alcohol, with suicidal intent. On exploration there were mul- tiple, full thickness necrotic areas in the proximal jejunum with minimal congestion of the oesophagus, stomach and duodenum. Inversion of the jejunal necrotic areas with feeding jejunostomy was carried out. However postoperatively patient developed progressive pulmonary insufficiency with features of sepsis and expired on the nineteenth day following a bout of massive haematemesis. Corrosive agents when taken in considerable amount mixed with other fluids can lead to full thickness small bowel necrosis with relative sparing of the proximal gastrointestinal tract. Keywords: Corrosive Injury, Acid Ingestion, Bowel Necrosis 1. Introduction Accidental or suicidal ingestion of sulphuric and hydro- chloric acids, leading to esophagogastric injury is not uncommon [1-3]. The site, extent and intensity of dam- age depend on the multiple factors related to the caustic agent, duration of contact and the victim [4]. Concomi- tant acid injury of the lower gastrointestinal tract is a rare occurrence due to acid induced pylorospasm with con- sequent gastric pooling, and neutralizing effect of the bile [1,5-7]. However, isolated necrosis of the lower gas- trointestinal tract with relative sparing of the proximal gastrointestinal tract is extremely rare with limited re- ports [2,4,5]. Here we present a case of isolated full thickness jejunal necrosis with relative sparing of the proximal gastrointestinal tract following sulphuric acid cocktail ingestion. 2. The Case A 42 year old manual labourer presented to emergency department with history of having consumed battery sulphuric acid mixed with alco hol, around 200 ml, under the influence of alcoh ol with suicidal intent 3 hours prior to presentatio n. Fo llowing inge stion p atien t h ad v omiting which had both fresh and altered blood and developed severe burning pain in epigastric and retrosternal regions. At presentation patien t was severely agitated. Abdominal examination revealed mild epigastric guarding, tender- ness and normal bowel sounds. As patient had mild epi- gastric guarding upper gastrointestinal endoscopy was not performed as there was a likely risk of perforation due to inflation for endoscopy. Initial arterial blood gas analysis revealed severe metabolic acidosis. Skiagram of the chest, electrocardiogram and other biochemical tests including serum amylase were normal. Patient was re- suscitated, started on antibiotics and shifted to surgical intensive care unit. Two days later, patient developed abdominal disten- sion with peritoneal signs for which he was posted for an exploratory laparotomy. Considering the patient being full stomach and scheduled for emergency laparotomy, 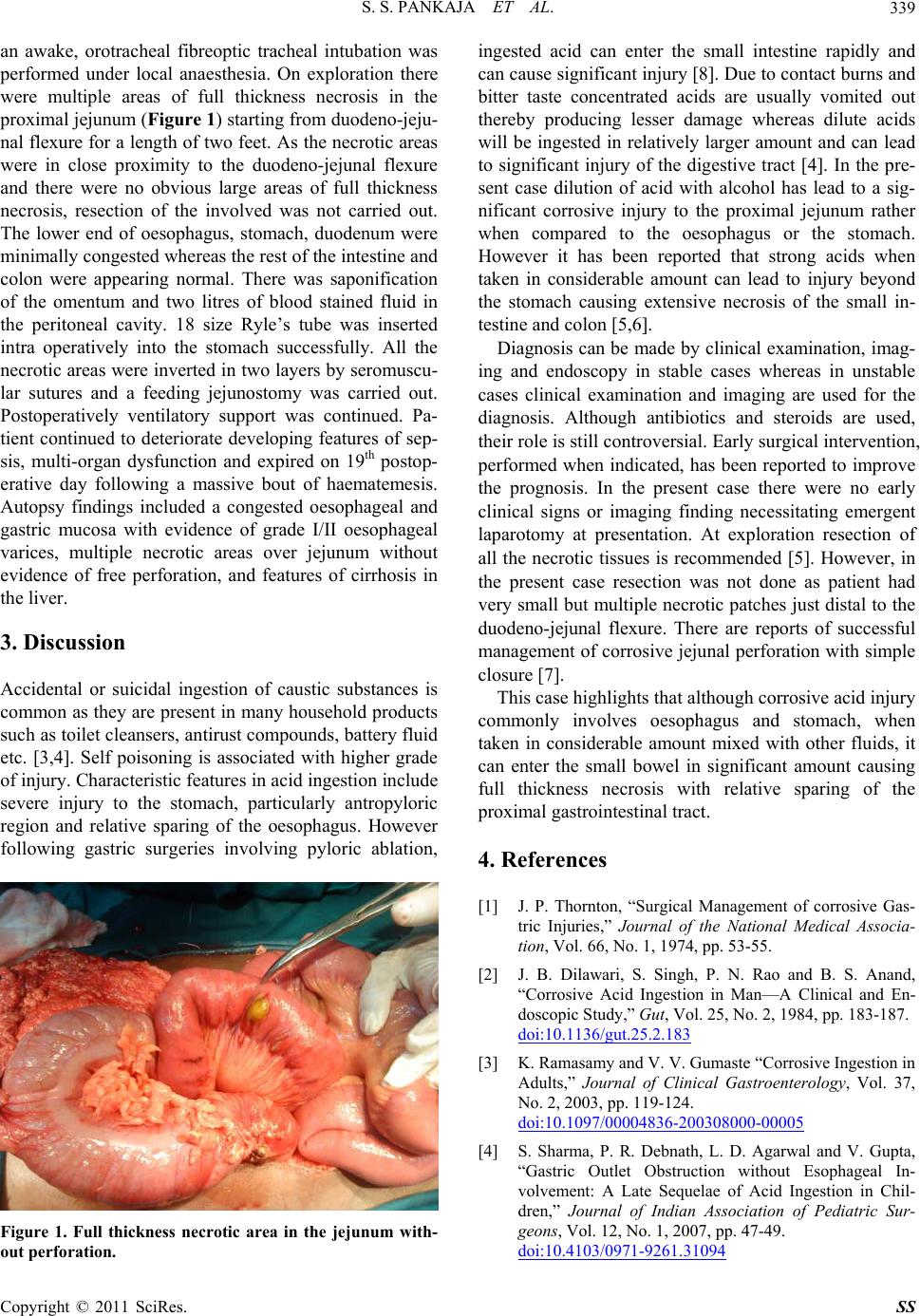 S. S. PANKAJA ET AL. Copyright © 2011 SciRes. SS 339 an awake, orotracheal fibreoptic tracheal intubation was performed under local anaesthesia. On exploration there were multiple areas of full thickness necrosis in the proximal jejunum (Figure 1) starting fr om duodeno-j eju- nal flexure for a leng th of two feet. As the necrotic areas were in close proximity to the duodeno-jejunal flexure and there were no obvious large areas of full thickness necrosis, resection of the involved was not carried out. The lower end of oesophagus, stomach, duodenum were minimally congested whereas the rest of the intestine and colon were appearing normal. There was saponification of the omentum and two litres of blood stained fluid in the peritoneal cavity. 18 size Ryle’s tube was inserted intra operatively into the stomach successfully. All the necrotic areas were inverted in two layers by seromuscu- lar sutures and a feeding jejunostomy was carried out. Postoperatively ventilatory support was continued. Pa- tient continued to deteriorate developing features of sep- sis, multi-organ dysfunction and expired on 19th postop- erative day following a massive bout of haematemesis. Autopsy findings included a congested oesophageal and gastric mucosa with evidence of grade I/II oesophageal varices, multiple necrotic areas over jejunum without evidence of free perforation, and features of cirrhosis in the liver. 3. Discussion Accidental or suicidal ingestion of caustic substances is common as they are presen t in many household products such as toilet cleansers, antirust compounds, battery fluid etc. [3,4]. Self poisoning is associated with higher grade of injury. Characteristic features in acid ingestion include severe injury to the stomach, particularly antropyloric region and relative sparing of the oesophagus. However following gastric surgeries involving pyloric ablation, Figure 1. Full thickness necrotic area in the jejunum with- out perforation. ingested acid can enter the small intestine rapidly and can cause significant inju ry [8]. Due to contact burn s and bitter taste concentrated acids are usually vomited out thereby producing lesser damage whereas dilute acids will be ingested in relatively larger amount and can lead to significant injury of the digestive tract [4]. In the pre- sent case dilution of acid with alcohol has lead to a sig- nificant corrosive injury to the proximal jejunum rather when compared to the oesophagus or the stomach. However it has been reported that strong acids when taken in considerable amount can lead to injury beyond the stomach causing extensive necrosis of the small in- testine and colon [5,6]. Diagnosis can be made by clinical examination, imag- ing and endoscopy in stable cases whereas in unstable cases clinical examination and imaging are used for the diagnosis. Although antibiotics and steroids are used, their role is still controversial. Early su rgical interven tion, performed when indicated, has been reported to improve the prognosis. In the present case there were no early clinical signs or imaging finding necessitating emergent laparotomy at presentation. At exploration resection of all the necrotic tissues is recommended [5]. However, in the present case resection was not done as patient had very small but multiple necrotic patches just distal to th e duodeno-jejunal flexure. There are reports of successful management of corrosive jejunal perforation with simple closure [7]. This case highlights that although corrosive acid injur y commonly involves oesophagus and stomach, when taken in considerable amount mixed with other fluids, it can enter the small bowel in significant amount causing full thickness necrosis with relative sparing of the proximal gastrointestinal tract. 4. References [1] J. P. Thornton, “Surgical Management of corrosive Gas- tric Injuries,” Journal of the National Medical Associa- tion, Vol. 66, No. 1, 1974, pp. 53-55. [2] J. B. Dilawari, S. Singh, P. N. Rao and B. S. Anand, “Corrosive Acid Ingestion in Man—A Clinical and En- doscopic Study,” Gut, Vol. 25, No. 2, 1984, pp. 183-187. doi:10.1136/gut.25.2.183 [3] K. Ramasamy and V. V. Gumaste “Corrosive Ingestion in Adults,” Journal of Clinical Gastroenterology, Vol. 37, No. 2, 2003, pp. 119-124. doi:10.1097/00004836-200308000-00005 [4] S. Sharma, P. R. Debnath, L. D. Agarwal and V. Gupta, “Gastric Outlet Obstruction without Esophageal In- volvement: A Late Sequelae of Acid Ingestion in Chil- dren,” Journal of Indian Association of Pediatric Sur- geons, Vol. 12, No. 1, 2007, pp. 47-49. doi:10.4103/0971-9261.31094  S. S. PANKAJA ET AL. Copyright © 2011 SciRes. SS 340 [5] P. Cattan, N. Munoz-Bongrand, T. Berney, B. Halimi, E. Sarfati and M. Celerier, “Extensive abdominal surgery after caustic ingestion,” Annals of Surgery, Vol. 231, No. 4, 2000, pp. 519-523. doi:10.1097/00000658-200004000-00010 [6] Q. Zeng, H. Zhou, X. Zheng, Z. Li, M. Zhou, S. Han, et al., “Total Gastrointestinal Tract Necrosis after Ingesting a Considerable Amount of Hydrochloric Acid,” Journal of Gastrointestinal Surgery, Vol. 13, No. 3, 2009, pp. 578-80. doi:10.1007/s11605-008-0524-9 [7] O. Boybeyi, I. Karnak, F. C. Tanyel and M. E. Senocak, “Management of Unusually Extensive Esophagogastric Corrosive Injuries: Emergency Measures and Gastric Reconstruction,” Journal of Pediatric Surgery, Vol. 44, No. 5, 2009, pp. 1022-1026. doi:10.1016/j.jpedsurg.2009.02.001 [8] J. M. Chang, M. H. Wu, W. W. Lai, M. Y. Lin, Y. F. Tsai, I. L. Hsu, et al., “Acid Corrosive Injury in Patients with a History of Partial Gastrectomy: Outcome Analysis,” Di- gestive Surgery, Vol. 24, No. 3, 2007, pp. 202-207. doi:10.1159/000102900 |