V. I. Gridnev et al. / Health 3 (2011) 477-481
Copyright © 2011 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/
481
The approach offered allows to determine bicycle er-
gometry result reliability in cases of positive or negative
results of the test individually in each patient and de-
crease possibility of diagnostic mistakes. Limitations of
the method offered for CHD diagnostics are initial heart
rate increase (heart rate more then 100 beats per minute)
and impossibility to obtain suitable for the spectral an-
alysis bicycle ergometry rhythmograms due to noise and
artifacts presence.
4. CONCLUSIONS
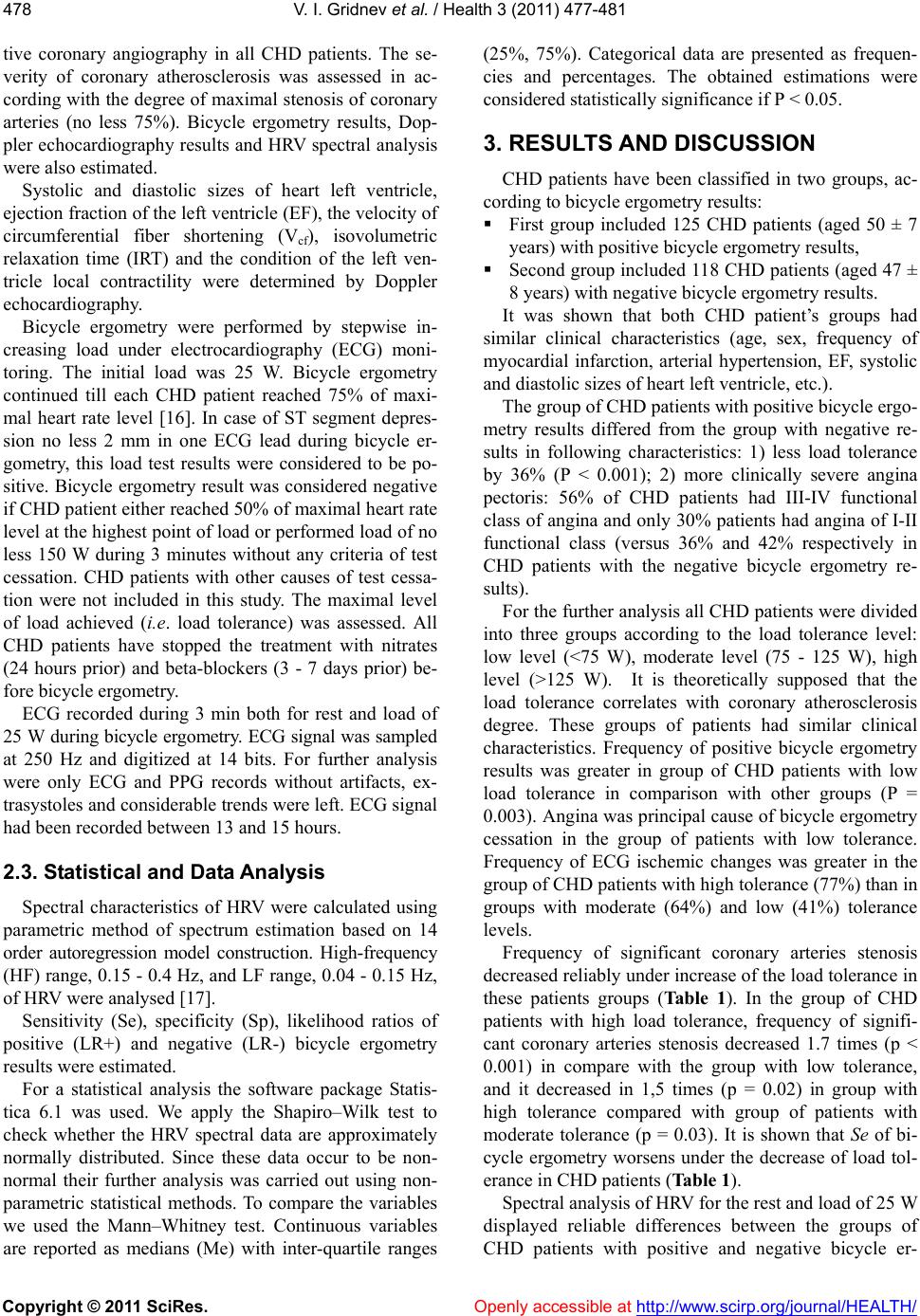
Thus, the analysis of spectral power of LF range of
HRV allows to advance diagnostic value of bicycle er-
gometry results in CHD patients. It is necessary to use a
complex assessment of bicycle ergometry results taking
into account the load tolerance level and a power of LF
range of HRV spectrum. Combined use of the load tol-
erance and LF range spectral power levels (in rest and
during 25 W loading) the validity of an individual exer-
cise raises 2 - 3 times (in particular, bicycle ergometry)
test result compared with standard procedure of the bi-
cycle ergometry results analysis in CHD patients.
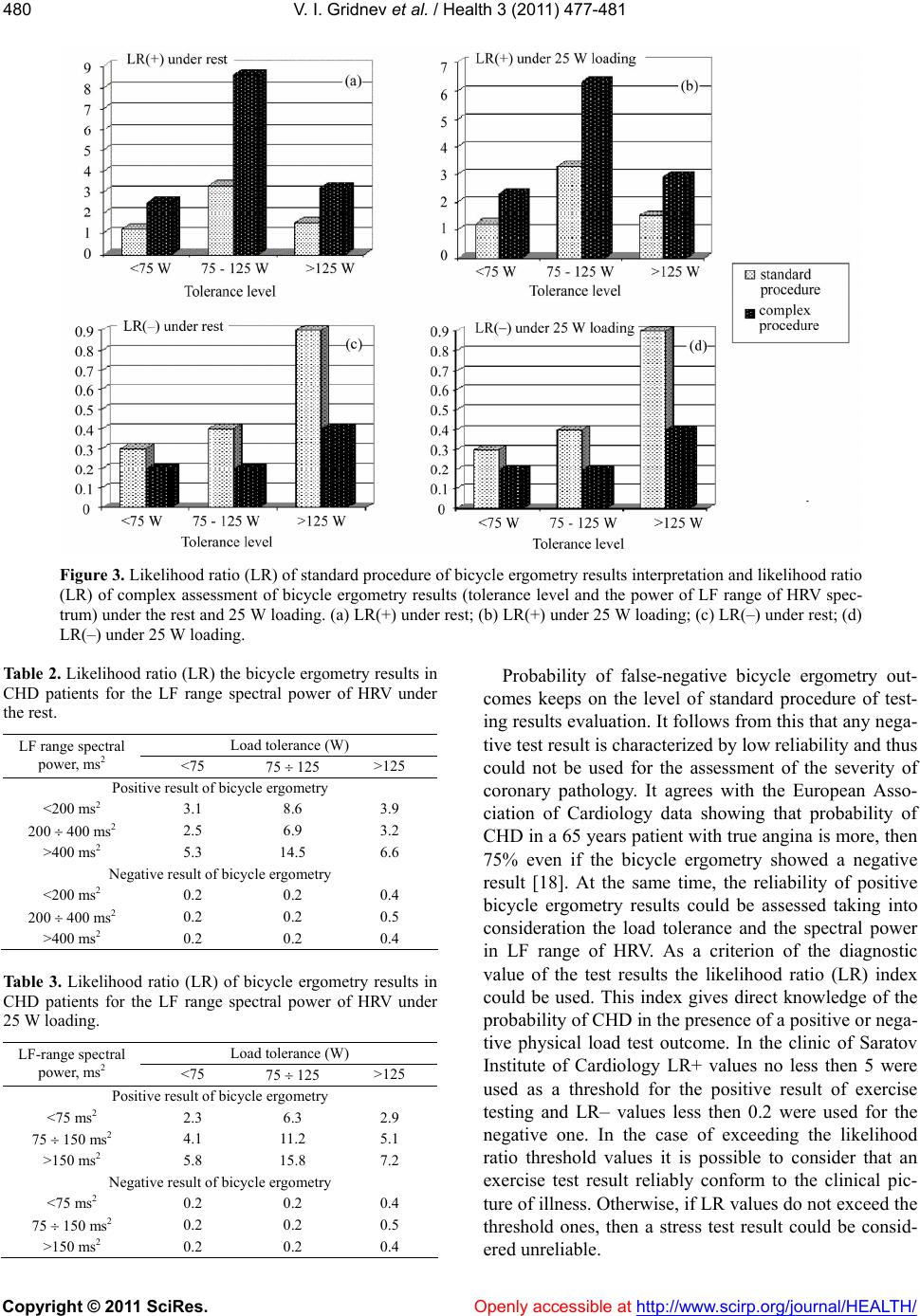
Table 2 can be used for preliminary assessment of the
bicycle ergometry results especially in CHD patients
with low levels of LF range spectral power (<400 ms2).
Further the obtained value of likelihood ratio can be
specified with the help of Tab le 3. Table data are con-
structed for CHD patients with hemodynamically sig-
nificant atherosclerotic stenosis at least one coronary
vessel (stenosis degree >50% according to data of coro-
narography).
REFERENCES
[1] European Society of Cardiology (1993) Guidelines for
cardiac exercise testing: ESC working group on exercise
physiology, physiopathology and electrocardiography.
European Heart Journal, 14, 969-988.
[2] Porta, C. and Bernardi, L. (2001) Interaction between
respiration, autonomic function, and respiratory pattern
inheart failure. New possibilities of rehabilitation inter-
vention. Italian Heart Journal, 2, 624-627.
[3] Juhani, K.E., Marku, J.I., Heikki, V.H., et al. (1993) Re-
sponses of heart rate variability to coronari occlusion
during coronari angioplasty. American Journal of Cardi-
ology, 72, 1026-1030.
doi:10.1016/0002-9149(93)90857-9
[4] De Boer, R.W., Karemuker, J.M. and Stracker, J. (1986)
On the spectral analysis of blood pressure variability.
American Journal of Physiology, 251, 685-687.
[5] De Boer, R.W., Karemuker, J.M. and Stracker, J. (1985)
Relationships between short-term blood pressure fluctua-
tions and heart variability in resting subjects. II: A simple
model. Medical & B iological Engineering & Computing,
23, 359-364. doi:10.1007/BF02441590
[6] De Boer, R.W., Karemuker, J.M. and Stracker, J. (1985)
Relationships between short-term blood pressure fluctua-
tions and heart variability in resting subjects. I: A spectral
analysis approach. Medical & Biological Engineering &
Computing, 23, 352-358. doi:10.1007/BF02441589
[7] De Boer, R.W., Karemuker, J.M. and Stracker, J. (1987)
Hemodynamic fluctuations and baroreflex sensitivity in
humans: A beat-to-beat model. American Journal of
Physiology, 253, 680-687.
[8] Madwed, J.B., Albrecht, P., Mark, R.G. and Cohen, R.J.
(1989) Low-frequency oscillation in arterial pressure and
heart-rate: A simple computer model. American Journal
of Physiology, 256, 1573-1579.
[9] Pagani, M. and Malliani, A. (2000) Interpreting oscilla-
tions of muscle sympathetic nerve activity and heart rate
variability. Journal of Hypertension, 18, 1709-1719.
doi:10.1097/00004872-200018120-00002
[10] Sleight, P., La Rovere, M.T., Mortara, A., et al. (1995)
Physiology and pathophysiology of heart rate variability
in humans: is power spectral analysis largely an index of
baroreflex gain? Clinical Science, 88, 103-109.
[11] Richter, D.W. and Spyer, K.M. (1990) Cardiorespiratory
control. Oxford University Press, New York.
[12] Cevese, A., Grasso, R., Poltronieri, R. and Schena, F.
(1995) Vascular resistance and arterial pressure low-fre-
quency oscillations in the anesthetized dog. American
Journal of Physiology, 268, 7-16.
[13] Whittam, A.M., Claytont, R.H., Lord, S.W., et al. (2000)
Heart rate and blood pressure variability in normal sub-
jects compared with data from beat-to-beat models de-
veloped from de Boer’s model of the cardiovascular sys-
tem. Physiological Measuremen, 21, 305-318.
doi:10.1088/0967-3334/21/2/310
[14] Bernardi, L., Passino, C., Spadacini, G., et al. (1997)
Arterial baro-receptor as determinants of 0.1 Hz and res-
piration-related changes in blood pressure and heart rate
spectra. IOS Press, Amsterdam.
[15] Simon, C.M. (2002) Neural influeces on cardiovascular
variability: Possibilities and pitfalls. The American
Physiological Society, 282, 6-20.
[16] Andersen, K., Shephard, R., Denolin, H., et al. (1979)
Fundamentals of exercise testing. WHO, Geneva.
[17] American Heart Association (1996) Heart rate variability.
Standarts of measurement, physiological interpretation
and clinical use. Circulation, 93, 1043-1065.
doi:10.1161/01.CIR.93.5.1043
[18] European Society of Cardiology (1997) Management of
stable angina pectoris: Recommendations of the task
force of the European Society of Cardiology. European
Heart Journal, 18, 394-413.