K. Okazaki et al. / Health 3 (2011) 518-523
Copyright © 2011 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/
523
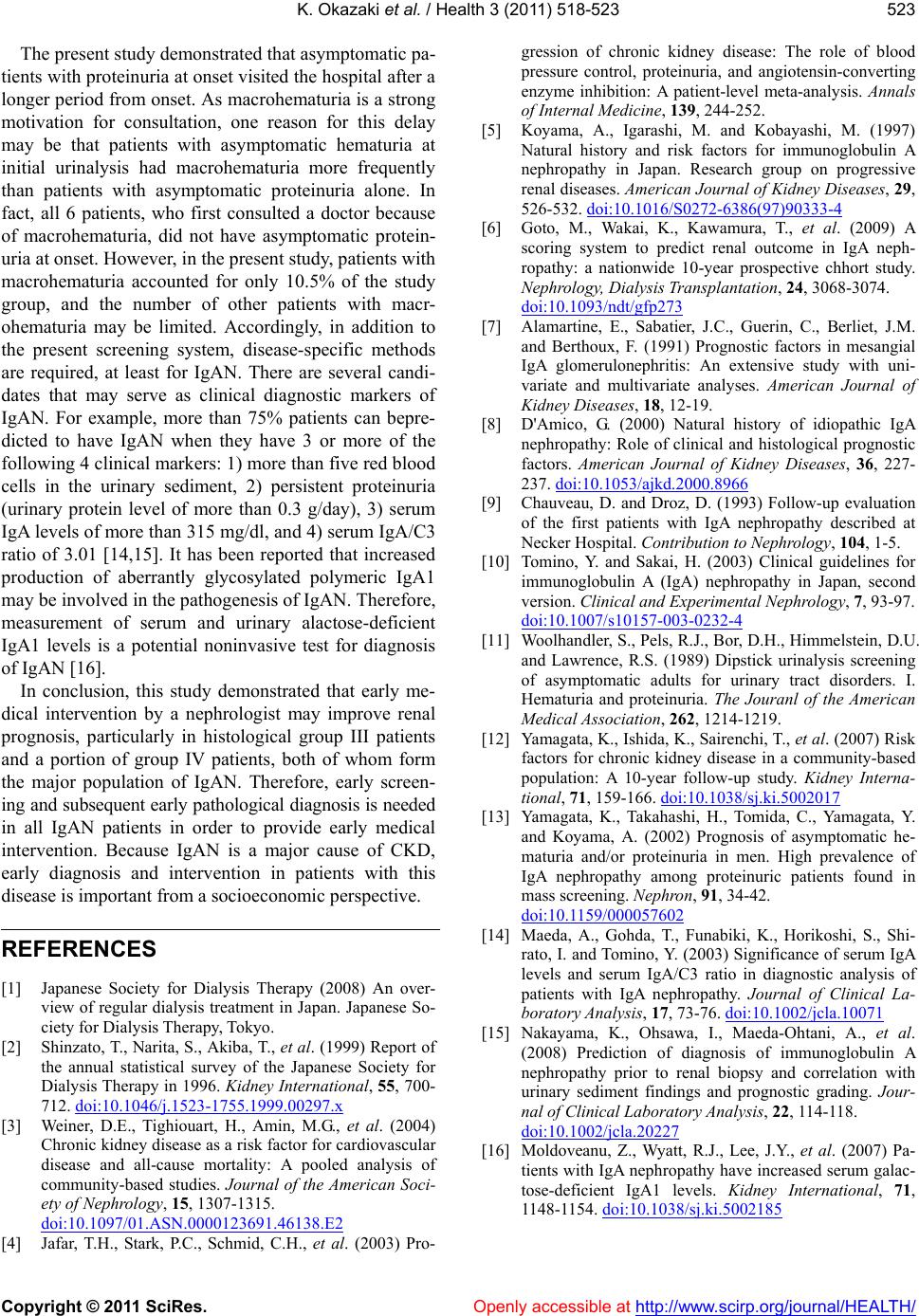
The present study demonstrated that asymptomatic pa-
tients with proteinuria at onset visited the hospital after a
longer period from onset. As macrohematuria is a strong
motivation for consultation, one reason for this delay
may be that patients with asymptomatic hematuria at
initial urinalysis had macrohematuria more frequently
than patients with asymptomatic proteinuria alone. In
fact, all 6 patients, who first consulted a doctor because
of macrohematuria, did not have asymptomatic protein-
uria at onset. However, in the present study, patients with
macrohematuria accounted for only 10.5% of the study
group, and the number of other patients with macr-
ohematuria may be limited. Accordingly, in addition to
the present screening system, disease-specific methods
are required, at least for IgAN. There are several candi-
dates that may serve as clinical diagnostic markers of
IgAN. For example, more than 75% patients can bepre-
dicted to have IgAN when they have 3 or more of the
following 4 clinical markers: 1) more than five red blood
cells in the urinary sediment, 2) persistent proteinuria
(urinary protein level of more than 0.3 g/day), 3) serum
IgA levels of more than 315 mg/dl, and 4) serum IgA/C3
ratio of 3.01 [14,15]. It has been reported that increased
production of aberrantly glycosylated polymeric IgA1
may be involved in the pathogenesis of IgAN. Therefore,
measurement of serum and urinary alactose-deficient
IgA1 levels is a potential noninvasive test for diagnosis
of IgAN [16].
In conclusion, this study demonstrated that early me-
dical intervention by a nephrologist may improve renal
prognosis, particularly in histological group III patients
and a portion of group IV patients, both of whom form
the major population of IgAN. Therefore, early screen-
ing and subsequent early pathological diagnosis is needed
in all IgAN patients in order to provide early medical
intervention. Because IgAN is a major cause of CKD,
early diagnosis and intervention in patients with this
disease is important from a socioeconomic perspective.
REFERENCES
[1] Japanese Society for Dialysis Therapy (2008) An over-
view of regular dialysis treatment in Japan. Japanese So-
ciety for Dialysis Therapy, Tokyo.
[2] Shinzato, T., Narita, S., Akiba, T., et al. (1999) Report of
the annual statistical survey of the Japanese Society for
Dialysis Therapy in 1996. Kidney International, 55, 700-
712. doi:10.1046/j.1523-1755.1999.00297.x
[3] Weiner, D.E., Tighiouart, H., Amin, M.G., et al. (2004)
Chronic kidney disease as a risk factor for cardiovascular
disease and all-cause mortality: A pooled analysis of
community-based studies. Journal of the American Soci-
ety of Nephrology, 15, 1307-1315.
doi:10.1097/01.ASN.0000123691.46138.E2
[4] Jafar, T.H., Stark, P.C., Schmid, C.H., et al. (2003) Pro-
gression of chronic kidney disease: The role of blood
pressure control, proteinuria, and angiotensin-converting
enzyme inhibition: A patient-level meta-analysis. Annals
of Internal Medicine, 139, 244-252.
[5] Koyama, A., Igarashi, M. and Kobayashi, M. (1997)
Natural history and risk factors for immunoglobulin A
nephropathy in Japan. Research group on progressive
renal diseases. American Journal of Kidney Diseases, 29,
526-532. doi:10.1016/S0272-6386(97)90333-4
[6] Goto, M., Wakai, K., Kawamura, T., et al. (2009) A
scoring system to predict renal outcome in IgA neph-
ropathy: a nationwide 10-year prospective chhort study.
Nephrology, Dialysis Transplantation, 24, 3068-3074.
doi:10.1093/ndt/gfp273
[7] Alamartine, E., Sabatier, J.C., Guerin, C., Berliet, J.M.
and Berthoux, F. (1991) Prognostic factors in mesangial
IgA glomerulonephritis: An extensive study with uni-
variate and multivariate analyses. American Journal of
Kidney Diseases, 18, 12-19.
[8] D'Amico, G. (2000) Natural history of idiopathic IgA
nephropathy: Role of clinical and histological prognostic
factors. American Journal of Kidney Diseases, 36, 227-
237. doi:10.1053/ajkd.2000.8966
[9] Chauveau, D. and Droz, D. (1993) Follow-up evaluation
of the first patients with IgA nephropathy described at
Necker Hospital. Contribution to Nephrology, 104, 1-5.
[10] Tomino, Y. and Sakai, H. (2003) Clinical guidelines for
immunoglobulin A (IgA) nephropathy in Japan, second
version. Clinical and Experimental Nephrology, 7, 93-97.
doi:10.1007/s10157-003-0232-4
[11] Woolhandler, S., Pels, R.J., Bor, D.H., Himmelstein, D.U.
and Lawrence, R.S. (1989) Dipstick urinalysis screening
of asymptomatic adults for urinary tract disorders. I.
Hematuria and proteinuria. The Jouranl of the American
Medical Associati on, 262, 1214-1219.
[12] Yamagata, K., Ishida, K., Sairenchi, T., et al. (2007) Risk
factors for chronic kidney disease in a community-based
population: A 10-year follow-up study. Kidney Interna-
tional, 71, 159-166. doi:10.1038/sj.ki.5002017
[13] Yamagata, K., Takahashi, H., Tomida, C., Yamagata, Y.
and Koyama, A. (2002) Prognosis of asymptomatic he-
maturia and/or proteinuria in men. High prevalence of
IgA nephropathy among proteinuric patients found in
mass screening. Nephron, 91, 34-42.
doi:10.1159/000057602
[14] Maeda, A., Gohda, T., Funabiki, K., Horikoshi, S., Shi-
rato, I. and Tomino, Y. (2003) Significance of serum IgA
levels and serum IgA/C3 ratio in diagnostic analysis of
patients with IgA nephropathy. Journal of Clinical La-
boratory Analysis, 17, 73-76. doi:10.1002/jcla.10071
[15] Nakayama, K., Ohsawa, I., Maeda-Ohtani, A., et al.
(2008) Prediction of diagnosis of immunoglobulin A
nephropathy prior to renal biopsy and correlation with
urinary sediment findings and prognostic grading. Jour-
nal of Clinical Laboratory Analysis, 22, 114-118.
doi:10.1002/jcla.20227
[16] Moldoveanu, Z., Wyatt, R.J., Lee, J.Y., et al. (2007) Pa-
tients with IgA nephropathy have increased serum galac-
tose-deficient IgA1 levels. Kidney International, 71,
1148-1154. doi:10.1038/sj.ki.5002185