 International Journal of Clinical Medicine, 2011, 2, 318-324 doi:10.4236/ijcm.2011.23055 Published Online July 2011 (http://www.SciRP.org/journal/ijcm) Copyright © 2011 SciRes. IJCM Maternal Smoking during Pregnancy and Sudden Infant Death Using the National Maternal and Infant Health Survey: A Case-Case Study Kathleen Franciska Brookfield1, James Dean Wilkinson1, Barbara Luke2, Kristopher Arheart1, Eleni Sfakianaki1 1Miller School of Medicine, University of Miami, Miami, USA; 2Michigan State University, East Lansing, USA. Email: kbrookfield@med.miami.edu Received January 12th, 2011; revised March 1st, 2011; accepted April 1st, 2011. ABSTRACT We utilized data from the National Maternal and Infant Health Survey (NMHIS) to analyze the risk of SIDS and other infant deaths among women who smoke during pregnancy adjusting for potentially modifiable risk factors such as sec- ondhand smoke exposure and breastfeeding. The following variables were assessed with respect to risk for SIDS and other infant deaths: smoking exposure, level of education, infant and maternal age, infant and maternal birthweight, maternal BMI, gender, secondhand smoke exposure, breast feeding, prenatal vitamins, WIC, multiple gestation, sleep apnea monitor prescription, sleep apnea incidents and maternal alcohol use. Univariate analysis and multivariate lo- gistic regression were performed to identify variables significantly associated with the odds of mortality from SIDS. Analysis utilized weighted estimates using SUDAAN 9.0.0 to adjust for design effects. A p-value < 0.01 was cons idered statistically significant. Women who smoked during pregnancy were 1.83 times more likely to give birth to an infant that died from SIDS versus some other cause of death, OR (95%) = 1.83(1.33, 2.51). Other Race infants and Black in- fants were more likely to suffer SIDS mortality than White infants, but the result was not significant in the fina l model. Other modifiable risk factors, such as secondhand smoke exposure and breast feeding, were not significant predictors of SIDS mortality. Independent o f sociod emo graph ic va riables and o ther poten tial risk fa cto rs for SIDS death, ma tern al smoking was associated with an increased risk of SIDS death versus other death. This study highlights the importance of screening all pregnant women for tobacco use and emphasizes the importance of smoking cessation to decrease the risk of infant death from SIDS. Keywords: Sudden Infant Death, Smoking, Pregnancy, Passive Smoking, Breastfeeding 1. Introduction Sudden Infant Death Syndrome (SIDS) is the leading cause of postneonatal death among all racial and ethnic groups, representing nearly one-third of such deaths. The incidence of SIDS peaks in the second or third month of life, and subsequently decreases over the first year of life. Two components of cigarette smoke poten- tially responsible for a role in SIDS pathophysiology are carbon monoxide (CO) and nicotine. These toxins, which cross the placental barrier, have been demon- strated to alter the physiologic development of organs and tissues most susceptible to hypoxia damage, includ- ing the brain and heart in animal models [1-4]. Altered autonomic nervous system function has been described in infants born to mothers who smoked during preg- nancy [5-7]. It has been hypothesized that CO exposure from maternal smoking may have an effect on postnatal electrophysiological remodeling which could predispose the infant heart to fatal arrythmias [3]. Exposure to CO in concentrations comparable to that of human smokers induced a statistically significant delay in action poten- tial (AP) duration in a rat model [3]. The potential effect of CO exposure on AP duration is a plausible explana- tion for an arrhythmia resulting in sudden death. In addition to CO exposure, nicotine exposure has also been implicated as a key cigarette component re- lated to the cardiorespiratory events characteristic of SIDS [8]. Although not associated with restricting uter- ine blood flow, the cardiovascular effects of nicotine increase the fetal heart rate while decreasing fetal heart rate variability [9,10]. Studies demonstrating that pre-  Maternal Smoking during Pregnancy and Sudden Infant Death Using the National Maternal and 319 Infant Health Survey: A Case-Case Study natal exposure to cigarette smoke alters lung mechanics in infants and children have been bolstered by animal experiments linking nicotine to altered alveolar archi- tecture, pulmonary hypoplasia, increases in collagen deposition and decreases in elastin content [11]. Nico- tine is also known to adversely affect neural networks controlling respiration by acting as a fetal neuroterato- gen [2]. While many toxic, infectious, metabolic, physiologic and socioeconomic factors have been proposed as causes of SIDS, less attention has focused on the role of modi- fiable behaviors such as smoke exposure (from maternal and secondhand exposures) and breast-feeding [12,13]. Smoking during pregnancy continues to be a significant public health problem, with 13.8% of women in 2005 admitting to this behavior while pregnant [14]. Smoking rates during pregnancy in the United Kingdom were 17% in the same year and the rates in Canada were 24% [15]. The role of secondhand smoke exposure in the pathophysiology of SIDS is less clear, as is the role of lower socioeconomic status which has been reported as an independent risk factor for SIDS [13]. The majority of studies performed to date are not based on a sample of infants’ representative of the U.S. population. A modifiable intervention, sleep position, has been studied more closely. As a result of the Back to Sleep Campaign that was implemented in 1994, SIDS mortal- ity rates in the U.S. have declined for all ethnic groups [16]. However, even after the implementation of the Back to Sleep Campaign, non-Hispanic Black infants were 2.14 times more likely to die from SIDS than Non-Hispanic White infants [17]. This finding is parti- cularly problematic considering White women are much more likely to smoke during pregnancy than Black women [14,18]. This suggests that there may be an in- teraction between race and smoking status although this has not been reported to date. This study utilized the 1988 National Maternal and Infant Health Survey (NMIHS) to examine the effect of maternal smoking status during pregnancy and second- hand smoke exposure on the prevalence of death due to sudden infant death syndrome (SIDS) using a nationally representative sample of infant deaths from the U.S. population. Previous studies utilizing the NMIHS to exa- mine the relationship between maternal smoking and SIDS were incomplete, failing to account for breast feeding or secondhand smoke exposure [19,20]. The analysis presented in this manuscript accounts for both maternal smoking, as well as secondhand smoke expo- sure during pregnancy. Additionally, the analysis pre- sented in this paper considers whether or not the infant was breast fed, a variable previously identified as an important protective factor against postneonatal death [21]. 2. Methods The 1988 National Maternal and Infant Health Survey (NMIHS) were conducted by the National Center for Health Statistics (NCHS) to assist researchers in study- ing factors related to poor pregnancy outcomes. The survey is a nationally representative sample of 9953 (74.2% response rate) women who had live births, 3309 (69.3%) that had late fetal deaths and 5332 (65.3%) who had infant deaths in 1988. The mother’s questionnaire included information on prenatal care and health habits, including tobacco smoke exposure, previous and subse- quent pregnancies, characteristics of the parents and the baby’s health through 6 months of age. Only the infant death group from the total study population was ana- lyzed for this report. This study was approved by the University of Miami Institutional Review Board. Data were abstracted from the birth certificate for the following information: birthweight, gender, gestational age, maternal age, infant race and parity. Data were ab- stracted from the maternal questionnaire for maternal education level, history of cigarette smoking during pregnancy, and history of alcohol use during pregnancy. The NMIHS and Longitudinal Follow-Up drew strati- fied systematic samples from live births and infant deaths that were registered in 48 states, the District of Columbia, and New York City in 1988; and from fetal deaths that were registered in 46 states, the District of Columbia, and New York City in 1988. To increase the reliability of the data, Black infants were oversampled in the live-birth, fetal-death, and infant-death components of the NMIHS because Black infants have rates of low birthweight and infant mortality about twice that of White infants [22]. Very low-birthweight (<1.500 g) and moderately low-birthweight (1500 - 2499 g) infants were oversampled in the live-birth component to obtain a suf- ficient number of high-risk births for special studies. The live-birth and fetal-death components were re- stricted to women 15 years of age or over, and the in- fant-death component included women under 15 years of age. Mothers included in this study were women who had infant deaths and responded to the questionnaire from the NMIHS (N = 5332). The two study groups in the analysis consisted of (1) SIDS deaths, as defined by an ICD-9-CM code recorded as 798.0; and (2) other deaths consisting of all other infant deaths [23]. This data was obtained from linkage of the birth certificates and death certificates. The following study independent variables were ex- Copyright © 2011 SciRes. IJCM 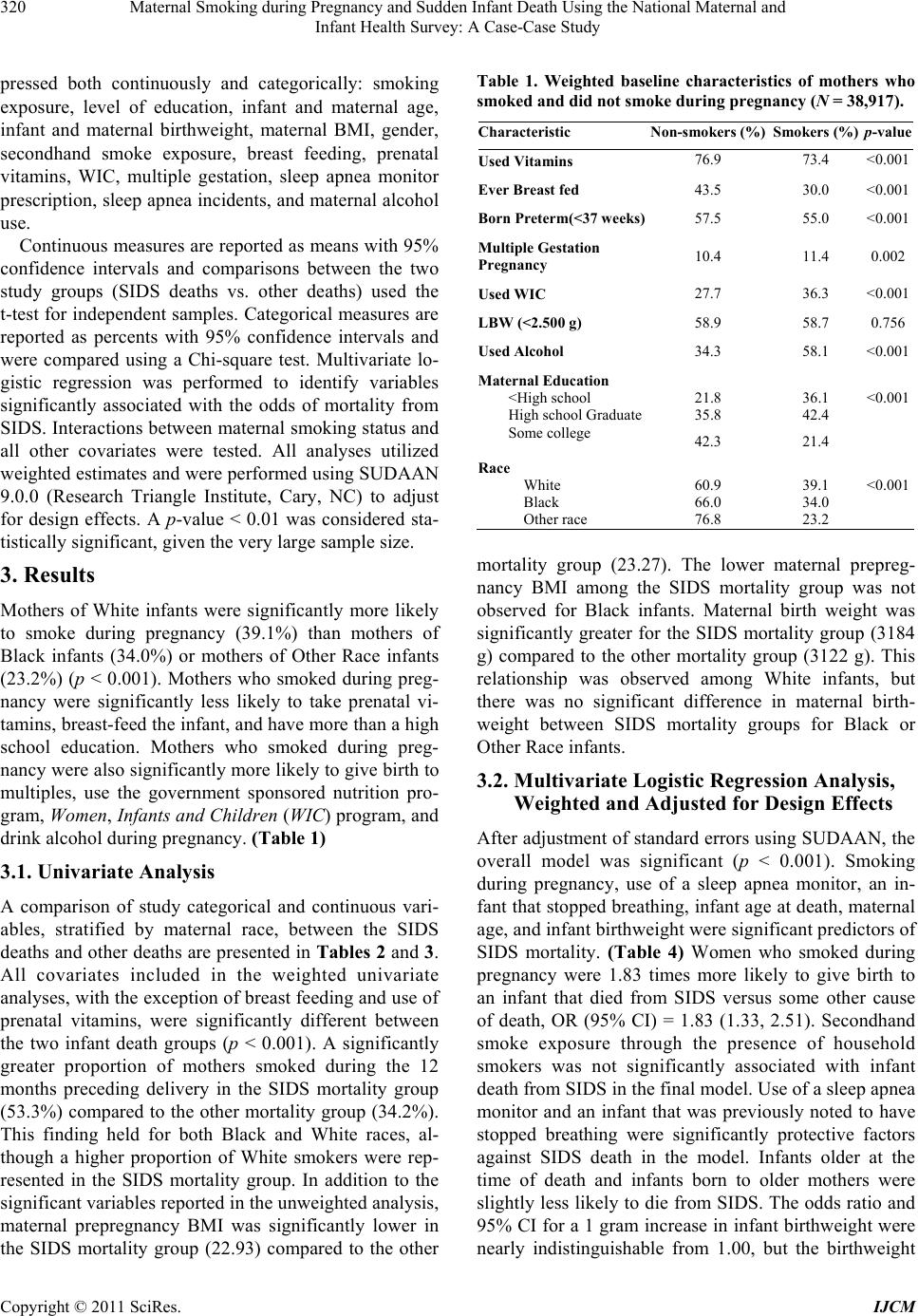 Maternal Smoking during Pregnancy and Sudden Infant Death Using the National Maternal and 320 Infant Health Survey: A Case-Case Study pressed both continuously and categorically: smoking exposure, level of education, infant and maternal age, infant and maternal birthweight, maternal BMI, gender, secondhand smoke exposure, breast feeding, prenatal vitamins, WIC, multiple gestation, sleep apnea monitor prescription, sleep apnea incidents, and maternal alcohol use. Continuous measures are reported as means with 95% confidence intervals and comparisons between the two study groups (SIDS deaths vs. other deaths) used the t-test for independent samples. Categorical measures are reported as percents with 95% confidence intervals and were compared using a Chi-square test. Multivariate lo- gistic regression was performed to identify variables significantly associated with the odds of mortality from SIDS. Interactions between maternal smoking status and all other covariates were tested. All analyses utilized weighted estimates and were performed using SUDAAN 9.0.0 (Research Triangle Institute, Cary, NC) to adjust for design effects. A p-value < 0.01 was considered sta- tistically significant, given the very large sample size. 3. Results Mothers of White infants were significantly more likely to smoke during pregnancy (39.1%) than mothers of Black infants (34.0%) or mothers of Other Race infants (23.2%) (p < 0.001). Mothers who smoked during preg- nancy were significantly less likely to take prenatal vi- tamins, breast-feed the infant, and have more than a high school education. Mothers who smoked during preg- nancy were also significantly more likely to give birth to multiples, use the government sponsored nutrition pro- gram, Women , In fants and Children (WIC) program, and drink alcohol during pregnancy. (Table 1) 3.1. Univariate Analysis A comparison of study categorical and continuous vari- ables, stratified by maternal race, between the SIDS deaths and other deaths are presented in Table s 2 and 3. All covariates included in the weighted univariate analyses, with the exception of breast feeding and use of prenatal vitamins, were significantly different between the two infant death groups (p < 0.001). A significantly greater proportion of mothers smoked during the 12 months preceding delivery in the SIDS mortality group (53.3%) compared to the other mortality group (34.2%). This finding held for both Black and White races, al- though a higher proportion of White smokers were rep- resented in the SIDS mortality group. In addition to the significant variables reported in the unweighted analysis, maternal prepregnancy BMI was significantly lower in the SIDS mortality group (22.93) compared to the other Table 1. Weighted baseline characteristics of mothers who smoked and did not smoke during pregnanc y (N = 38,917). Characteristic Non-smokers (%) Smokers (%)p-value Used Vitamins 76.9 73.4 <0.001 Ever Breast fed 43.5 30.0 <0.001 Born Preterm(<37 weeks)57.5 55.0 <0.001 Multiple Gestation Pregnancy 10.4 11.4 0.002 Used WIC 27.7 36.3 <0.001 LBW (<2.500 g) 58.9 58.7 0.756 Used Alcohol 34.3 58.1 <0.001 Maternal Education <High school 21.8 36.1 <0.001 High school Graduate35.8 42.4 Some college 42.3 21.4 Race White 60.9 39.1 <0.001 Black 66.0 34.0 Other race 76.8 23.2 mortality group (23.27). The lower maternal prepreg- nancy BMI among the SIDS mortality group was not observed for Black infants. Maternal birth weight was significantly greater for the SIDS mortality group (3184 g) compared to the other mortality group (3122 g). This relationship was observed among White infants, but there was no significant difference in maternal birth- weight between SIDS mortality groups for Black or Other Race infants. 3.2. Multivariate Logistic Regression Analysis, Weighted and Adjusted for Design Effects After adjustment of standard errors using SUDAAN, the overall model was significant (p < 0.001). Smoking during pregnancy, use of a sleep apnea monitor, an in- fant that stopped breathing, infant age at death, maternal age, and infant birthweight were significant predictors of SIDS mortality. (Table 4) Women who smoked during pregnancy were 1.83 times more likely to give birth to an infant that died from SIDS versus some other cause of death, OR (95% CI) = 1.83 (1.33, 2.51). Secondhand smoke exposure through the presence of household smokers was not significantly associated with infant death from SIDS in the final model. Use of a sleep apnea monitor and an infant that was previously noted to have stopped breathing were significantly protective factors against SIDS death in the model. Infants older at the time of death and infants born to older mothers were slightly less likely to die from SIDS. The odds ratio and 95% CI for a 1 gram increase in infant birthweight were nearly indistinguishable from 1.00, but the birthweight Copyright © 2011 SciRes. IJCM  Maternal Smoking during Pregnancy and Sudden Infant Death Using the National Maternal and 321 Infant Health Survey: A Case-Case Study Table 2. Baseline categorical characteristics (weighted) of 1988 NMIHS cohort for infant mortality groups (N = 38,917). Characteristic SIDS Death (%) Other Death (%) p-value N 5215 33,702 Gender Female 40.8 44.1 <0.001 Male 59.2 55.9 Mother Smoked 12 Months Preceding Delivery Black 47.1 32.0 <0.001 White 59.3 35.9 <0.001 Other Race 32.4 20.8 <0.001 Smokers in Home During Pregnancy Black 47.1 45.3 0.230 White 56.7 38.3 <0.001 Other Race 39.3 33.7 0.090 Mother Drank Alcohol 12 Months Preceding Delivery Black 35.8 31.1 0.001 White 54.5 48.7 <0.001 Other 32.4 26.0 0.038 Mother Ever Breastfed Black 15.5 16.8 0.367 White 43.0 43.8 0.481 Other Race 61.9 46.4 <0.001 Mother’s Education Level Total High School Graduate 38.3 38.3 <0.001 Some College 26.7 35.9 Black High School Graduate 39.2 40.1 <0.001 Some College 19.6 29.5 White High School Graduate 39.9 38.4 <0.001 Some College 27.3 38.8 Other High School Graduate 26.0 27.3 <0.001 Some College 29.8 46.2 Prenatal Vitamin Use Black 63.6 65.6 0.140 White 78.0 80.9 <0.001 Other Race 82.5 75.4 0.017 WIC Use During Pregnancy Black 60.8 43.6 <0.001 White 39.4 21.7 <0.001 Other 52.8 25.8 <0.001 Multiple Gestation Birth Black 6.4 11.4 <0.001 White 5.5 12.5 <0.001 Other Race 2.3 11.7 <0.001 Premature Bir th < 37 weeks Total 21.6 62.6 <0.001 Black 32.6 73.4 <0.001 White 17.4 58.6 <0.001 Other 17.2 52.3 <0.001 Apnea Monitor Prescribed Total 2.4 2.5 <0.001 Black 3.3 1.6 <0.001 White 1.9 2.8 <0.001 Other 0.0 1.2 <0.001* Infant Ever Stopped Breathing Total 17.2 5.2 <0.001 Black 16.3 4.4 <0.001 White 17.8 5.4 <0.001 Other 4.2 5.2 <0.001* *indicates insufficient sample size (at least 1 cell had a count of 0). Table 3. Baseline continuous measures (weighted) of 1988 nmihs cohort for infant mortality groups (N = 38,917). Characteristic SIDS Death (Mean; 95% CI) Other Death (Mean; 95% CI) -value N 5215 33,702 Number of Ciga- rettes/Day After Knowledge of Pregnancy Black 7.9 (7.3, 8.6) 8.1 (7.8, 8.4) 0.680 White 12.3 (11.9, 12.7) 9.1 (8.9, 9.3) <0.001 Other 13.9 (10.8, 17.0) 6.8 (5.9, 7.7) <0.001 Maternal Level of Education (Years) Black 11.6 (11.5, 11.7) 12.1 (12.0, 12.2)<0.001 White 11.9 (11.8, 12.0) 12.5 (12.4, 12.5)<0.001 Other Race 10.9 (10.4, 11.4) 12.1 (11.8, 12.3)<0.001 Maternal Age (Years) Black 22.8 (22.5, 23.1) 24.1 (24.0, 24.2)<0.001 White 24.5 (24.3, 24.7) 26.2 (26.1, 26.3)<0.001 Other 23.8 (23.1, 24.5) 29.1 (28.8, 29.5)<0.001 Maternal BMI Black 23.8 (23.5, 24.1) 24.0 (23.9, 24.2)0.207 White 22.6 (22.4, 22.7) 23.0 (22.9, 23.1)<0.001 Other 23.2 (22.8, 23.7) 21.7 (21.5, 22.0)<0.001 Maternal Birth weight (Kg) Black 3.00 (2.95, 3.05) 3.00 (2.98, 3.02)0.993 White 3.25 (3.23, 3.27) 3.17 (3.16, 3.18)<0.001 Other 3.16 (3.06, 3.25) 3.16 (3.12, 3.21)0.876 Child’s Birth weight (Kg) Black 2.86 (2.82, 2.90) 1.47 (1.44, 1.49)<0.001 White 3.19 (3.16, 3.21) 1.90 (1.88, 1.92)<0.001 Other 3.17 (3.10, 3.24) 2.03 (1.95, 2.10)<0.001 Gestational Age (Weeks) 38.4 (38.3, 38.5) 31.6 (31.5, 31.7)<0.001 Infant Age at Death (Days) 96.6 (94.5, 98.6) 54.9 (53.7, 56.1)<0.001 Copyright © 2011 SciRes. IJCM 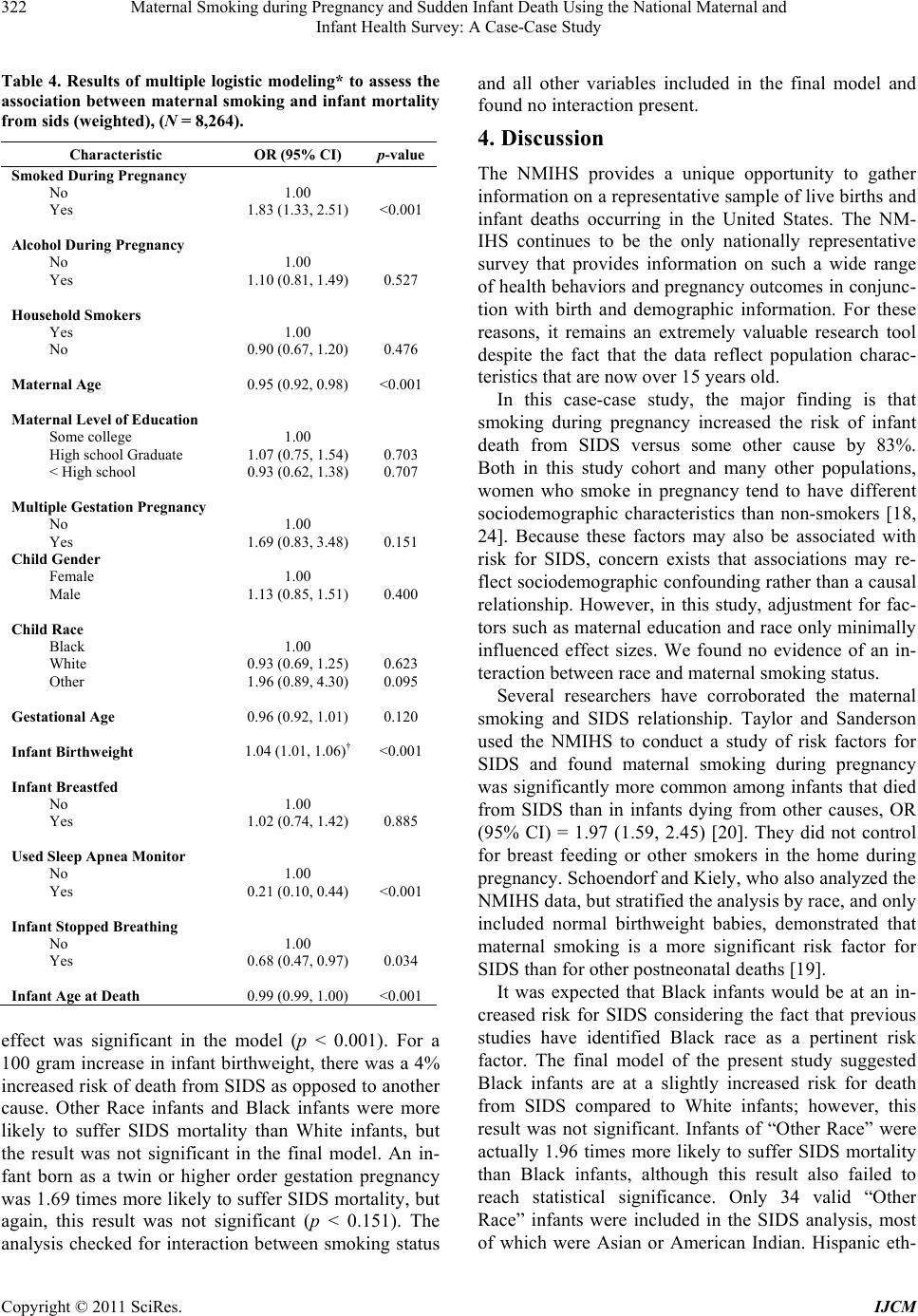 Maternal Smoking during Pregnancy and Sudden Infant Death Using the National Maternal and 322 Infant Health Survey: A Case-Case Study Table 4. Results of multiple logistic modeling* to assess the association between maternal smoking and infant mortality from sids (weighted), (N = 8,264). Characteristic OR (95% CI) p-value Smoked During Pregnancy No 1.00 Yes 1.83 (1.33, 2.51) <0.001 Alcohol During Pregnancy No 1.00 Yes 1.10 (0.81, 1.49) 0.527 Household Smokers Yes 1.00 No 0.90 (0.67, 1.20) 0.476 Maternal Age 0.95 (0.92, 0.98) <0.001 Maternal Level of Education Some college 1.00 High school Graduate 1.07 (0.75, 1.54) 0.703 < High school 0.93 (0.62, 1.38) 0.707 Multiple Gestation Pregnancy No 1.00 Yes 1.69 (0.83, 3.48) 0.151 Child Gender Female 1.00 Male 1.13 (0.85, 1.51) 0.400 Child Race Black 1.00 White 0.93 (0.69, 1.25) 0.623 Other 1.96 (0.89, 4.30) 0.095 Gestational Age 0.96 (0.92, 1.01) 0.120 Infant Birthweight 1.04 (1.01, 1.06)† <0.001 Infant Breastfed No 1.00 Yes 1.02 (0.74, 1.42) 0.885 Used Sleep Apnea Monitor No 1.00 Yes 0.21 (0.10, 0.44) <0.001 Infant Stopped Breathing No 1.00 Yes 0.68 (0.47, 0.97) 0.034 Infant Age at Death 0.99 (0.99, 1.00) <0.001 effect was significant in the model (p < 0.001). For a 100 gram increase in infant birthweight, there was a 4% increased risk of death from SIDS as opposed to another cause. Other Race infants and Black infants were more likely to suffer SIDS mortality than White infants, but the result was not significant in the final model. An in- fant born as a twin or higher order gestation pregnancy was 1.69 times more likely to suffer SIDS mortality, but again, this result was not significant (p < 0.151). The analysis checked for interaction between smoking status and all other variables included in the final model and found no interaction present. 4. Discussion The NMIHS provides a unique opportunity to gather information on a representative sample of live births and infant deaths occurring in the United States. The NM- IHS continues to be the only nationally representative survey that provides information on such a wide range of health behaviors and pregnancy outcomes in conjunc- tion with birth and demographic information. For these reasons, it remains an extremely valuable research tool despite the fact that the data reflect population charac- teristics that are now over 15 years old. In this case-case study, the major finding is that smoking during pregnancy increased the risk of infant death from SIDS versus some other cause by 83%. Both in this study cohort and many other populations, women who smoke in pregnancy tend to have different sociodemographic characteristics than non-smokers [18, 24]. Because these factors may also be associated with risk for SIDS, concern exists that associations may re- flect sociodemographic confounding rather than a causal relationship. However, in this study, adjustment for fac- tors such as maternal education and race only minimally influenced effect sizes. We found no evidence of an in- teraction between race and maternal smoking status. Several researchers have corroborated the maternal smoking and SIDS relationship. Taylor and Sanderson used the NMIHS to conduct a study of risk factors for SIDS and found maternal smoking during pregnancy was significantly more common among infants that died from SIDS than in infants dying from other causes, OR (95% CI) = 1.97 (1.59, 2.45) [20]. They did not control for breast feeding or other smokers in the home during pregnancy. Schoendorf and Kiely, who also analyzed the NMIHS data, but stratified the analysis by race, and only included normal birthweight babies, demonstrated that maternal smoking is a more significant risk factor for SIDS than for other postneonatal deaths [19]. It was expected that Black infants would be at an in- creased risk for SIDS considering the fact that previous studies have identified Black race as a pertinent risk factor. The final model of the present study suggested Black infants are at a slightly increased risk for death from SIDS compared to White infants; however, this result was not significant. Infants of “Other Race” were actually 1.96 times more likely to suffer SIDS mortality than Black infants, although this result also failed to reach statistical significance. Only 34 valid “Other Race” infants were included in the SIDS analysis, most of which were Asian or American Indian. Hispanic eth- Copyright © 2011 SciRes. IJCM  Maternal Smoking during Pregnancy and Sudden Infant Death Using the National Maternal and 323 Infant Health Survey: A Case-Case Study nicity was distributed among White, Black, and Other Race infants and was not readily isolated in this analysis. Although race was not a significant predictor of SIDS mortality, future studies should pay special attention to American Indians, a group in which SIDS accounted for 81.8% of infant deaths in addition to representing a group where smoke exposure during pregnancy is highly prevalent. These results further highlight the importance of counseling women against smoking during pregnancy and providing access to cessation programs. Bed-sharing and sleep position have been implicated as risk factors for SIDS and pacifier use during sleep has been implicated as a protective factor for SIDS; however, these variables were not available for analysis in the NMIHS [25,26]. The NMIHS and Longitudinal Fol- low-Up were conducted prior to the initiation of the Back to Sleep campaign. Sleep behaviors are pertinent variables to consider as risk factors for SIDS mortality because of their possible impact on the infant’s control of arousal mechanisms, but due to limitations of the dataset, only smoke exposure could be assessed [27]. In addition to smoking during pregnancy, use of a sleep apnea monitor and the infant having ever stopped breathing were significantly associated with risk of SIDS mortality. Use of a sleep apnea monitor decreased the risk of SIDS mortality by 79%, and noticing the in- fant had stopped breathing reduced the risk of SIDS mortality by 32%. The univariate analysis indicates Black infants that died from SIDS were more likely to have been prescribed a sleep apnea monitor and that infants that stopped breathing were more likely to have died from SIDS; however, the final regression model found the association reversed. There were high per- centages of missing cases for both of these variables, possibly reducing the validity of conclusions drawn about these relationships. An analysis of the NMIHS using SIDS deaths and live controls also described a protective effect of home apnea monitoring [28]. It is important to note when interpreting the analysis that a distinction should be made between statistical significance and clinical significance. The large sample size produced by weighting often times results in very small p-values that reflect small effect estimates of questionable clinical relevance. In Table 1, for example, one might expect a significantly higher percentage of preterm infants to be born to smokers rather than to non-smokers, rather than vice-versa. Prematurity is a common characteristic among infants suffering all causes of mortality; and it is likely that the statistically significant difference seen between smokers and non- smokers regarding prematurity is the product of the large sample size, and not a clinically important observation. SIDS continues to be a major cause of postneonatal death. Although lower than in 1988, the prevalence of smoking during pregnancy continues to be substantial, both in the U.S. and other Western countries. With overall smoking prevalence among women increasing in many countries, maternal smoking is clearly an impor- tant international health issue. In many developing countries, the lack of adequate health facilities, and to- bacco education or control programs can increase the health risks of maternal smoking on the fetus and infant. Importantly, this analysis found neither race, nor socio- economic status, were significantly associated with SIDS risk, suggesting universal tobacco screening and education during pregnancy should be undertaken. Fi- nally, while many health benefits of breast feeding have been identified, this study failed to find a significant protective effect of breast feeding in reducing the risk of SIDS mortality. Further study of this topic is needed before breast feeding can be recommended or dis- counted as a modifiable risk factor in the prevention of SIDS. The relationship between maternal smoking status and SIDS was clear. The importance of abstaining from tobacco smoke exposure during and after their preg- nancy should be stressed when educating all pregnant women how to maintain a healthy pregnancy and smok- ing cessation guidance should be made available to all pregnant women with a positive screen. REFERENCES [1] R. Machaalani, K. A. Waters and K. D. Tinworth, “Ef- fects of Postnatal Nicotine Exposure on Apoptotic Mark- ers in the Developing Piglet Brain,” Neuroscience, Vol. 132, No. 2, 2005, pp. 325-333. doi:10.1016/j.neuroscience.2004.12.039 [2] T. A. Slotkin, “Cholinergic Systems in Brain Develop- ment and Disruption by Neurotoxicants: Nicotine, Envi- ronmental Tobacco Smoke, Organophosphates,” Toxi- cology and Applied Pharmacology, Vol. 198, No. 2, 2004, pp. 132-151. doi:10.1016/j.taap.2003.06.001 [3] L. Sartiani, E. Cerbai, G. Lonardo, et al., “Prenatal Ex- posure to Carbon Monoxide Affects Postnatal Cellular Electrophysiological Maturation of the Rat Heart,” Cir- culation, Vol. 109, 2004, pp. 419-423. doi:10.1161/01.CIR.0000109497.73223.4D [4] R. A. Neff, S. J. Simmens, C. Evans and D. Mendelowitz, “Prenatal Nicotine Exposure Alters Central Cardiorespi- ratory Responses to Hypoxia in Rats: Implications for Sudden Infant Death Syndrome,” The Journal of Neuro- science, Vol. 24, No. 42, 2004, pp. 9261-9268. doi:10.1523/JNEUROSCI.1918-04.2004 [5] C. A. Browne, P. B. Colditz and K. R. Dunster, “Infant Autonomic Function Is Altered by Maternal Smoking during Pregnancy,” Early Human Development, Vol. 59, Copyright © 2011 SciRes. IJCM  Maternal Smoking during Pregnancy and Sudden Infant Death Using the National Maternal and Infant Health Survey: A Case-Case Study Copyright © 2011 SciRes. IJCM 324 No. 3, 2000, pp. 209-218. doi:10.1016/S0378-3782(00)00098-0 [6] W. P. Fifer, S. T. Fingers, M. Youngman, E. Go- mez-Gribben and M. M. Myers, “Effects of Alcohol and Smoking during Pregnancy on Infant Autonomic Con- trol,” Developmental Psychobiology, Vol. 51, No. 3, 2009, pp. 234-242. doi:10.1002/dev.20366 [7] J. R. Duncan, M. Garland, M. M. Myers, et al., “Prenatal Nicotine-Exposure Alters Fetal Autonomic Activity and Medullary Neurotransmitter Receptors: Implications for SIDS,” Journal of Applied Physiology, Vol. 107, No. 5, 2009, pp. 1579-1590. doi:10.1152/japplphysiol.91629.2008 [8] O. Hafström, J. Milerad, K. L. Sandberg and H. W. Sun- dell, “Cardiorespiratory Effects of Nicotine Exposure during Development,” Respiratory Physiology and Neu- robiology, Vol. 149, No. 1-3, 2005, pp. 325-341. doi:10.1016/j.resp.2005.05.004 [9] A. Lindblad, K. Marsal and K. E. Andersson, “Effect of Nicotine on Human Fetal Blood Flow,” Obstetrics and Gynecology, Vol. 72, No. 3, 1988, pp. 371-382. [10] G. Thiriez, M. Bouhaddi, L. Mourot, et al., “Heart Rate Variability in Preterm Infants and Maternal Smoking during Pregnancy,” Clinical Autonomic Research, Vol. 19, No. 3, 2009, pp. 149-156. doi:10.1007/s10286-009-0003-8 [11] R. A. Pierce and N. M. Nguyen, “Prenatal Nicotine Ex- posure and Abnormal Lung Function,” American Journal of Respiratory Cell and Molecular Biology, Vol. 26, No. 1, 2002, pp. 10-13. [12] R. W. Byard and H. F. Krous, “Sudden Infant Death Syndrome: Problems, Progress and Possibilities,” Arnold, London, 2001. [13] N. Spencer and S. Logan, “Sudden Unexpected Death in Infancy and Socioeconomic Status: A Systemic Review,” Journal of Epidemiology and Community Health, Vol. 58, No. 5, 2004, pp. 366-373. doi:10.1136/jech.2003.011551 [14] V. T. Tong, J. R. Jones, P. M. Dietz, D. D’Angelo and J. M. Bombard, “Trends in Smoking before, during and after Pregnancy. Pregnancy Risk Assessment Monitoring Sys- tem (PRAMS), United States, 31 Sites, 2000-2005,” Mor- bidity and Mortality Weekly Report, Vol. 58, No. SS04, 2009, pp. 1-29. [15] S. Kafouri, G. Leonard, M. Perron, L. Richer, J. R. Seguin, S. Veillette, Z. Pausova and T. Paus, “Maternal Cigarette Smoking during Pregnancy and Cognitive Per- formance in Adolescence,” International Journal of Epi- demiology, Vol. 38, No. 1, 2009, pp. 158-172. doi:10.1093/ije/dyn250 [16] M. Willinger, C.-W. Ko, H. J. Hoffman, R. C. Kessler and M. J. Corwin, “Factors Associated with Caregivers’ Choice of Infant Sleep Position, 1994-1998: The National Infant Sleep Position Study,” The Journal of American Medical Association, Vol. 283, No. 16, 2000, pp. 2135- 2142. doi:10.1001/jama.283.16.2135 [17] P. Muhuri, M. F. MacDorman and T. M. Ezzati-Rice, “Racial Differences in Leading Causes of Infant Death in the United States,” Paediatric and Perinatal Epidemiol- ogy, Vol. 18, No. 1, 2004, pp. 51-60. doi:10.1111/j.1365-3016.2004.00535.x [18] T. J. Mathews, “Smoking during Pregnancy in the 1990s,” National Vital Statistics Reports, Vol. 49, No. 7, 2001, pp. 1-14. [19] K. C. Schoendorf and J. L. Kiely, “Relationship of Sud- den Infant Death Syndrome to Maternal Smoking during and after Pregnancy,” Pediatrics, Vol. 90, No. 6, 1992, pp. 905-908. [20] J. A. Taylor and M. Sanderson, “A Reexamination of the Risk Factors for the Sudden Infant Death Syndrome,” The Journal of Pediatrics, Vol. 126, No. 6, 1995, pp. 887-891. doi:10.1016/S0022-3476(95)70202-4 [21] A. Chen and W. J. Rogan, “Breastfeeding and the Risk of Postneonatal Death in the United States,” Pediatrics, Vol. 113, No. 5, 2004, pp. 435-439. doi:10.1542/peds.113.5.e435 [22] Public Health Service, “National Center for Health Statis- tics. Health, United States, 1991,” Hyattsville, USA, 1992. [23] Public Health Service and Health Care Financing Ad- ministration, “International Classification of Diseases, Ninth Revision, Clinical Modification,” Washington, USA, 1980. [24] Department of Health and Human Services, “National Center for Health Statistics. Health, United States, 1998 with Socioeconomic and Health Chartbook,” Hyattsville, USA, 1998. [25] M. Mitka, “Policy Targets Lowering SIDS Incidence,” The Journal of American Medical Association, Vol. 294, No. 19, 2005, p. 2420. doi:10.1001/jama.294.19.2420 [26] D.-K. Li, M. Willinger, D. B. Petitti, R. Odouli, L. Liu and H. J. Hoffman, “Use of a Dummy (Pacifier) during Sleep and Risk of Sudden Infant Death Syndrome (SIDS): Population Based Case-Control Study,” British Medical Journal, Vol. 332, No. 7532, 2005, p. 18. doi:10. 1136/bmj.38671.640475.55 [27] H. L. Richardson, A. M. Walker and R. S. Horne, “Ma- ternal Smoking Impairs Arousal Patterns in Sleeping In- fants,” Sleep, Vol. 32, No. 4, 2009, pp. 515-521. [28] M. H. Malloy and H. J. Hoffman, “Home Apnea Moni- toring and Sudden Infant Death Syndrome,” Preventive Medicine, Vol. 25, No. 6, 1996, pp. 645-649. doi:10.1006/pmed.1996.9998
|