58 S. YUI ET AL.
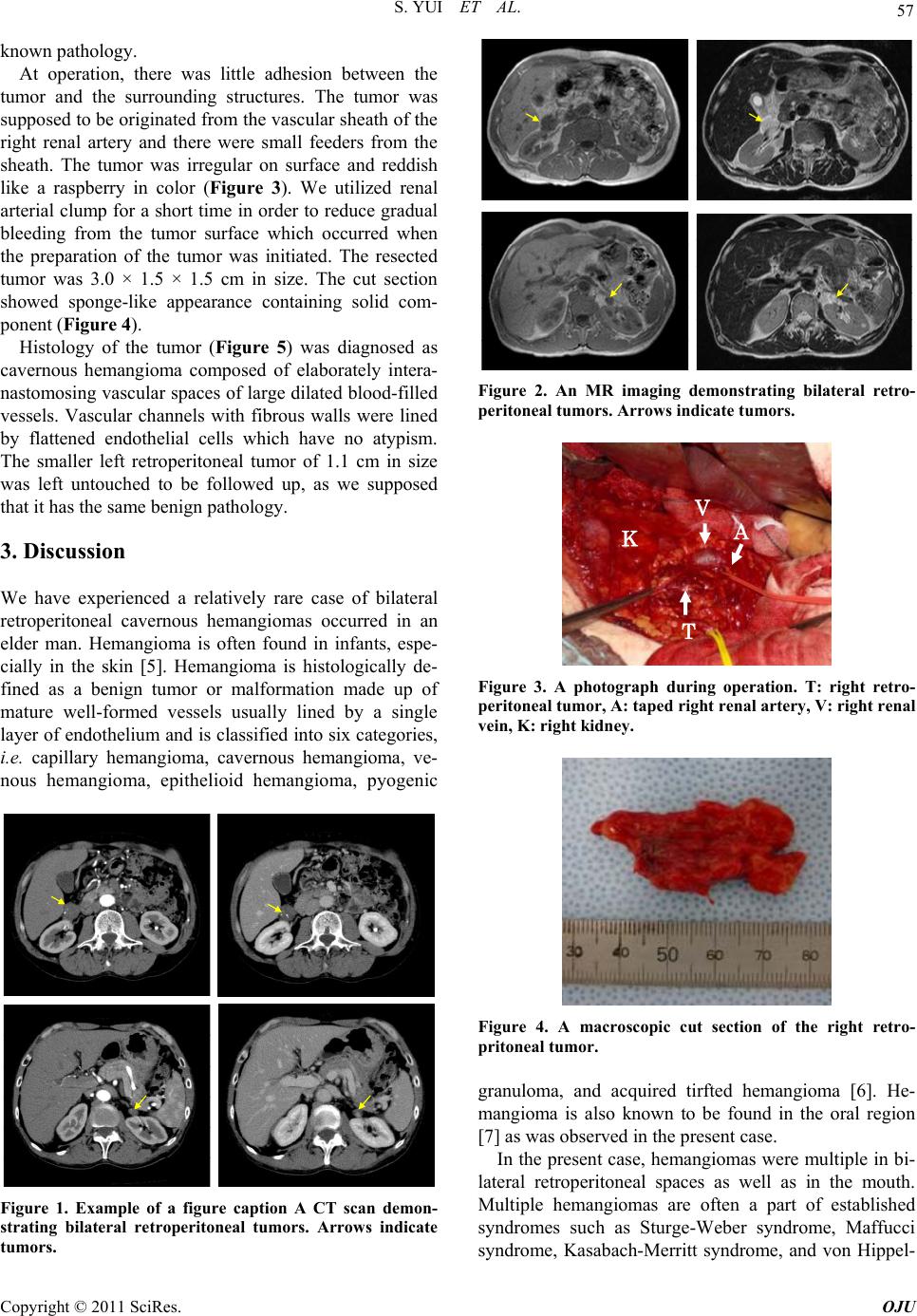
Figure 5. Hematoxylin and eosin staining of the right re-
troperitoneal tumor showing cavernous hemangioma.
Lindau disease, but this case did not seem to apply to
them as it lacks in the characteristics of those disorders.
There have been no previous cases of retroperitoneal
cavernous hemangioma as a presentation of multiple
hemangiomas.
Surgical removal of retroperitoneal tumors is indicated
as long as the possibility of poten tial malignan cy remains.
Maximum diameter of malignant retroperitoneal tumors
is reported to be larger than that of benign ones (11.45 ±
1.90 cm vs 5.31 ± 0.43 cm) [3]. The tumor size of the
present case was relatively small and the probability of
malignancy was not very high in the view points of tu-
mor size, then we might have followed up the interval
change in the tumor size before indicating surgery. Addi-
tionally, retroperitoneal hemangiomas have a risk of
rupture and bleeding [8] even they are histologically be-
nign, leading to a rational of choosing surgical extirpa-
tion especially when they are large. Although we adopted
open surgical approach, laparoscopic resection of retrop-
eritoneal cavernous hemangioma has been reported
[9,10]. It may be appropriate to remove retroperitoneal
hemangiomas laparoscopically or retroperitoneoscopi-
cally if they are probably benign .
Besides surgical treatments, there are some options as
corticosteroid therapy and radiotherapy in the treatment
of hemangioma. While corticosteroid therapy is mainly a
choice of treatments of capillary hemangioma [11], there
is a report of unresectable 8 × 5 cm retroperitoneal cav-
ernous hemangioma diagnosed in a female neonate 20
days after birth and showing anemia and thrombocyto-
penia, which disappeared following oral corticosteroid
therapy [12]. Radiotherapy is also given to treat symp-
tomatic hemangiomas [13].
In the present case, the smaller left retroperitoneal tu-
mor of 1.1 cm in size was left untouched to be followed
up, as we supposed that it has the same ben ign pathology.
When the left retroperiton eal tumor grows larger enough ,
we may need to re-consider if he needs some treatment
including surgery.
4. References
[1] G. T. Pack and E. J. Tabah, “Collective Review: Primary
Retroperitoneal Tumors; a Study of 120 Cases,” Surgery,
Gynecology & Obstetrics, Vol. 99, No. 3, 1954, pp. 209-
231.
[2] J. W. Braasch and A. B. Mon, “Primary Retroperitoneal
Tumors,” Surgical Clinics of North America, Vol. 47, No.
3, 1967, pp. 663-678.
[3] J. Nakashima, M. Ueno, K. Nakamura, M. Tachibana, S.
Baba, N. Deguchi, H. Tazaki and M. Murai, “Differential
Diagnosis of Primary Benign and Malignant Retroperito-
neal Tumors,” International Journal of Urology, Vol. 4,
No. 5, 1997, pp. 441-446.
doi:10.1111/j.1442-2042.1997.tb00282.x
[4] N. Takaha, M. Hosomi, K. Se kii, S. Nakamori, K. Itoh, S.
Sagawa, T. Kido, M. Satani, S. Kawamoto and K. Sato,
“Retroperitoneal Cavernous Hemangioma: A Case Re-
port,” Hinyokika Kiyo, Vol. 37, No. 7, 1991, pp. 725-728.
[5] B. A. Drolet, N. B. Esterly and I. J. Frieden, “Heman-
giomas in Children,” New England Journal of Medicine,
Vol. 341, No. 3, 1999, pp. 173-181.
doi:10.1056/NEJM199907153410307
[6] S. W. Weiss, “Histological Typing of Soft Tissue Tu-
mours,” Vol. 2, Springer-Verlag, New York, 1994.
[7] N. Kawachi, “A Comparative Histopathological and Im-
munohistochemically Study of Capillary Hemangioma,
Pyogenic Granuloma and Cavernous Hemangioma in the
Oral Region: With Special Reference to Vascular Prolif-
eration Factors,” International Journal of Oral-Medical
Sciences, Vol. 9, No. 3, 2011, pp. 241-251.
doi:10.5466/ijoms.9.241
[8] T. L. Forbes, “Retroperitoneal Hemorrhage Secondary to
a Ruptured Cavernous Hemangioma,” Canadian Journal
of Surgery, Vol. 48, No. 1, 2005, pp. 78-79.
[9] Y. S. Choi and H. K. Oh, “Laparoscopic Resection of a
Retroperitoneal Hemangioma Arising from Ovarian Ves-
sels,” Journal of Minimally Invasive Gynecology, Vol. 16,
No. 6, 2009, pp. 778-780.
doi:10.1016/j.jmig.2009.07.017
[10] R. N. P. Martín, J. E. Zarranz, C. V. F. Mdel, C. C. Re-
dondo, J. A. Sesmero and J. Martinez-Sagarra, “Laparo-
scopic Resection of Retroperitoneal Venous Heman-
gioma,” Journal of Urology, Vol. 171, No. 1, 2004, p.
336.
[11] M. T. Edgerton, “The Treatment of Hemangiomas: With
Special Reference to the Role of Steroid Therapy,” An-
nals of Surgery, Vol. 183, No. 5, 1976, pp. 517-532.
doi:10.1097/00000658-197605000-00009
[12] Y. Kasubuchi, T. Sawada and T. Nakamura, “Successful
Treatment of Neonatal Retroperitoneal Hemangioma with
Corticosteroid,” Journal of Pediatric Surgery, Vol. 8, No.
1, 1973, pp. 59-62.
Copyright © 2011 SciRes. OJU