Paper Menu >>
Journal Menu >>
 Open Journal of Urology, 2011, 1, 25-27 doi:10.4236/oju.2011.13007 Published Online August 2011 (http://www.SciRP.org/journal/oju) Copyright © 2011 SciRes. OJU Embolisation of Bleeding Renal Angiomyolipoma in Pregnancy Chin Hong Lim, David Mulvin Department of Urology, St. Vincent’s University Hospital, Dublin, Ireland E-mail: chinhong242002@yahoo.com Received May 10, 201 1; revised June 18, 2011; accepted June 25, 2011 Abstract Bleeding from renal angiomyolipoma in pregnancy can be catastrophic to both mother and fetus. Selective arterial embolisation is considered more superior than conventional surgery in these patients. Our case report exemplifies how a bleeding angiomyolipoma was halted with embolisation in our pregnant patient. Keywords: Selective Arterial Embolisation, Renal Angiomyolipoma, Pregnancy, Bleeding, Choristoma 1. Introduction Renal angiomyolipoma (AML) was once considered a rare tumour with the diagnosis traditionally established by histology after removal of the renal lesion, it is now recognised as a relatively common lesion with a broad range of clinical sequelae that is amenable to different management options. Recent developments in interven- tional radiology have provided new tools for diagnosing and treating this interesting con dition. 2. Case Report A 32-year-old female gravida 3, para 2 presented with left flank pain radiating to her left groin at 24 weeks gestation. Her haemoglobin dropped from 10.7 g/dL on admission to 6.9 g/dL over 24 hours. On examinations, the fundus of her uterus palpable consistent with her gestation and there was fullness and tenderness over her left renal angle. Investigation revealed haemoglobin of 10.3 g/dL, WCC 11.3 × 109, platelets 186 × 109 and nor- mal renal function (urea 2.1 µmol/l, creatin ine 49 µmol/l). Her ultrasound show ed 7 × 8 cm echogenic lesion in her left kidney with hyperechoic component suggestive of angiomyolipoma (Figure 1). She was haemodynamically stable after transfusion of 2 units of red cells. On day 3 post-admission, she developed pain and her Hb dropped from 10.7 g/dL to 8.6 g/dL. She underwent urgent MRI. But because of her claustrophobia, only T1 axial se- quences and localisers could be obtained. This confirms the presence of a large (approximately 12 cm) left-sided abdominal mass with a high signal within it consistent with fat or blood (Figure 2). The overall MR appear- ances are entirely consistent with the presumptive clini- cal diagnosis of a bleed into a left renal tumour, most likely angiomyolipoma. It was elected to proceed to em- bolisatio n of bleeding angi omyolipoma. An initial aortogram was performed via the left femo- ral artery to assess the number and location of left renal artery. Selective renal arteriography was then used to delineate the vascular anatomy of the target tumour . The feeding vessel was then selectively catheterised with microcatheter (Figure 3(a)). Embolisation was per- formed with combination of microspheres (300 - 500 microns) (Terumo Europe N.V.) and coil (3 mm) (man- ufactured by William Cook Europe) positioned in ac- tively bleeding vessel. Post-embolisation film showed excellent result. (Figure 3( b)). Following the procedure, the patient complained of left sided pleuritic chest pain and palpitations. Spiral CT revealed no evidence of pulmonary embolism and her symptoms settled with simple oral analgesia. Her repeat Haemoglobin for the next 5 days was stable and she was discharged on day 6 post-embolisati o n. The proceeding pregnancy was completely uneventful and at 40 weeks she gave birth by elective caesarean section to a normal female infant weighting 3000 g. There were no further complications during the preg- nancy or in the post-p artum period. She was reviewed on outpatient clinic 8 weeks post partum complaint of ongoing left flank pain. CT abdo- men showed a 10 × 4 × 4 cm collection in left renal bed. The lesion was not suitab le for re-embolisation and deci- sion was make to remove the left kidney. She had elective 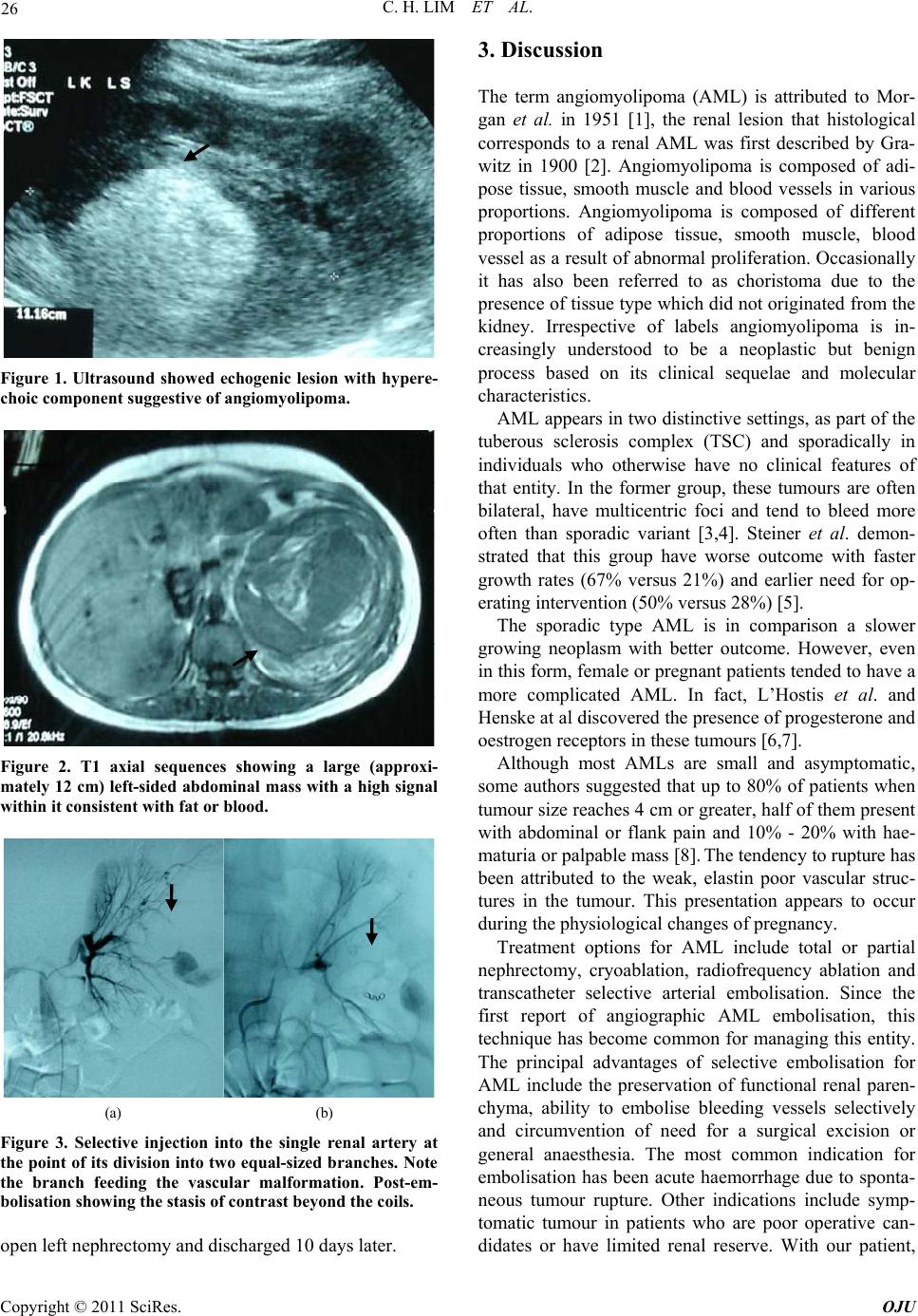 26 C. H. LIM ET AL. Figure 1. Ultrasound showed echogenic lesion with hypere- choic component suggestive of angiomyolipoma. Figure 2. T1 axial sequences showing a large (approxi- mately 12 cm) left-sided abdominal mass with a high signal within it consistent with fat or blood. (a) (b) Figure 3. Selective injection into the single renal artery at the point of its division into two equal-sized branches. Note the branch feeding the vascular malformation. Post-em- bolisation showing the stasis of contrast beyond the c oils. open left nephrectomy and discharged 10 days later. 3. Discussion The term angiomyolipoma (AML) is attributed to Mor- gan et al. in 1951 [1], the renal lesion that histological corresponds to a renal AML was first described by Gra- witz in 1900 [2]. Angiomyolipoma is composed of adi- pose tissue, smooth muscle and blood vessels in various proportions. Angiomyolipoma is composed of different proportions of adipose tissue, smooth muscle, blood vessel as a result of abnormal proliferation. Occasionally it has also been referred to as choristoma due to the presence of tissue type which did not originated from the kidney. Irrespective of labels angiomyolipoma is in- creasingly understood to be a neoplastic but benign process based on its clinical sequelae and molecular characteristics. AML appears in two distinctive settings , as part of the tuberous sclerosis complex (TSC) and sporadically in individuals who otherwise have no clinical features of that entity. In the former group, these tumours are often bilateral, have multicentric foci and tend to bleed more often than sporadic variant [3,4]. Steiner et al. demon- strated that this group have worse outcome with faster growth rates (67% versus 21%) and earlier need for op- erating intervention (50% versus 28%) [5 ]. The sporadic type AML is in comparison a slower growing neoplasm with better outcome. However, even in this form, female or pregnant patients tended to have a more complicated AML. In fact, L’Hostis et al. and Henske at al discovered the presence of progesterone and oestrogen receptors in these tumours [6,7]. Although most AMLs are small and asymptomatic, some authors suggested that up to 80% of patients when tumour size reaches 4 cm or greater, half of them present with abdominal or flank pain and 10% - 20% with hae- maturia or palpable mass [8]. The tendency to rupture has been attributed to the weak, elastin poor vascular struc- tures in the tumour. This presentation appears to occur during the physiological changes of pregnancy. Treatment options for AML include total or partial nephrectomy, cryoablation, radiofrequency ablation and transcatheter selective arterial embolisation. Since the first report of angiographic AML embolisation, this technique has become common for managing this entity. The principal advantages of selective embolisation for AML include the preservation of functional renal paren- chyma, ability to embolise bleeding vessels selectively and circumvention of need for a surgical excision or general anaesthesia. The most common indication for embolisation has been acute haemorrhage due to sponta- neous tumour rupture. Other indications include symp- tomatic tumour in patients who are poor operative can- didates or have limited renal reserve. With our patient, Copyright © 2011 SciRes. OJU 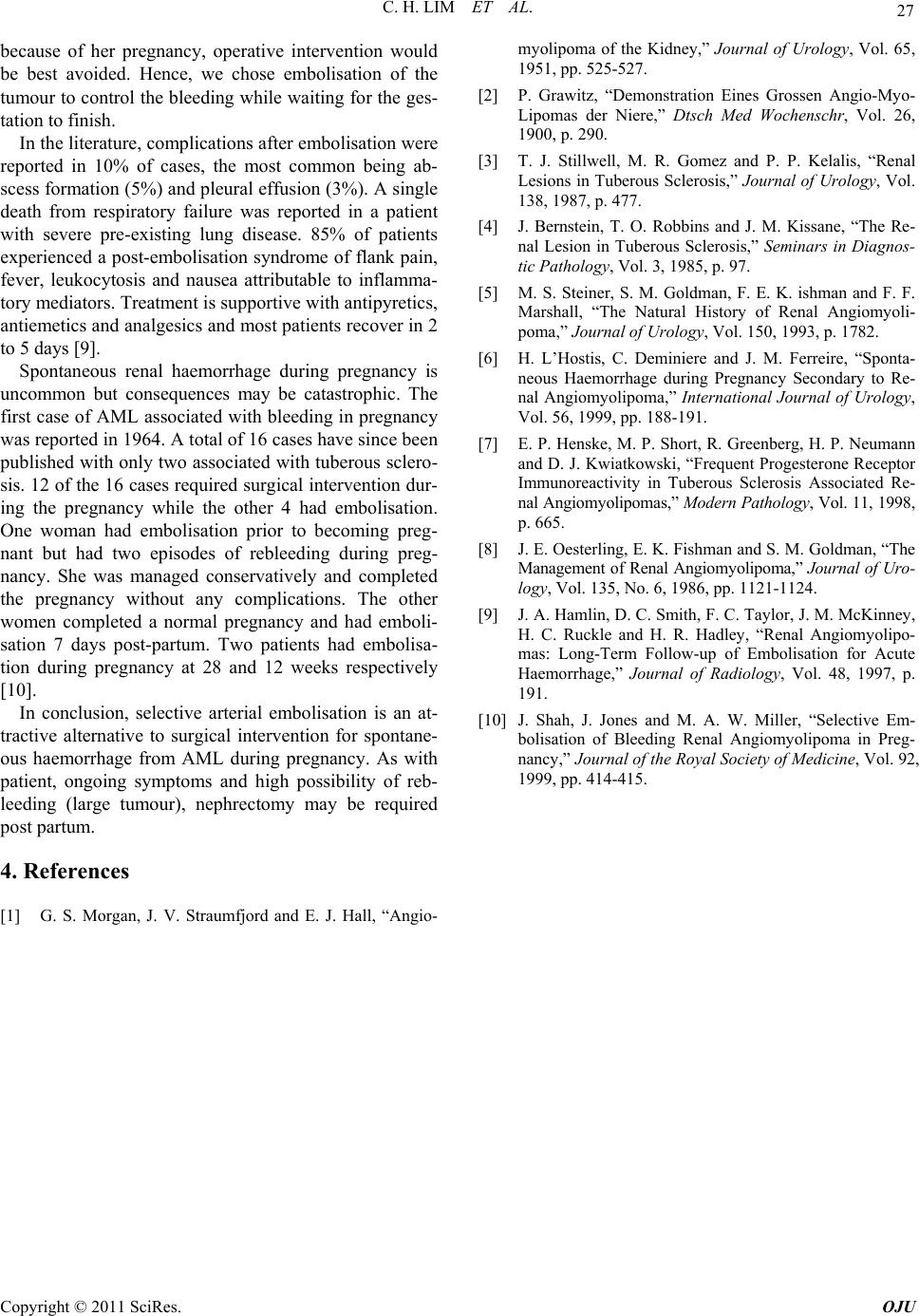 C. H. LIM ET AL. Copyright © 2011 SciRes. OJU 27 because of her pregnancy, operative intervention would be best avoided. Hence, we chose embolisation of the tumour to control the bleed ing while waiting for the ges- tation to finish. In the literature, complications after embolisation were reported in 10% of cases, the most common being ab- scess formation (5%) and pleural effusion (3%). A single death from respiratory failure was reported in a patient with severe pre-existing lung disease. 85% of patients experienced a post-embolisation syndrome of flank pain, fever, leukocytosis and nausea attributable to inflamma- tory mediators. Treatment is supportive with antipyretics, antiemetics and analgesics and most patients recover in 2 to 5 days [9]. Spontaneous renal haemorrhage during pregnancy is uncommon but consequences may be catastrophic. The first case of AML associated with bleeding in pregnancy was reported in 1964. A total of 16 cases have since been published with only two associated with tuberou s sclero- sis. 12 of the 16 cases required su rgical intervention dur- ing the pregnancy while the other 4 had embolisation. One woman had embolisation prior to becoming preg- nant but had two episodes of rebleeding during preg- nancy. She was managed conservatively and completed the pregnancy without any complications. The other women completed a normal pregnancy and had emboli- sation 7 days post-partum. Two patients had embolisa- tion during pregnancy at 28 and 12 weeks respectively [10]. In conclusion, selective arterial embolisation is an at- tractive alternative to surgical intervention for spontane- ous haemorrhage from AML during pregnancy. As with patient, ongoing symptoms and high possibility of reb- leeding (large tumour), nephrectomy may be required post partum. 4. References [1] G. S. Morgan, J. V. Straumfjord and E. J. Hall, “Angio- myolipoma of the Kidney,” Journal of Urology, Vol. 65, 1951, pp. 525-527. [2] P. Grawitz, “Demonstration Eines Grossen Angio-Myo- Lipomas der Niere,” Dtsch Med Wochenschr, Vol. 26, 1900, p. 290. [3] T. J. Stillwell, M. R. Gomez and P. P. Kelalis, “Renal Lesions in Tuberous Sclerosis,” Journal of Urology, Vol. 138, 1987, p. 477. [4] J. Bernstein, T. O. Robbins and J. M. Kissane, “The Re- nal Lesion in Tuberous Sclerosis,” Seminars in Diagnos- tic Pathology, Vol. 3, 1985, p. 97. [5] M. S. Steiner, S. M. Goldman, F. E. K. ishman and F. F. Marshall, “The Natural History of Renal Angiomyoli- poma,” Journal of Urology, Vol. 150, 1993, p. 1782. [6] H. L’Hostis, C. Deminiere and J. M. Ferreire, “Sponta- neous Haemorrhage during Pregnancy Secondary to Re- nal Angiomyolipoma,” International Journal of Urology, Vol. 56, 1999, pp. 188-191. [7] E. P. Henske, M. P. Short, R. Greenberg, H. P. Neumann and D. J. Kwiatkowski, “Frequent Progesterone Receptor Immunoreactivity in Tuberous Sclerosis Associated Re- nal Angiomyolipomas,” Modern Patholo gy, Vol. 11, 1998, p. 665. [8] J. E. Oesterling, E. K. Fishman and S. M. Goldman, “The Management of Renal Angiomyolipoma,” Journal of Uro- logy, Vol. 135, No. 6, 1986, pp. 1121-1124. [9] J. A. Hamlin, D. C. Smith, F. C. Taylor, J. M. McKinney, H. C. Ruckle and H. R. Hadley, “Renal Angiomyolipo- mas: Long-Term Follow-up of Embolisation for Acute Haemorrhage,” Journal of Radiology, Vol. 48, 1997, p. 191. [10] J. Shah, J. Jones and M. A. W. Miller, “Selective Em- bolisation of Bleeding Renal Angiomyolipoma in Preg- nancy,” Journal of the Royal Society of Medicine, Vol. 92, 1999, pp. 414-415. |