J. BARNES ET AL.
374
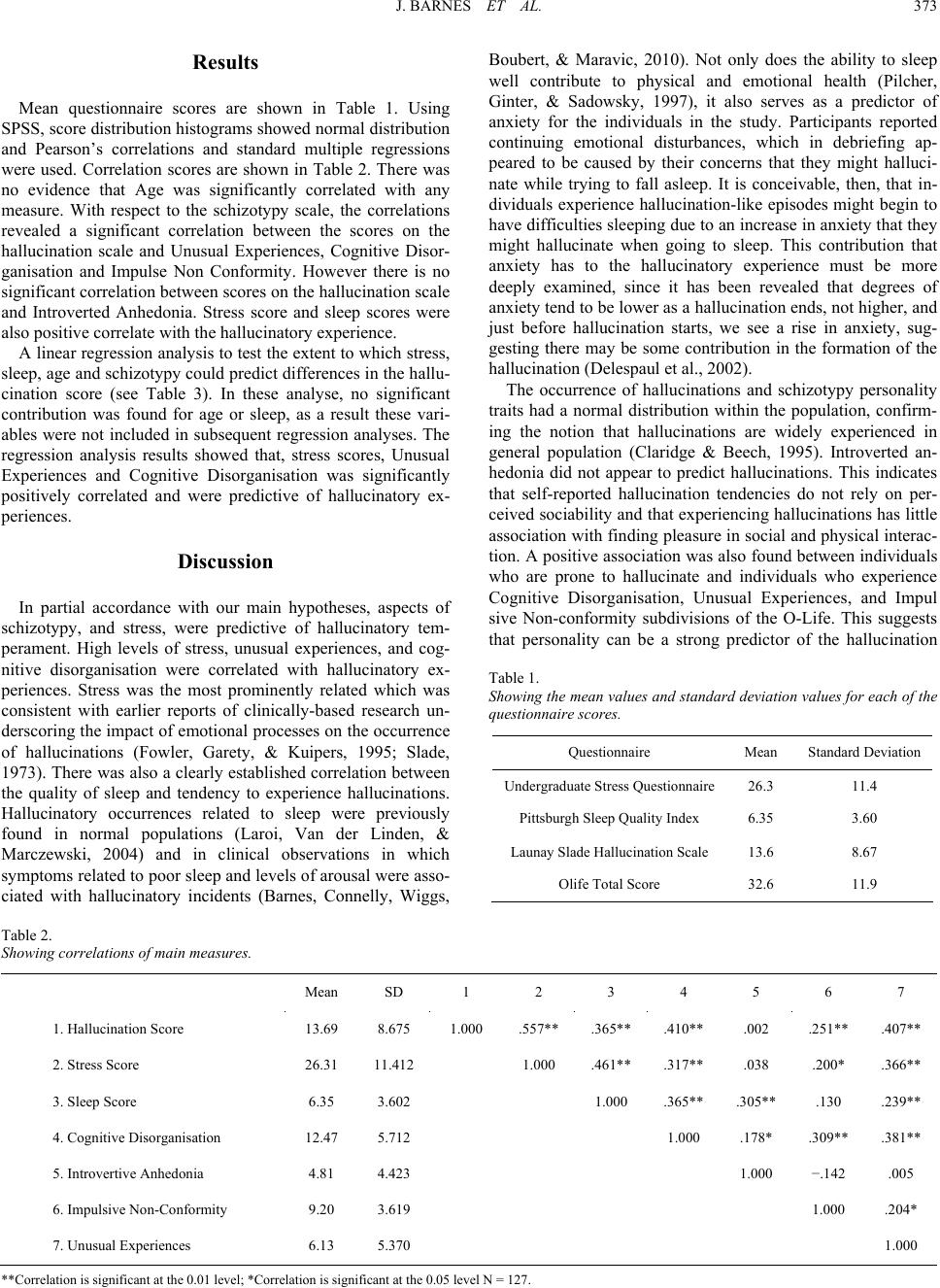
Table 3.
Linear regression analysis for hallucinatory experiences as measures
by Launay Slade Hallucination Scale.
Beta t
Stress Score .422 5.433**
Unusual Experiences .163 2.054*
Impulsive Non Conformity .065 .855
Introvertive Anhedonia −.041 −.563
Cognitive Disorganisation .201 2.439*
F (5,121) = 16.14; R-squared = 0.406; Adjusted R-squared = 0.376; **Significant
at the 0.01 level; *Significant at the 0.05 level.
phenomenon and supports previous work that found a similar
relationship (Laroi & Van der Linden, 2005). The impulsive
non-conformity was found to correlate with the hallucination
scores but not to be predictive for hallucinations in the regres-
sion calculations. This finding may be explained with reference
to the shared variance between the O-LIFE dimensions, so that
when the effects of the other three dimensions had been taken
into account, impulsive non conformity was not predictive.
Thus people who experience hallucinations would be no more
likely than their peers to have unstable mood, or display disor-
ganized and socially inappropriate behaviour.
Overall, this study was able to demonstrate that stress and
schizotypy were able to account for variance in hallucination
scores. But we must observe that, even though we observed
consistent relationships, when we consider predictor variables,
there were other factors that appeared to be connected to hallu-
cinations when isolated and examined. This means it is possible
that, even though schizotypy and stress levels forecast halluci-
nations, there are obviously other individual differences, like
motivation and awareness for instance, that must be taken into
account. There were also a number of limitations which need be
acknowledged before an examination of the implications of this
study. The size of the sample was relatively small, and the al-
location of gender was not equal. Also, the most prominent
correlations might be partly the result of overlapping methods,
simply because self-reported measures forecast self-report
measures. The discovery that the hallucinations were not pre-
dicted by the Introvertive Anhedonia scale may be a reflection
of the negative facets of psychosis and consists of items that
evaluate anhedonia when socialising and suggests that with-
drawal from the social environment and being depressed are not
major factors in experiencing hallucinations.
In conclusion the findings of this study suggest that the lev-
els of stress and anxiety experienced by the participants were
the most influential predictors of a tendency to hallucinate.
Consequently, future investigations in this area might consider
rigorously examining the emotional predictors of a person’s
tendency to have hallucinations. This could involve more accu-
rate measures of stress levels, for instance, testing the cortisol
levels, as well as conducting interviews, and implementing
daily stress diaries maintained by the participant. In addition to
offering insight into the hallucinatory experience, it may also
shed light on the extent to which a person’s level of anxiety has
an impact on their tendency to have hallucinations.
References
Barnes, J., Connelly, V., Wiggs, L., Boubert, L., & Maravic, K. (2010).
Sleep patterns in Parkinson’s disease patients with visual hallucina-
tions. International J o ur n a l o f N e ur oscience, 120, 564-569.
doi:10.3109/00207454.2010.494790
Barnes, J., & David, A. S. (2001). Visual hallucinations in Parkinson’s
disease: A review and phenomenological survey. Journal of Neurol-
ogy, Neurosurgery & Psychiatry, 70, 727-733.
doi:10.1136/jnnp.70.6.727
Bentall, R. P. (1990). The illusion of reality: A review and integration
of psychological research on hallucinations. Psychological Bulletin,
107, 82-95. doi:10.1037/0033-2909.107.1.82
Barrett, T. R., & Etheridge, J. B. (1992). Verbal hallucinations in nor-
mals. I: People who hear voices. Applied Cognitive Psychology, 6,
379-387. doi:10.1002/acp.2350060503
Claridge, G., & Beech, T. (1995). Fully and quasi-dimensional con-
structions of schizotypy. In A. Raine, T. Lencz and S. A. Mednick
(Eds.), Schizotypal personality. Cambridge: Cambridge University
Press. doi:10.1017/CBO9780511759031.010
Claridge, G., Clark, K., & Davis, C. (1997). Nightmares, dreams, and
schizotypy. British Journal of Clinical Psychology, 36, 377-386.
doi:10.1111/j.2044-8260.1997.tb01245.x
Costa, P. T. Jr., & McCrae, R. R. (1992). NEO PI-R professional man-
ual. Odessa, FL: Psychological Assessment Resources, Inc.
Crandall, C. S., Preisler, J. J., & Aussprung, J. (1992). Measuring life
event stress in the lives of college students: The Undergraduate
Stress Questionnaire (USQ). Journal of Behavioral Medicine, 15,
627-662. doi:10.1007/BF00844860
Delespaul, P., DeVries, M., & Van Os, J. (2002). Determinants of oc-
currence and recovery from hallucinations in daily life. Social Psy-
chiatry and Psychiatric Epide m i o l o gy, 37, 97-104.
doi:10.1007/s001270200000
Fowler, D., Garety, P. A., & Kuipers, L. (1995). Cognitive behaviour
therapy for psychosis: Theory a nd practice. Chichester: Wiley.
Freeman, D., & Garety, P. A. (2003). Connecting neurosis and psycho-
sis: The direct influence of emotion on delusions and hallucinations.
Behaviour Research and Therapy, 41, 923-947.
doi:10.1016/S0005-7967(02)00104-3
Fuller, K. H., Waters, W. F., Binks, P. G., & Anderson, T. (1997).
Generalized anxiety and sleep architecture: A polysomnographic in-
vestigation. Sleep, 20, 370-376.
Johns, L. C. (2005). Hallucinations in the general population. Current
Psychiatry Reports, 7, 162-167. doi:10.1007/s11920-005-0049-9
Johns, L. C., & Van Os, J. (2001). The continuity of psychotic experi-
ences in the general population. Clinical Psychology Review, 21,
1125-1141. doi:10.1016/S0272-7358(01)00103-9
Kirmil-Gray, K., Eagleston, J. R., Gibson, E., & Thoresen, C. E. (1984).
Sleep disturbance in adolescents: Sleep quality, sleep habits, beliefs
about sleep, and daytime functioning. Journal of Youth and Adoles-
cence, 13, 375-384. doi:10.1007/BF02088636
Laroi, F., & Van der Linden, M. (2005). Metacognitions in proneness
towards hallucinations and delusions. Behaviour Research and
Therapy, 43, 1425-1441. doi:10.1016/j.brat.2004.10.008
Laroi, F., Van der Linden, M., & Marczewski, P. (2004). The effects of
emotional salience, cognitive effort and meta-cognitive beliefs on a
reality monitoring task in hallucination-prone subjects. British Jour-
nal of Clinical Psychology, 43, 221-233.
doi:10.1348/0144665031752970
Launay, G., & Slade, P. (1981). The measurement of hallucinatory
predisposition in male and female prisoners. Personality and Indi-
vidual Differences, 2, 221-234. doi:10.1016/0191-8869(81)90027-1
Medeiros, A. L. D., Mendes, D. B. F., Lima, P. C. F., & Araujo, J. F.
(2001). The relationships between sleep-wake cycle and academic
performance in medical students. Biological Rhythm Research, 32,
263-270. doi:10.1076/brhm.32.2.263.1359