International Journal of Otolaryngology and Head & Neck Surgery
Vol.2 No.2(2013), Article ID:29596,6 pages DOI:10.4236/ijohns.2013.22017
Sensori-Neural Hearing Loss Client’s Performance with Receiver-In-Canal (RIC) Hearing Aids
1Ali Yavar Jung National Institute for the Hearing Handicapped, Southern Regional Centre, Department of Disability Affairs, Ministry of Social Justice and Empowerment, Goverment of India, Secunderabad, India
2Ali Yavar Jung National Institute for the Hearing Handicapped, Department of Disability Affairs, Ministry of Social Justice and Empowerment, Goverment of India, Mumbai, India
Email: prakash_nihh@rediffmail.com, aparnaravichandran75@gmail.com, sarathna@yahoo.co.in, kaki.ashritha@gmail.com, madhav.aslp@gmail.com, vindhyakande25@gmail.com
Received February 7, 2013; revised March 11, 2013; accepted March 21, 2013
Keywords: Sensori Neural Hearing Loss; RIC Hearing Aids; Functional Gain Measures
ABSTRACT
Background: Individuals fitted with hearing aids complain of the unnatural sound quality of their voice, other internally generated sounds such as chewing and swallowing sounds “hollow”, “muffled” sounds. Receiver-In-Canal hearing aids are favored due to small size, discrete appearance and ability to minimize occlusion. Aim: To compare the performance of Receiver-In-Canal (RIC) to traditional ear tip (ET), ear moulds (EM) fittings using Functional gain measures. Method: Ten subjects with flat moderately severe sensori neural hearing loss participated in the study. Subjective unaided and aided measures for digital BTE hearing aids with ear tip, ear mould or Receiver-In-Canal for pure tones of 250 Hz, 500 Hz, 1000 Hz, 2000 Hz, 4000 Hz were obtained. Results and Discussion: Higher scores were obtained with Receiver-In-Canal fitting on Functional gain measures. No significant difference between all the three conditions was obtained at low frequencies especially at 500 Hz, as Receiver-In-Canal hearing aids attenuate low frequency sounds automatically when the ear is left open (up to 30 dB less amplification at 500 Hz) especially for hearing in noisy situations. Conclusion: The results suggest that Receiver-In-Canal fittings are an effective means of overcoming the major barriers to the acceptance of amplification and further suggest the clinical importance of subjective measures in measuring aided benefit of open-fit devices in the rehabilitation of person’s with moderately severe to severe SN hearing loss.
1. Introduction
In the past decades, majority of the hearing aid dispensing centers prescribe hearing aids either with ear mould (soft/hard) or with ear tips. Frequently, hearing aid users complain the unnatural sound quality of their voice, other internally generated sounds such as chewing and swallowing sounds “hollow”, “muffled” [1-3]. Although such complaints sometimes result from sub optimal hearing aid settings, they may also be associated with significant occlusion created by the hearing aid shell (or) ear mould [1-3]. When the ear canal is occluded, much of the energy is trapped, causing an increase in the sound pressure level delivered to the tympanic membrane and, ultimately, to the cochlea. For some closed vowels, occluding the external ear using a shallow insertion depth can result in levels of 100 dB SPL or greater within the canal [4]. This energy is centered primarily in the low frequencies, with the peak of the occlusion effect typically occurring in the range of 200 to 500 Hz [5]. The magnitude of the occlusion effect varies among individuals. Typical values are around 12 to 16 dB, but in some cases may be as great as 25 to 30 dB [1,6]. Patient dissatisfaction resulting from the occlusion effect can lead to inconsistent hearing aid use (or) outright rejection [4].
Studies revealed that 27.8% of patients experienced problems related to the quality of their voice [7]. The occlusion effect has been documented as a consistent problem when it comes to maximizing satisfaction with conventional hearing aid fitting [8,9] others reported occlusion and amplusion effects in 28% to 65% of hearing aid wearers [10]. Amplusion is the combination of low frequency amplification and the occlusion effect [3]. Studies have also reported that when hearing aid is fitted to occluded ear it leads to loss of localization cues, poor sound quality and discomfort [11].
Receiver-In-Canal hearing aid also known as RIC have been introduced by hearing aid industry to overcome the above mentioned problems. While open canal hearing instruments have been available for decades, improved digital signal processing (DSP) technology has made open fittings possible for a larger portion of hearing loss configuration. This hearing aid consists of a small, nonoccluding, non custom ear tip placed in the ear canal. Receiver-In-Canal hearing aids can be effective in addressing end-user concerns such as cosmetic appeal, wearer comfort and occlusion [12]. Reported benefits of open canal fitting that have lead to a rise in popularity, which has improved comfort for the user, sound quality, cosmetics, localization, ease of repair/maintenance, intelligibility, high frequency gain and reduction of occlusion effect [13]. Many of these benefits are a result of the design of these products, leaving the ear canal open to allow air circulation as well as unaltered sound information to enter the ear canal. A study of dispenser opinions of open canal (OC) hearing aids reported that 92% of dispensers surveyed believed that patients were at least as satisfied (or) more satisfied with OC devices than with non OC devices [14].
Significantly greater satisfaction was reported with the open-ear canal device than with traditional fittings, such as the ITE hearing aids [15]. Specifically, the study suggested that OC users were significantly more satisfied with the following product aspects: comfort, visibility, size, clearness, feedback, reliability, appearance, noisy situations, expense, value, natural sounding, localization, and telephone usability, among others. Significantly higher satisfaction ratings of open-canal than non open canal hearing aids with regards to sound localization, quality of their own voice, phone comfort and appearance in experienced hearing aid users was reported by [16].
Receiver-In-Canal hearing aids reduce occlusion effect (i.e. the hollowness of voice), and improves sound quality of the wearer’s own voice, and improves localization ability. The purported advantages of Open Canal hearing aids suggest that these devices may be valuable for individuals with high-frequency hearing loss. The reduction or elimination of the occlusion effect, a more comfortable physical fit, and the relatively inconspicuous appearance afforded by OC hearing aids have the potential to increase user satisfaction. Although, these hearing aids were present since a decade, there is a recent rise of behind the ear (BTE) hearing aid market share from 26% in 2004 to 44% for the second quarter of the year. A report on online dispenser survey stated that on an average 17% of all the fittings were open, which suggests that close to 40% of the BTEs being dispensed at the time were open fit [13]. In particular, advances in acoustic feedback reduction algorithms have made modern open canal hearing fittings feasible. Sophisticated feedback reduction algorithms are an integral part of open canal hearing aids, allowing them to provide 8 to 15 dB of additional gain before entering the audible oscillatory state [17]. Manufacturer’s product claims and dispenser surveys also tend to support the belief that the unique feature of open canal devices offer patients added advantages [14].
Traditional tube or IROS (Ipsilateral routing of signal) behind-the-ear (BTE) fittings can alleviate occlusion and insertion loss, but may be cosmetically unappealing and present feedback concerns due to the open feedback loop. Resolving or minimizing this issue is considered necessary for the successful use of hearing aids and for improving satisfaction with amplification. Fitting patients who have moderately severe sensori neural hearing losses with appropriate amplification has always been a challenging situation. In general, in quiet situations, these patients often exhibit little or no difficulty in understanding speech due to the audibility of a significant portion of lower-frequency speech phonemes but the voiceless consonants like p, t, k, f, s and ch are often missed, they experience greater difficulty with speech understanding in presence of background noise and also for soft or high pitched voice and this reduction in audibility of high-frequency information can be significantly handicapping. These patients are often hesitant to use hearing aids due to the perceived disadvantages of traditional hearing aids. Visibility, fit, and comfort have been identified as three primary factors that can affect a person’s satisfaction with and acceptance of amplification. Recently in India there is an increase in number of hearing aid prescriptions with Receiver-In-Canal fittings. Although there are anecdotal and empirical reports from hearing aid manufacturer of increased patient satisfaction with open fittings, limited data exist outside of the hearing aid industry. Product popularity and laboratory evidence do not equate to real-world satisfaction and benefit in everyday listening situations. In recent years, evidencebased practice has pointed out the need for effectiveness as well as efficiency studies. With the recent growth in the Open Canal market, there is a need to investigate the performance of Receiver-In-canal hearing aids. The present study aims to compare the “Functional gain” measures in subjects fitted with digital behind the ear hearing aids either with ear tip (ET), ear moulds (EM) or Receiver-In-Canal (RIC) hearing aids. In India also, RIC hearing aids are slowly gaining popularity and there is an increase in number of hearing aid prescriptions with RIC hearing aids.
2. Methodology
2.1. Subjects Selection
10 subjects in the age range of 30 - 50 years having moderately severe sensorineural Hearing loss with flat audiogram configuration were recruited from those reporting to the Ali Yavar Jung National Institute for the Hearing Handicapped, Southern Regional centre for hearing aid fitting using a purposive sampling technique. Necessary consent was obtained from the subjects prior to testing.
2.2. Tools
The tools used in the present study were binaural digital behind the ear (BTE) hearing aid with ear tip fitting, ear mould fitting and RIC fitting. The hearing aids were programmed with a Basic Fit or first fit using NAL-NL1 prescriptive method and were adjusted as per the client’s requirement and satisfaction. All the hearing aids were matched in their technical specifications. RMS Acoustia Pure tone audiometer with free field set up was used for presenting the pure tone stimuli of 250 Hz, 500 Hz, 1000 Hz, 2000 Hz and 4000 Hz in unaided and aided conditions. The experiment was conducted in a sound treated free-field setup calibrated as per American National Standard Specifications for Audiometers [18].
2.3. Procedure for Data Collection
Hearing thresholds for subjects were obtained and based on their hearing levels the digital behind the ear hearing aids were selected and programmed with a Basic Fit or first fit using NAL-NL1 prescriptive method. The gain characteristics were adjusted as per the client’s requirement and satisfaction. For the purpose of verification of the performance of the fitted device the subjects were made to sit comfortably and their unaided thresholds in sound field were measured using a calibrated audiometer [18]. Pure tone stimuli of 250 Hz, 500 Hz, 1000 Hz, 2000 Hz, 4000 Hz was presented and they were instructed to respond by pressing the patient response button whenever they hear the stimulus. The method employed was a modified method of limits with 10 dB descending steps and 5 dB ascending steps [19]. Once the unaided thresholds were obtained the participants were randomly fitted with digital BTE hearing aids with either ear tip fitting, ear mould fitting or Receiver-In-Canal fitting and their Pure tone aided responses for 250 Hz, 500 Hz, 1000 Hz, 2000 Hz, 4000 Hz were collected in three different phases. Prior to testing, familiarization of the test procedure was done and detail procedure was informed to the participants. Functional gain was measured by taking the difference between aided and unaided sound field thresholds.
Technical Phases:
Phase 1: Participants were fitted with hearing aids with ear tips (ET) and Functional Gain was measured.
Phase 2: Participants were fitted with hearing aids with ear moulds (EM) and Functional Gain was measured.
Phase 3: Participants were fitted with Receiver-InCanal (RIC) hearing aids and Functional Gain was measured.
2.4. Statistical Analysis of Data
The total score of functional gain for all the three phases were computed and analyzed using SPSS software version 17. The mean scores and standard deviations for each phase was computed and to explore all possible pair wise comparisons of means, the data was subjected to One way ANOVA and Post-Hoc analysis in order to find out statistical significance between phases.
3. Results
The mean values of functional gain obtained for ear tip fitting at frequencies of 250 Hz, 500 Hz, 1000 Hz, 2000 Hz, 4000 Hz are 26.00, 28.00, 29.00, 31.00 and 35.50 respectively with the highest mean value at 4000 Hz (35.50) and lowest mean value at 250 Hz (35.50); for ear mould fitting the mean values of functional gain are 29.00, 29.50, 32.50, 38.50, 39.00 respectively with highest mean value at 4000 Hz (39.00) and lowest mean value at 250 Hz (29.00) and for Receiver-In-Canal fitting the mean values of functional gain are 34.50, 33.50, 38.50, 43.00 and 48.00 respectively with the highest mean value at 4000 Hz (48.00) and lowest mean value at 250 Hz (34.50) as shown in Figure 1. It is noted from the results that the functional gain values increased with an increase in frequency (i.e.) highest values were obtained for 4000 Hz (31.00, 39.00, and 48.00) for all the three conditions (i.e.) ear tip, ear mould and Receiver in the Canal. The results were least for low frequency stimuli across the three conditions (i.e.) ear tip, ear mould and Receiver in the Canal. Results also indicate that the Receiver-In-Canal hearing aids had highest functional gain values compared to ear moulds and ear tips. The lowest functional gain values are for ear tip fitting. To find out the statistical significance between the three fittings the obtained means and standard deviation were subjected to One-Way ANOVA, the results reveal a significant difference within groups and also in between the fittings (P > 0.05) except at 500 Hz were there was no significant difference (0.27, P > 0.05).
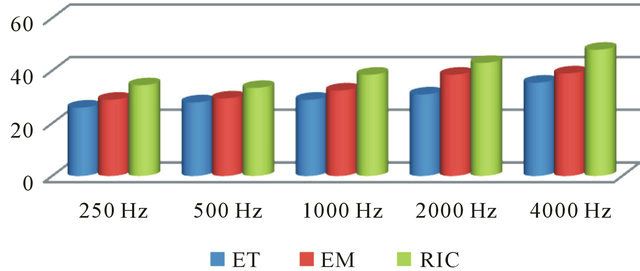
Figure 1. Comparison of mean values of functional gain of adults fitted with ear tip, ear mould and Receiver-In-Canal hearing aids.
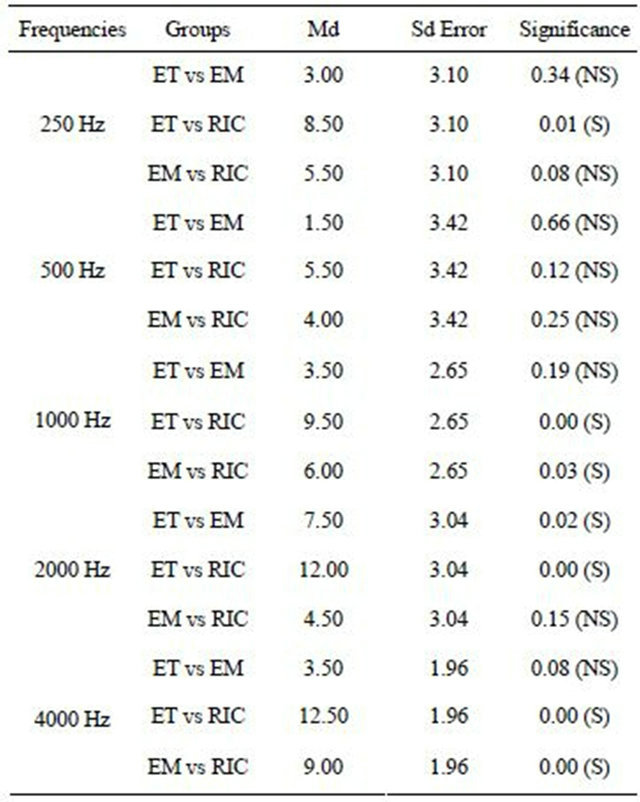
To explore all possible pair wise comparisons of means and to provide specific information on which aspects means are significantly different from each other data was subjected to Post-Hoc analysis between the fittings (i.e.) ear tip vs ear mould, ear tip vs Receiver in the canal, ear mold vs Receiver-In-Canal and the results reveal a significant difference in ear tip fitting vs ear mould fitting only at 2000 Hz and no significant difference at 250 Hz, 500 Hz, 1000 Hz and 4000 Hz. There is significant difference in ear tip vs Receiver-In-Canal at 250 Hz, 1000 Hz, 2000 Hz, 4000 Hz and no significant difference at 500 Hz; and also there is significant difference in ear mould vs Receiver-In-Canal at 250 Hz, 1000 Hz, 4000 Hz and no significant difference at 500 Hz, 2000 Hz indicating that Receiver-In-Canal fitting is significant better than ear tip and ear mould fitting in most conditions as shown in Tables 1 and 2.
4. Discussion
The functional gain scores at all frequencies were higher when individuals were fitted with digital hearing aids with Receiver-In-Canal as compared to with ear mould or ear tip, which can be attributed to better pinna effects due to the absence of ear moulds or ear tips. The results are in accordance with [16] who reported significantly higher satisfaction ratings of open-canal than non open canal hearing aids with regards to sound localization, quality of their own voice, phone comfort and appearance in experienced hearing aid users. It was also noted that the scores at 4 KHz was highest for Receiver-InCanal fitting. A study on the performance of open canal hearing instruments using probe microphone measurements also found maximum gain for the Receiver-InCanal instrument at 4 kHz and 6 KHz [20]. Placement of the receiver deep in the ear canal as in Receiver-In-Canal
Table 1. The significance between the groups and within the groups.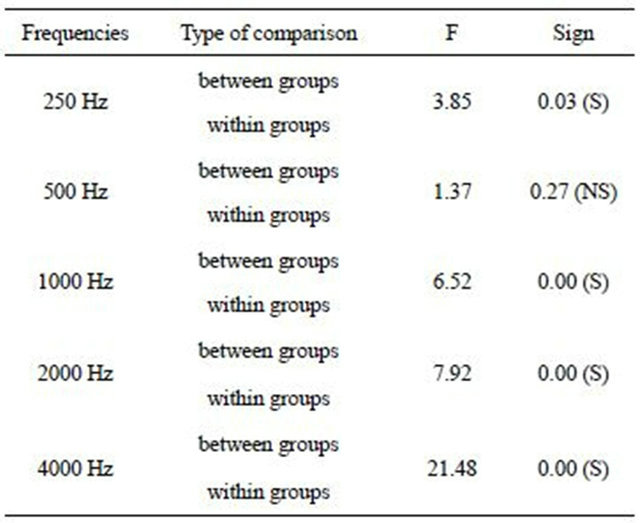
Table 2. Mean difference, standard error and significance across each condition.
fitting permits the individual to benefit from high frequency pinna effects that enhance front-back localization abilities [21-23].
The results also show that at low frequencies especially at 500 Hz there is no significant difference between all the three conditions which can be explained by the fact that Receiver-In-Canal hearing aids attenuate low frequency sounds automatically when the ear is left open (up to 30 dB less amplification at 500 Hz) especially for hearing in noisy situations [24].
These findings also suggest that open canal configurations are effective in minimizing the magnitude of the hearing aid occlusion effect and reportedly effective in reducing user perceptions of “hollowness” [25]. The improved quality of the user’s own voice is probably related to the expected reduction of the occlusion effect [26,27]. Others [15] also indicated significantly greater satisfaction with the open-ear canal device than with traditional fittings, such as the In-the-Ear hearing aids and suggested that open canal users were significantly more satisfied with the product aspects like comfort, visibility, size, clearness, feedback, reliability, appearance, noisy situations, expense, value, natural sounding, localization, and telephone usability, among others.
The findings also indicate that the use of functional gain measures as an effective tool for evaluating the performance of Receiver-In-Canal hearing aid fittings [20] in their study have also suggested that objective measures did not show any benefit however subjective measures did indicate aided benefit. During the verification stage of hearing aid the functional gain measure allows for one to check out the entire hearing aid and hearing mechanism and during this measurement feedback oscillations are not induced which are obtained often with high gain or deep-fitting hearing aids due to real-ear mic probe placement. It also helps in predicting the difficulty the patient might have when communicating in some specific environment when wearing hearing aid as it predicts the speech gain at low speech levels [28].
5. Conclusions
The results of this study on the Functional gain measures provide data base outside hearing aid companies, and were consistent with other studies, and suggest that open canal fittings are an effective means of overcoming one of the major barriers to the acceptance of amplification: poor own-voice sound quality resulting from the hearing aid occlusion effect The results can be used in the rehabilitation of hearing impaired individuals with moderately severe to severe SN hearing losses by providing hearing aids that will provide maximum benefit to them.
Traditional tube or behind-the-ear (BTE) fittings with ear moulds can alleviate occlusion and insertion loss, may be cosmetically unappealing and present feedback concerns due to the open feedback loop. The advantages of open canal hearing aids suggest that these devices are valuable for individuals in reduction or elimination of the occlusion effect, increased high frequency hearing, a more comfortable physical fit, and the relatively inconspicuous appearance with the potential to increase user satisfaction. Although the performance effects support recommendation of Receiver-In-Canal fittings, clinicians should still consider other factors while discussing options with individual patients. For instance, small ear canals may preclude the use of Receiver-In-Canal instruments because of retention, comfort or occlusion concerns. Every patient’s individual characteristics and concerns must be considered, but the potential benefits of Receiver-In-Canal instruments warrant further examination.
6. Acknowledgements
The authors would like to thank Prof. R. Rangasayee, Director, Dr. Geeta Mukundan, Deputy Director and other colleagues of AYJNIHH for their support for conducting the study. We would also like to thank all the subjects who participated in the study. We acknowledge Dr. S. Santhi Prakash, Reader in Spl. Education, AYJNIHH, SRC for helping us with statistical analysis.
REFERENCES
- H. G. Mueller, K. E. Bright and J. L. Northern, “Studies of the Hearing Aid Occlusion Effect,” Seminars in Hearing, Vol. 17, No. 1, 1996, pp. 21-32. doi:10.1055/s-0028-1089925
- F. Kuk and C. Ludvigsen, “Ampclusion Management 101: Understanding Variables,” Hearing Review, Vol. 9, No. 8, 2002, pp. 22-32. doi:10.1055/s-0028-1089925
- S. W. Painton, “Objective Measure of Low-Frequency Amplification Reduction in Canal Hearing Aids with Adaptive Circuitry,” Journal of the American Academy of Audiology, Vol. 4, No. 3, 1993, pp. 152-156.
- M. C. Killion, L. A. Wilber ans G. I. Gudmundsen, “A Potential Solution for the ‘Hollow Voice’ Problem (the Amplified Occlusion Effect) with Deeply Sealed Earmolds,” Hearing Instruments, Vol. 39, No. 1, 1988, pp. 14-18.
- H. G. Mueller, “Page Ten: There’s Less Talking in Barrels, but the Occlusion Effect is Still with Us,” Hearing Journal, Vol. 56, No. 8, 2003, pp. 10-16.
- D. J. MacKenzie, H. G. Mueller, T. A. Ricketts and D. F. Konkle, “The Hearing Aid Occlusion Effect: A Comparison of Two Measurement Devices,” Hearing Journal, Vol. 57, No. 9, 2004, pp. i30-i39.
- H. Dillon, G. Birtles and R. Lovegrove, “Measuring the Outcomes of a National Rehabilitation Program: Normative Data for the Client Oriented Scale of Improvement (COSI) and the Hearing Aid User’s Questionnaire (HAUQ),” Journal of the American Academy of Audiology, Vol. 10, No. 2, 1999, pp. 67-79.
- H. Dillon, “Hearing Aids: Hearing Aid Earmolds, Earshells, and Coupling Systems,” Boomerang Press, Sydney, 2001.
- J. Kiessling, S. Margolf-Hackl and S. Gellar, “Field Test of an Occlusion-Free Hearing Instrument,” GN ReSound White Paper, 2001.
- R. W. Sweetow and C. W. Pirzanski, “The Occlusion Effect and Ampclusion Effect,” Seminars in Hearing, Vol. 24, No. 4, 2003, pp. 333-344. doi:10.1055/s-2004-815549
- K. Durrer, “Critical Review: In Individuals with Sensorineural Hearing Loss, Are There Benefits of OpenCanal Hearing Aid Fittings Relative to Those of Traditional Fittings?” Candidate School of Communication Sciences and Disorders, 2008.
- D. Gnewikow and M. Moss, “Hearing Aid Outcomes with Openand ClosedCanal Fittings,” The Hearing Journal, Vol. 59, No. 11, 2006, pp. 66-72.
- H. G. Mueller and T. A. Ricketts, “Open-Canal Fittings: Ten Take Home Tips,” Hearing Journal, Vol. 59, No. 11, 2006, pp. 24-39.
- E. E. Johnson, “Segmenting Dispensers: Factors in Selecting Open-Canal Fittings,” Hearing Journal, Vol. 59, No. 11, 2006, pp. 58-64.
- L. Christensen and G. Matsui, “Hearing Aid Satisfaction with ReSound Air,” GN Resound White Paper, 2003.
- B. Taylor, “Real-World Satisfaction and Benefit with Open-Canal Fittings,” Hearing Journal, Vol. 59, No. 11, 2006, pp. 74-82.
- V. Parsa, “Acoustic Feedback and Its Reduction through Digital Signal Processing,” The Hearing Journal, Vol. 59, No. 11, 2006, pp. 16-23.
- American National Standards Institute, “Specifications for Pure Tone Audiometers (ANSI S 3.6-1969),” Author, New York, 1970.
- American Speech and Hearing Association, “Guidelines for Manual Pure-Tone Threshold Audiometery,” ASHA, Vol. 20, 1978, pp. 297-301.
- L. N. Alworth, P. N. Plyer, M. N. Rebert and P. M. Johnstone, “The Effect of Receiver Placement on Probe Microphone Performance and Subjective Measures with Open Canal Hearing Instruments,” Journal of the American Academy of Audiology, Vol. 21, No. 4, 2010, pp. 249- 266.
- T. S. Griffing and D. P. Preves, “In-the-Ear Aids, Part I,” Hearing Instruments, Vol. 27, No. 3, 1976, pp. 22-24.
- K. Chung, A. Neuman and M. Higgins, “Effects of InThe-Ear Microphone Directionality on Sound Direction Identification,” Journal of the Acoustical Society of America, Vol. 123, No. 4, 2005, pp. 2264-2275.
- T. Van den Bogaert, E. Carette and J. Wouters, “Sound Source Localization Using Hearing Aids with Microphones Placed Behind-The-Ear, in-the-Canal, and in-thePinna,” International Journal of Audiology, Vol. 50, No. 3, 2011, pp. 164-176.
- R. M. Cox and G. C. Alexander, “Acoustic versus Electronic Modifications of Hearing Aid Low Frequency Output,” Ear and Hearing, Vol. 4, No. 4, 1983, pp. 190-196. doi:10.1097/00003446-198307000-00003
- W. Otto, “Evaluation of an Open Canal Hearing Aid by Experienced Users,” Hearing Journal, Vol. 58, No. 8, 2005, pp. 26-32.
- F. Kuk, M. Keenan and C. Ludvigsen, “Efficacy of an Open-Fitting Hearing Aid,” Hearing Review, Vol. 12, No. 2, 2005, pp. 26-32.
- J. Kiessling, B. Brenner, C. T. Jespersen, et al., “Occlusion Effect of Earmolds with Different Venting Systems,” Journal of the American Academy of Audiology, Vol. 16, No. 4, 2005, pp. 237-249. doi:10.3766/jaaa.16.4.5
- D. Hawkins, “Limitations and Uses of Aided Audiogram,” Seminars in Hearing, Vol. 25, No. 1, 2004, pp. 51-62. doi:10.1055/s-2004-823047