 Surgical Science, 2011, 2, 252-256 doi:10.4236/ss.2011.25056 Published Online July 2011 (http://www.SciRP.org/journal/ss) Copyright © 2011 SciRes. SS Loop Ileostomy and Colostomy—A Comparison between Supporting Plastic Rods and Epicutaneous or Subcutaneous Silicon Drains Mike Ralf Langenbach1, Ste fan Sauerl and 2, Eiyad Issa1, Claudia Nitschke3, Hubert Zirngibl3 1Helios St. Elisabeth Klinik Oberhausen, Department of S urgery II, University of Witten/Herdecke, Oberhausen, Ger many 2Institute for Research in Operative Medicine (IFOM), University Witten/Herdecke, Cologne, Germany 3Helios Klinikum Wuppertal, Department of Surgery II, University of Witten/Herdecke, Wuppertal, Germany E-mail: mike-ralf.langenbach@helios-kliniken.de Received March 21, 20 1 1; revised May 23, 2011; accepted J un e 1, 2011 Abstract Purpose: Beside the conventional plastic rods, different techniques and materials have been proposed in the last years to prevent the loop from retraction into the abdominal cavity. The aim of this retrospective com- parative study was to assess three different techniques of loop support. Methods: The study included 65 pa- tients who had loop ileostomy or colostomy formed. Depending on the decision of the operating surgeon, one of three techniques was chosen to fixate the stoma loop: an epicutaneous plastic rod (group 1, n = 14), an epicutaneous suture-fixated silicone drain (group 2, n = 27), or a subcutaneous silicone drain (group 3, n = 24). Results: The majority of patients (85%) received loop ileostomy. Pain intensity was significantly (p = 0.0014) different among the three groups. A total of 19 patients (30%) suffered a complication. There was a tendency towards less complications if the stoma was secured by a silicone drain with epicutaneous fixation. Comfort with stoma care was significantly different, with group 3 experiencing the best results. Conclusions: Using a subcutaneously tunnelled silicon drain as a stoma bridge results in less complications, less pain and higher satisfaction as compared to the conventional plastic rod. Conventional plastic rods should be avoided. Keywords: Ileostomy, Colostomy, Drains, Plastic Rods 1. Introduction Loop ileostomy and colostomy are frequently indicated in patients with acute or complicated intestinal diseases, such as acute neoplastic obstruction, inflammatory steno- sis or perforation. Irregardless of the differences between ileostomy and colostomy [1-3], stomas usually cause a number of medical but also psychosocial problems. In two of the largest studies on this problem [4,5], local complications of minor severity were noted in one third of patients. According to Cottam, et al. [4], the most frequent complication was retraction of the stoma, which occurred in one quarter of patients. However, this figure needs to be interpreted with caution, because the defini- tion of retraction is not straightforward. Since many years plastic rods have been used to sup- port a loop stoma and to prevent the loop from falling back into the abdominal cavity [6-8]. However, the use of rigid plastic rods is not without complicatio ns, mainly because the rod lies on the skin surface for one or two weeks after surgery, which can lead to skin maceration and local infection. Dissatisfaction with plastic rods is highly prevalent as evidenced by the large number of alternative techniques that were proposed in more recent years [9-16]. In most of these articles, the bridge which supported the stoma limbs was reinforced with a softer material, such as a Jackson-Pratt drain, a suction drain tube, or a Penrose drain. So me surgeons have even ques- tioned whether the use of supporting br idges is necessar y at all [17,18]. Based on clinical experience, the technique of secure- ing loop ileostomies and colostomies at the authors’ in- stitution has been variable during th e last years. The aim of this retrospective study therefore was to assess which technique of loop support provided the lowest rate of complications and the highest level of satisfaction for  M. R. LANGENBACH ET AL. 253 stoma therapist and patient. 2. Material and Methods Consecutive patients with a first stoma between June 2008 and December 2009 were studied. Stoma construc- tion followed either an emergency or an elective surgical procedure. Depending on the decision of the operating surgeon, one of three stoma techniques was chosen: a conventional epicutaneous plastic rod (group 1), an epicutaneous suture-fixated silicone drain (group 2), or a silicone drain placed in a subcutaneous tunnel (group 3). The selection of surgical technique depended more on the surgeon’s personal expertise than on the patient’s characteristics. The steps in performing a loop colo- or ileostomy with a suprafascial bridge device were similar to those gener- ally described in international textboo ks. After a suitable incision in the abdominal wall had been made, the colic or ileic loop was gently pulled through the opening and a small incision was made in the mesentery. In group 1, a conventional plastic rod (ConvaTec®, Coloplast Inc., Hamburg, Germany) measuring 7 or 10 cm in length was placed through the mesenteric window. At both ends of the rod small wings were opened, so that the rod could not slip through the mesentery. In groups 2 and 3, a 21 Charrière silicone drain was used. Both ends were pointed to ease tissue penetration. In group 2, after placement through the mesentery, the ends of the silicon drain were fixed with nonresorbable polyamid sutures (Ethilone, 3.0; Ethicon, Inc.) to the skin at the incisional site. The stitches were inside the range of the stoma appliance. When the surgeon decided to secure the stoma with a subcutaneous silicone drain (group 3), the silicone drain was cut to a length of about 20 cm. After being placed through the mesentery, both ends of the drain were subcutaneously tunnelled, were brought out and fixed with a stitch. Entry and exit point of the drain were just beyond the circumference of the stoma flange. Finally, both end of the drain were short- ened to the level of the skin. Whilst in the hospital the patients were regularly re- viewed and stomata were assessed by a surgeon and stoma therapist. Using standardized forms, we recorded demographic characteristics, surgical indication, and type of surgery. At the first, third, fifth and tenth postopera- tive day, the severity of local pain (u sing a 0 to 10 visual analogue scale [VAS]), the occurrence of local compli- cations, and the level of satisfaction of stoma therapist and patient were recorded. The definition of complica- tions was adapted from other studies and required the presence of patient-reported symptoms, or the necessity of specific therapy (local or systemic). Follow up was continued until stoma support was removed, which took place between the seventh and tenth postoperative day. All data collected in the patients’ charts were retrospect- tively reviewed and analysed. Statistical Analysis Differences in baseline and outcome parameters between the three groups were statistically assessed using analysis of variance (ANOVA) or chi square testing. In order to account for the fact that pain scores represented repeated measures of the same individual, these were analyzed with a general linear model followed by post hoc Tukey tests. Significance was defined as a p-value smaller than 0.05. 3. Results Among the 65 patients, there were 55 (85%) loop ileo- stomies and 10 (15%) loop colostomies. In colostomy patients, a plastic rod was used more frequently. With regard to other baseline variables, the groups were more or less comparable (Table 1). As shown in Figure 1, pain was clearly different among the three groups (p = 0.014). Group-wise com- parisons indicated that pain was significantly lower in the group with subcutaneous silicone drains than in each of the other two groups: p = 0.008 vs. plastic rod and p < 0.001 vs. silicone drain on skin. No patient required an- algesics because of local pain. A total of 19 patients (29%) suffered a complication. There were slightly less complications in patients who had their stoma secured by a superficially placed silicone drain (Table 2), but this difference was not significant. However, the severest complications (arrosion of the in- testine) were all seen exclusively in the group with con- ventional plastic rods. All wound infections in the group with subcutaneously tunnelled silicon drains were super- ficial and mild. From the viewpoint of the stoma therapist, comfort and ease of stoma care was significantly different among the groups, as the group with subcutaneously placed sili- con drains showed the best results. Since entry and exit site of the silicon drain in this group were outside the diameter of the stomal flange, changing the stoma bag did not interfere with any type of rod or drain. 4. Discussion The creation of a loop ileo- or colostomy strongly influ- ences the patients’ quality of life after an operation. Fur- thermore, patient cooperation is necessary for correct stoma care. Therefore, it is essential that no complication decreases the patients' trust in the normal functioning of Copyright © 2011 SciRes. SS  M. R. LANGENBACH ET AL. Copyright © 2011 SciRes. SS 254 Table 1. Demographic baseline characteristics. Conventional plastic rod Silicon drain on skin surfaceSilicon drain with subcutaneous tunnel P-value Number of patient s 14 27 24 Age (in years) with ra n ge 63 (16) 31 - 81 66 (12) 27 - 86 73 (11) 40 - 87 0.028a) Gender (proport i o n males) 9 (64%) 15 (56%) 15 (63%) 0.82b) Underlying disease Rectal cancer Colon cancer Intestinal ischemia Inflammatory bowel disease Sacral pressure ulcer Diverticulitis Other c) 6 (43%) 1 (7%) 2 (14%) 0 0 1 (7%) 4 (27%) 16 (59%) 3 (11%) 3 (11%) 2 (7%) 1 (4%) 1 (4%) 1 (4%) 16 (67%) 4 (17%) 1 (4%) 1 (4%) 2 (8%) 0 0 0.15b) Type of stoma Loop ileostomy Loop colostomy 11 (79%) 3 (21%) 24 (89%) 3 (11%) 20 (83%) 4 (17%) 0.05b) Data are means ± standard deviations (with ranges) or counts (with percentages); a) by ANOVA, b) by Chi square test, c) This category in cluded rectal i mpale- ment injury, advanced prostatic cancer, rectocele, complicated ileus, and multiple sclerosis. Table 2. Clinical results. Conventional plastic rod Silicon drain on skin surface Silicon drain with subcutaneous tunnel P-value Number of patient s 14 27 24 Any complication 7 (50%) 8 (30%) 4 (17%) 0.41 Local complications Arrosion of intestine Partial necrosis of intestine Intestinal malperfusion Fixation suture torn out Infection at drain entry site Small stoma prolapse Small parastomal hernia Local swelling 5c) 1 1 2 1 1 1 3 2 1 1 NA Comfort of stoma care Good Average Bad 2 (14%) 5 (36%) 7 (50%) 12 (44%) 9 (33%) 6 (22%) 24 (100%) 0 0 0.001 Data are means ± standard d eviations (with ranges); a) by ANOVA, b) by Chi square t est, c) On day 1, 3 (three cases) and 5 after stoma creation. the stoma. In this study, complications were more fre- quent and more severe in patients with a conventionally secured stoma. In order to avoid arrosion of the intestinal loop, the use of softer material for the stoma bridge ap- pears necessary. Nevertheless, complications were still quite common in the two groups, where a silicon drain was used instead of a plastic rod. This shows the need for further improvements in surgical techniques. The complication rate of this study (29%) is well in line with previous research [4,19-26]. In a large registry study, Cottam, et al. identified 34% of 3970 stomas as problematic [4]. In that study, type of stoma and gender of the patient were described as significant risk factors, but also the height of the stoma was predictive for com- plications. In our experience, securing the stoma loop with a silicon drain effectively prevented any retraction of the loop into the wound. Although stoma height is Figure 1. Local pain on day 1, 3, 5, and 7 after different type s of stoma creation Data are means with error bars indicat- ing one standard error.  M. R. LANGENBACH ET AL. 255 difficult to measure quantitatively, the subcutaneous po- sition of a silicon drain is fully sufficient to support the loop, which then guarantees for correct emptying of in- testinal contents into the stoma appliance. Using a subcutaneously tunnelled suction drain as a stoma bridge was first described in 2008 by Harish [13]. As the two main advantages of this technique, he con- sidered the quick availability of suction drains in operat- ing theatre and the ease of stoma care device application. In the present study, surg ical techniques were exactly the same as described by Harish, except for the fact that he used tubes of 16 or 18 French, whereas a calibre of 21 Frenc h was pref err ed b y us . Th is difference can probably be best explained by the larger body size of Europeans as compared to Indians, in whom Harish developed the technique. Already in 1984, Jenkinson, et al. proposed to use the subcutaneous layer for placement of the stoma bridge [27]. In a more recent study, Branco, et al. [12] im- planted a conventional plastic bridge device in the sub- cutaneous tissue. In this technique, there is no need for additional skin incisions, which clearly reduces the risk of wound infection. Among the 19 cases reported by Branco, et al., there was not a single infection, but ap- parently pain was a problem, as two patients requested analgesics. Of note, pain during bridge removal was not reported in the study by Branco, et al., because the plas- tic rod remained in place until stoma reversal. However, a permanent plastic rod in the abdominal wall may cause discomfort to the patient. Since silicone is a softer mate- rial than plastic, pain was clearly reduced in the present study. It is quite interesting that a silicon drain causes less pain when subcutaneously tunnelled than being placed on the skin. Apparently, the stitches for securing the drain must also be considered a potential source of pain, because the intestinal loop may pull on these stitches. An important strength of the present study is that it represents a comparative design including three com- parison groups and assessment of patient-reported out- comes. Although the assignment of patients into the three groups was not randomised, the potential for selection bias was very small, because during the study period most surgeons performed only one of the three tech- niques. Usually, evidence derived from prospectively controlled trials allows for more valid conclusions than do case series without a control group. To some extent the lack of comparative studies is certainly responsible for the large variety in surgical techniques in this field and the lack of a consensus on the best technique [28]. 5. Conclusions In summary, our data implicate that a subcutaneously tunnelled silicon drain provides the lowest rate of com- plications and pain and the highest level of satisfaction for patient and stoma therapist. Plastic rods should be avoided. 6. References [1] A. W. Gooszen, R. H. Geelkerken, J. Hermans, M. B. Lagaay and H. G. Gooszen, “Quality of Life with a Tem- porary Stoma: Ileostomy vs. Colostomy,” Diseases of the Colon & Rectum, Vol. 43, No. 5, 2000, pp. 650-655. doi:10.1007/BF02235581 [2] N. S. Williams, D. G. Nasmyth, D. Jones and A. H. Smith, “Defunctioning Stomas: A Prospective Controlled Trial Comparing Loop Ileostomy with Loop Transverse Colos- tomy,” British Journal of Surgery, Vol. 73, No. 7, 1986, pp. 566-570. doi:10.1002/bjs.1800730717 [3] S. D. Wexner, D. A. Taranow, O. B. Johansen, F. Itzko- witz, N. Daniel, J. J. Nogueras and D. G. Jagelman, “Loop Ileostomy is a Safe Option for Fecal Diversion,” Diseases of the Colon & Rectum, Vol. 36, No. 4, 1993, pp. 349-354. doi:10.1007/BF02053937 [4] J. Cottam, K. Richards, A. Hasted and A. Blackman, “Results of a Nationwide Prospective Audit of Stoma Complications within 3 Weeks of Surgery,” Colorectal Disease, Vol. 9, No. 9, 2007, pp. 834-838. doi:10.1111/j.1463-1318.2007.01213.x [5] J. J. Park, A. Del Pino, C. P. Orsay, R. L. Nelson, R. K. Pearl, J. R. Cintron and H. Abcarian, “Stoma Complica- tions: The Cook County Hospital Experience,” Diseases of the Colon & Rectum, Vol. 42, No. 12, 1999, pp. 1575 -1580. doi:10.1007/BF02236210 [6] S. M. Poticha, “A New Technic for Loop Colostomy with Use of a Plastic Bridge,” American Journal of Surgery, Vol. 127, No. 5, 1974, pp. 620-621. doi:10.1016/0002-9610(74)90333-X [7] J. M. Corman and D. B. Odenheimer, “Securing the Loop—Historic Review of the Methods Used for Creat- ing a Loop Colostomy,” Diseases of the Colon & Rectum, Vol. 34, No. 11, 1991, pp. 1014-1021. doi:10.1007/BF02049967 [8] P. M. Go, N. H. Vaessen, C. J. van Duin and J. Lens, “A Plastic Rod to Facilitate Longitudinal Incision of the Bowel. An Inexpensive and Practical Device,” Diseases of the Colon & Rectum, Vol. 29, No. 10, 1986, p. 674. doi:10.1007/BF02560338 [9] R. A. Cochrane, D. J. Hay and A. F. Jones, “A Better Bridge for Loop Stomas,” British Journal of Surgery, Vol. 83, No. 3, 1996, p. 365. doi:10.1002/bjs.1800830322 [10] R. J. Fitzgibbons, Jr., G. D. Schmitz and R. T. Bailey, Jr., “A Simple Technique for Constructing a Loop En- terostomy which Allows Immediate Placement of an Ostomy Appliance,” Surgery, gynecology & obstetrics, Vol. 164, No. 1, 1987, pp. 78-80. [11] S. W. Atkinson and P. G. Bentley, “Subcutaneous Bridge Support for Defunctioning Loop Colostomy,” British Journal of Surgery, Vol. 83, No. 10, 1996, p. 1458. doi:10.1002/bjs.1800831042 Copyright © 2011 SciRes. SS 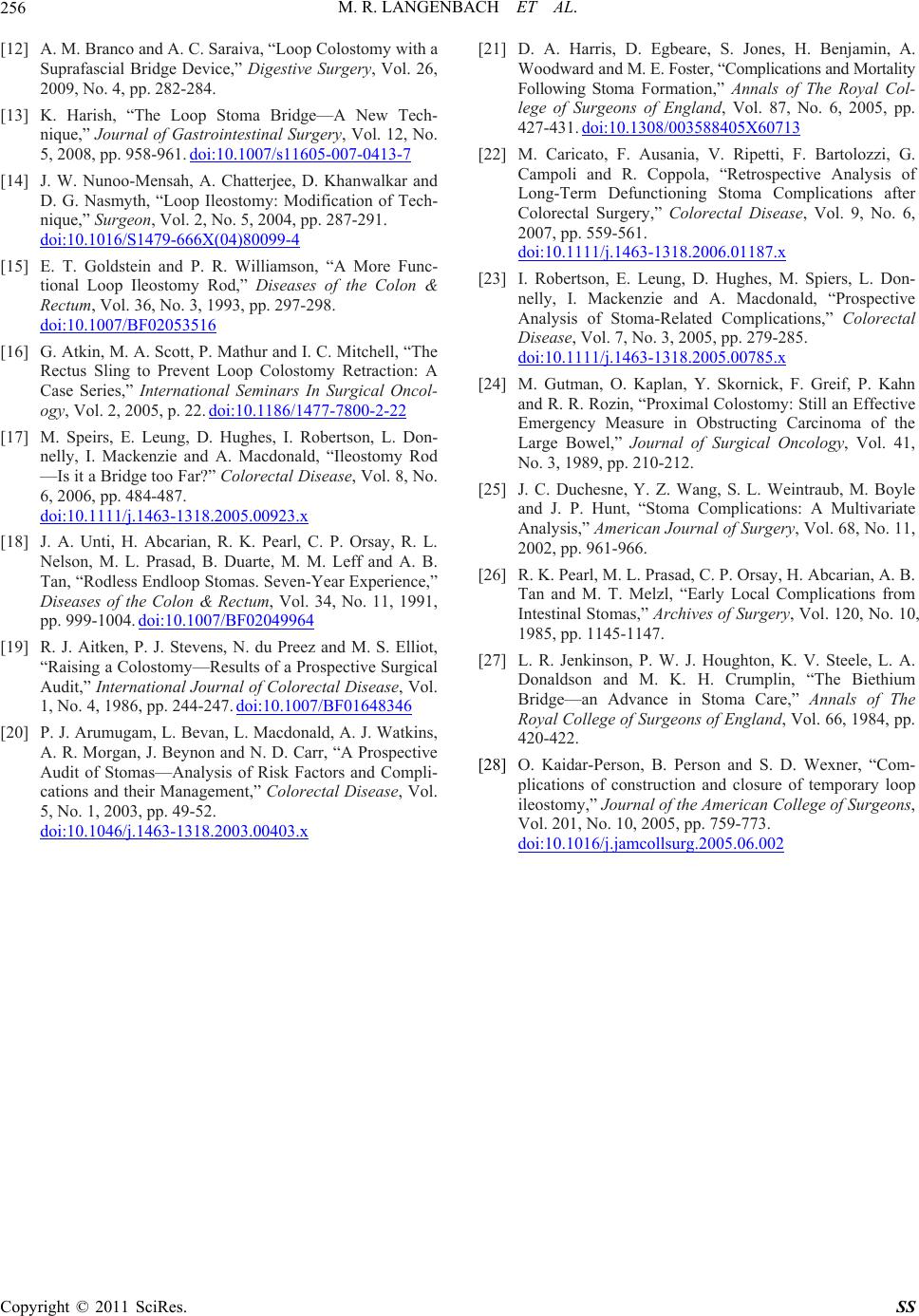 M. R. LANGENBACH ET AL. Copyright © 2011 SciRes. SS 256 [12] A. M. Branco and A. C. Saraiva, “Loop Colostomy with a Suprafascial Bridge Device,” Digestive Surgery, Vol. 26, 2009, No. 4, pp. 282-284. [13] K. Harish, “The Loop Stoma Bridge—A New Tech- nique,” Journal of Gastrointestinal Surgery, Vol. 12, No. 5, 2008, pp. 958-961. doi:10.1007/s11605-007-0413-7 [14] J. W. Nunoo-Mensah, A. Chatterjee, D. Khanwalkar and D. G. Nasmyth, “Loop Ileostomy: Modification of Tech- nique,” Surgeon, Vol. 2, No. 5, 2004, pp. 287-291. doi:10.1016/S1479-666X(04)80099-4 [15] E. T. Goldstein and P. R. Williamson, “A More Func- tional Loop Ileostomy Rod,” Diseases of the Colon & Rectum, Vol. 36, No. 3, 1993, pp. 297-298. doi:10.1007/BF02053516 [16] G. Atkin, M. A. Scot t, P. Mathur a nd I. C. Mitche ll, “The Rectus Sling to Prevent Loop Colostomy Retraction: A Case Series,” International Seminars In Surgical Oncol- ogy, Vol. 2, 2005, p. 22. doi:10.1186/1477-7800-2-22 [17] M. Speirs, E. Leung, D. Hughes, I. Robertson, L. Don- nelly, I. Mackenzie and A. Macdonald, “Ileostomy Rod —Is it a Bridge too Far?” Colorectal Disease, Vol. 8, No. 6, 2006, pp. 484-487. doi:10.1111/j.1463-1318.2005.00923.x [18] J. A. Unti, H. Abcarian, R. K. Pearl, C. P. Orsay, R. L. Nelson, M. L. Prasad, B. Duarte, M. M. Leff and A. B. Tan, “Rodless Endloop Stomas. Seven-Year Experience,” Diseases of the Colon & Rectum, Vol. 34, No. 11, 1991, pp. 999-1004. doi:10.1007/BF02049964 [19] R. J. Aitken, P. J. Stevens, N. du Preez and M. S. Elliot, “Raising a Colostomy—Results of a Prospective Surgical Audit,” International Journal of Colorectal Disease, Vol . 1, No. 4, 1986, pp. 244-247. doi:10.1007/BF01648346 [20] P. J. Arumugam, L. Bevan, L. Macdonald, A. J. Watkins, A. R. Morgan, J. Beynon and N. D. Carr, “A Prospective Audit of Stomas—Analysis of Risk Factors and Compli- cations and their Management,” Colorectal Disease, Vol. 5, No. 1, 2003, pp. 49-52. doi:10.1046/j.1463-1318.2003.00403.x [21] D. A. Harris, D. Egbeare, S. Jones, H. Benjamin, A. Woodward and M. E. Foster, “ Complicatio ns and M or ta lity Following Stoma Formation,” Annals of The Royal Col- lege of Surgeons of England, Vol. 87, No. 6, 2005, pp. 427-431. doi:10.1308/003588405X60713 [22] M. Caricato, F. Ausania, V. Ripetti, F. Bartolozzi, G. Campoli and R. Coppola, “Retrospective Analysis of Long-Term Defunctioning Stoma Complications after Colorectal Surgery,” Colorectal Disease, Vol. 9, No. 6, 2007, pp. 559-561. doi:10.1111/j.1463-1318.2006.01187.x [23] I. Robertson, E. Leung, D. Hughes, M. Spiers, L. Don- nelly, I. Mackenzie and A. Macdonald, “Prospective Analysis of Stoma-Related Complications,” Colorectal Disease, Vol. 7, No. 3, 2005, pp. 279-285. doi:10.1111/j.1463-1318.2005.00785.x [24] M. Gutman, O. Kaplan, Y. Skornick, F. Greif, P. Kahn and R. R. Rozin, “Proximal Colostomy: Still an Effective Emergency Measure in Obstructing Carcinoma of the Large Bowel,” Journal of Surgical Oncology, Vol. 41, No. 3, 1989, pp. 210-212. [25] J. C. Duchesne, Y. Z. Wang, S. L. Weintraub, M. Boyle and J. P. Hunt, “Stoma Complications: A Multivariate Analysis,” American Journal of Surgery, Vol. 68, No. 11, 2002, pp. 961-966. [26] R. K. Pearl, M. L. Prasad, C. P. Orsay, H. Abcarian, A. B. Tan and M. T. Melzl, “Early Local Complications from Intestinal Stomas,” Archives of Surgery, Vol. 120, No. 10, 1985, pp. 1145-1147. [27] L. R. Jenkinson, P. W. J. Houghton, K. V. Steele, L. A. Donaldson and M. K. H. Crumplin, “The Biethium Bridge—an Advance in Stoma Care,” Annals of The Royal College of Surgeons of England, Vol. 66, 1984, pp. 420-422. [28] O. Kaidar-Person, B. Person and S. D. Wexner, “Com- plications of construction and closure of temporary loop ileostomy,” Journal of the American College of Surgeons, Vol. 201, No. 10, 2005, pp. 759-773. doi:10.1016/j.jamcollsurg.2005.06.002
|